
Abstract
Tall Cell Carcinoma with Reversed Polarity (TCCRP) is a rare type of invasive breast cancer. Most available literature focuses on histopathology and gene-sequencing, while few studies offer insights into clinical management. This report provides a comprehensive review of available literature including 2 new clinical cases to offer insights into the diagnosis, treatment, and outcomes of TCCRP. A systematic literature review was conducted using PubMed with collation of all cases with appropriate clinicopathologic data available. Two TCCRP cases with complete clinicopathologic data were identified at our institution and included in the analysis. Clinical, radiographic, and pathological characteristics were analyzed. Literature review identified 46 relevant studies, with 88 prior cases reported. Data was extracted from 14 studies with complete data, and 67 unique cases analyzed. All patients were female, with a median age of 62 (40-85). Clinical data included tumor size, receptor status, surgery management, adjuvant therapy, recurrence, and overall survival. Most cases demonstrate triple-negative status, yet almost all cases behave indolently with excellent prognosis after surgery and little/no adjuvant therapy. Improved understanding of the clinical behavior of this disease will promote appropriate management and avoid overtreatment.
Keywords
Introduction
Tall Cell Carcinoma with Reversed Polarity (TCCRP) is a rare type of invasive breast cancer, first reported in 2003 by Eusebi et al and officially designated by the WHO as a distinct entity in 2019.1,2 Its resemblance to the tall cell variant of papillary thyroid carcinoma, from which its name is derived, initially raised the possibility this cancer was a thyroid carcinoma metastatic to the breast. However, TCCRP tumors do not express thyroid-specific tumor markers (thyroglobulin and TTF1) or the common molecular alterations in papillary thyroid cancers. 3
To our knowledge, 88 unique cases have since been reported in the literature, as well as 2 additional cases identified at our institution. Most of these tumors demonstrate triple-negative receptor status, yet behave indolently, with small size at diagnosis, negative lymph nodes, and excellent response to treatment. As such, most surgeons are unlikely to have encountered this disease, and appropriate treatment does not follow the usual paradigm for triple-negative breast cancer. Moreover, most available literature to date is found in molecular pathology focused journals, with a particular focus on histopathological features and gene-sequencing results, while few studies offer insights into clinical management. This report provides a comprehensive review of available literature on TCCRP clinical data to offer useful insights into TCCRP diagnosis, treatment, and outcomes.
Methods
Summary of Clinical Data of all Reported TCCRP Cases.
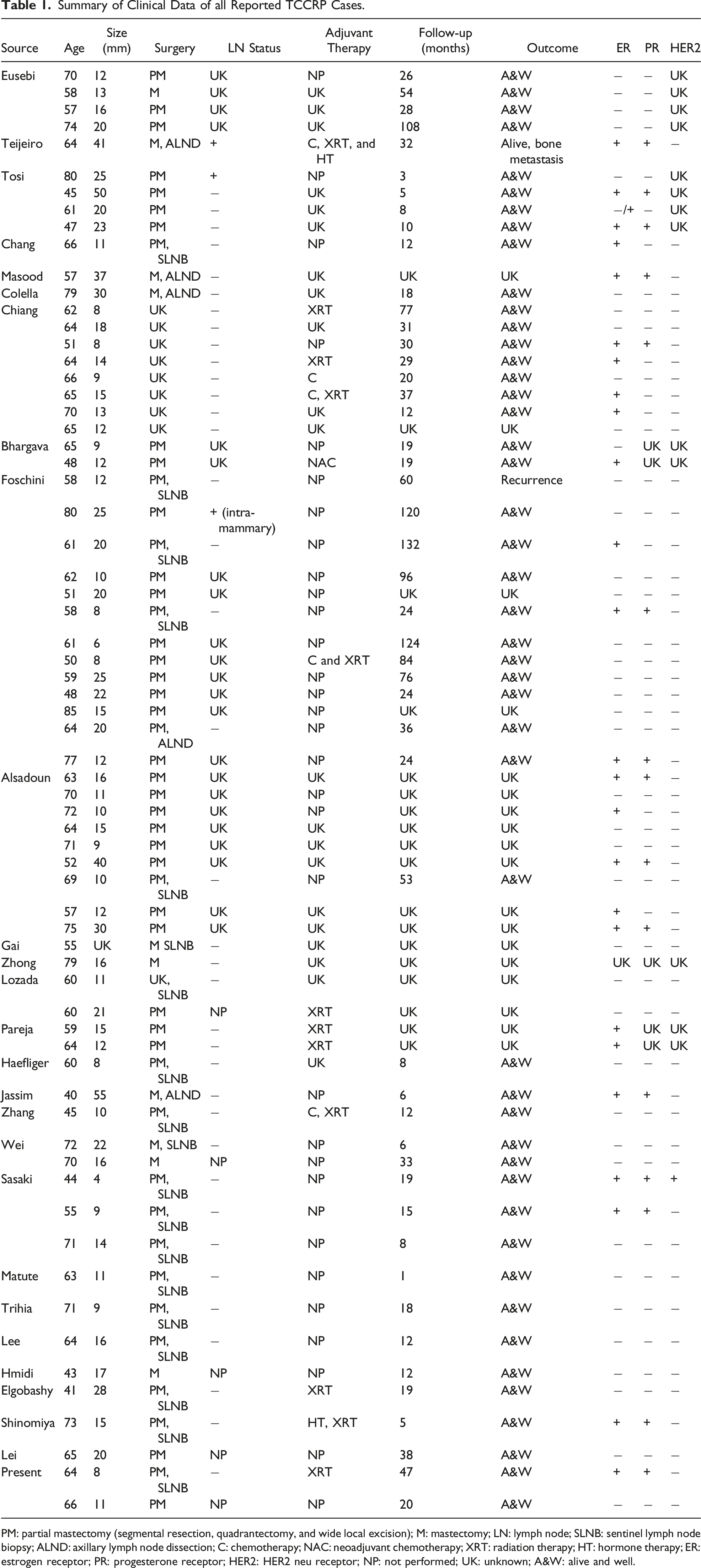
PM: partial mastectomy (segmental resection, quadrantectomy, and wide local excision); M: mastectomy; LN: lymph node; SLNB: sentinel lymph node biopsy; ALND: axillary lymph node dissection; C: chemotherapy; NAC: neoadjuvant chemotherapy; XRT: radiation therapy; HT: hormone therapy; ER: estrogen receptor; PR: progesterone receptor; HER2: HER2 neu receptor; NP: not performed; UK: unknown; A&W: alive and well.
Results
Summary of Clinical Data From 67 Cases of TCCRP.
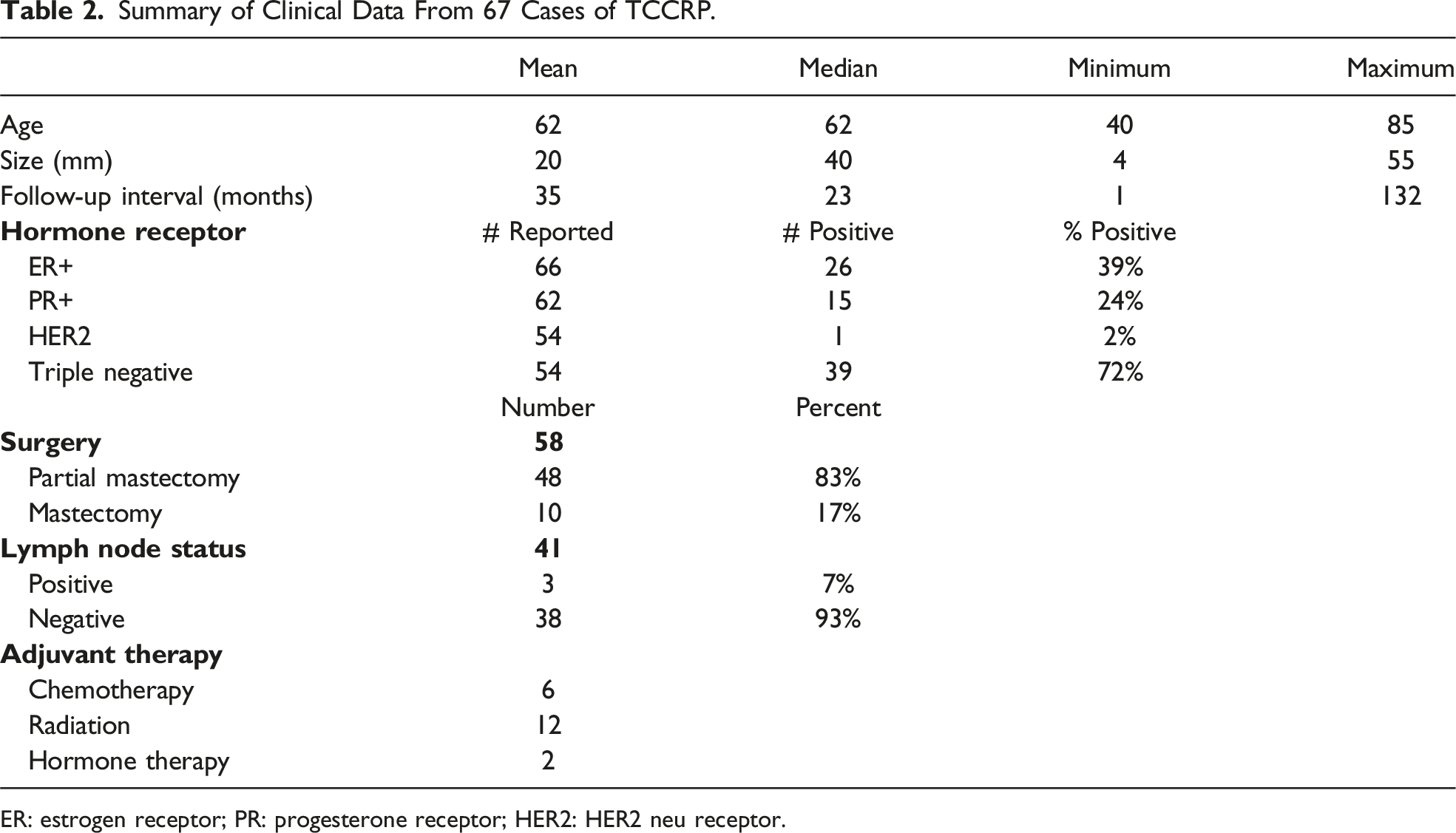
ER: estrogen receptor; PR: progesterone receptor; HER2: HER2 neu receptor.
Discussion
Tall Cell Carcinoma with Reversed Polarity appears to affect predominantly older women and presents as a small tumor with minimal risk of nodal metastasis. 4 of the cases specifically mention that nodal sampling was omitted, and all 4 patients were alive and well without complications or recurrences at their interval follow-up.4-6 Of the patients with reported nodal status, 93% were node-negative.2-4,7-24 Of the 3 patients found with nodal metastases, the first patient underwent partial mastectomy for a 25 mm tumor with an intra-mammary lymph node identified in the specimen, the second patient underwent a partial mastectomy for a 25 mm tumor with a positive sentinel node, and the third patient underwent a modified radical mastectomy for a 41 mm tumor with several positive lymph nodes. These 3 cases give credence to the concept of possible nodal evaluation if the local tumor is greater than 2 cm. The first 2 patients are alive and well at reported interval follow-up, while the third patient developed bone metastases and is reportedly still living.3,7,25 This third patient is the only patient to have distant metastasis in the case review. Notably, the review by Barghava et al of the third patient noted that the histopathology in that case suggests the features may be more similar to a typical ER+/PR+ breast cancer rather than true TCCRP. 26 Considering such minimal risk of nodal disease and negligible metastatic disease, it may be reasonable to omit lymph node sampling in clinically node negative patients with tumors smaller than 2 cm, and complete axillary dissection is likely unwarranted.
Regarding surgical choice, most cases underwent partial mastectomy. It is important to note that 28 patients who underwent partial mastectomy did not receive postoperative radiation therapy, as would typically be the standard for breast-conserving therapy, and 27 of these patients were alive and well at interval follow-up without local recurrence.1-3,6-8,12,20-22,26 One patient did experience local and axillary recurrent disease, which was surgically removed without further treatment or recurrence. 3
Not all cases with relevant clinical data reported receptor statuses. However, for those studies reporting receptor status, a predilection for triple-negative disease (72%) in TCCRP seems apparent. These cases all behaved indolently, and the majority did not receive neoadjuvant or adjuvant therapy.2-6,12,20-22 Only 2 patients with ER+ disease received adjuvant hormone therapy; none of the patients with ER+ disease who omitted hormone therapy experienced recurrent disease.3,8,11,12,16,18,20,24-26 Given the usual aggressive behavior of triple-negative invasive mammary carcinoma, and subsequent aggressive approach to treatment, it is important for physicians to recognize TCCRP as a distinct clinical entity, so that overtreatment can be avoided.
The unique histologic appearance of tall cell carcinoma with reverse polarity features circumscribed nests of epithelial cells which contain delicate fibrovascular cores (Figure 1A). The nests are composed of columnar epithelial cells with abundant eosinophilic cytoplasm and reversed polarity of the nuclei, with the nuclei at the apical rather than basal poles of the tumor cells. A dense fibroma surrounds the tumor nests. The tumor cell nuclei are bland, round to ovoid, and scattered cells contain nuclear grooves and intra-nuclear cytoplasmic inclusions (Figure 1B). Although most cases have a triple-negative phenotype (negative for estrogen, receptors, progesterone, receptors, and HER2), mitotic figures are rare and the Ki67 index is low. Immunohistochemical stains show the tumor cells are positive for CK5/6 (Figure 1C) while lacking p63-expressing basal myoepithelial cells (Figure 1D) surrounding the tumor nests. (A) TCCRP composed of circumscribed nests of epithelial cells which contain delicate fibrovascular cores and are surrounded by dense fibroma. (B) TCCRP is composed of columnar epithelial cells with abundant eosinophilic cytoplasm and reversed polarity of the nuclei with the nuclei at the apical rather than basal poles of the tumor cells. The tumor cell nuclei are bland, round to ovoid, and scattered cells contain nuclear grooves and intra-nuclear cytoplasmic inclusions. (C) Tumor cells are strongly positive for CK5/6. (D) Tumor cell nests lack p63-expressing basal myoepithelial cells.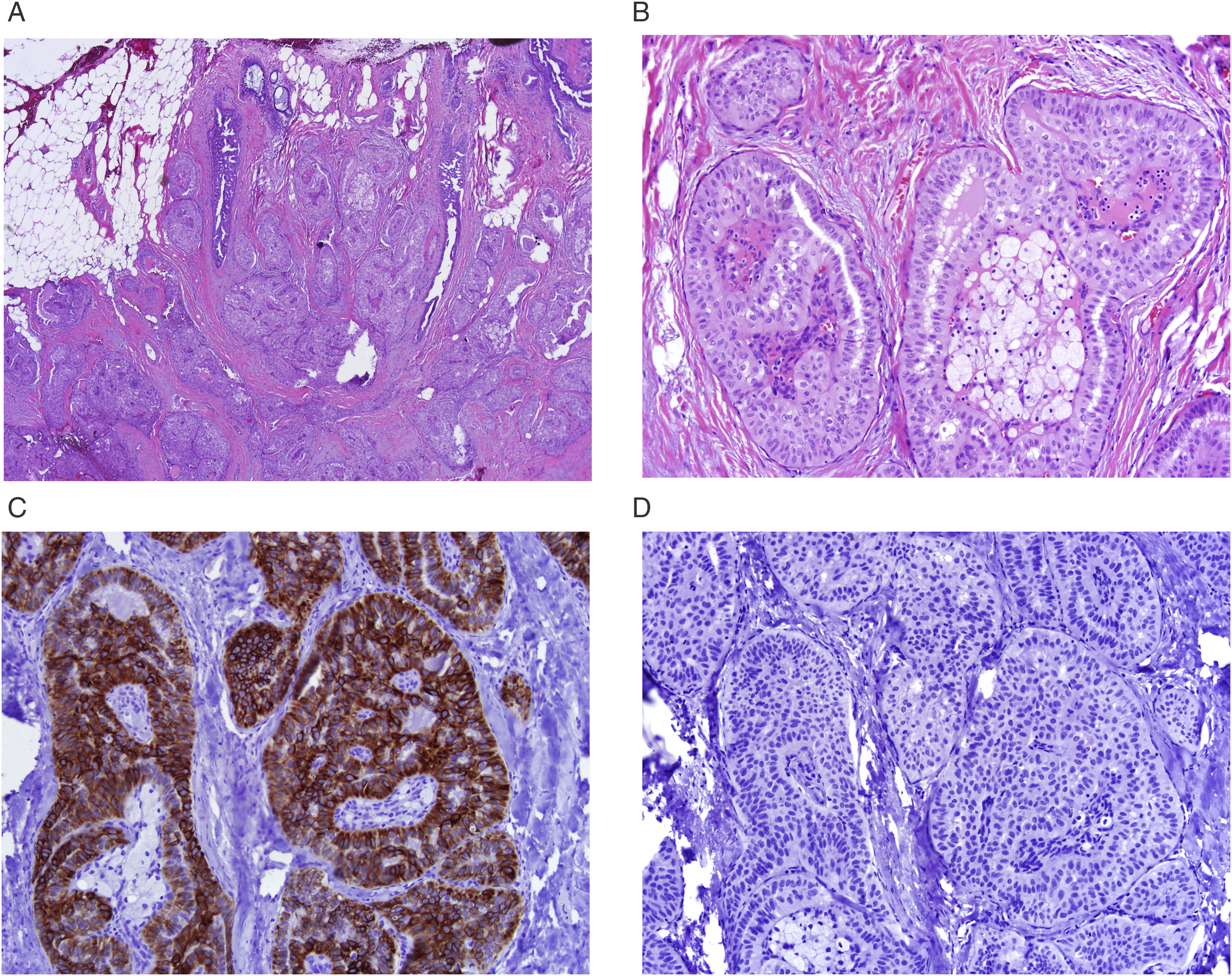
Tall Cell Carcinoma with Reversed Polarity is a rare clinical entity with little available clinical data to guide management. Most cases demonstrate triple-negative receptor status, yet almost all cases behave indolently with excellent prognosis after surgery and with little benefit from adjuvant therapy. This review offers a thorough interpretation of all reported clinical cases to date, to improve understanding of the clinical behavior of this disease, promote appropriate management, and avoid overtreatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.