
Abstract
Keywords
Key Takeaways
• Thromboembolism is a feared complication of thrombectomy. • The Protrieve sheath offers temporary embolic protection during thrombectomy. • Manipulation of the sheath intraoperatively can cause lapses in embolic protection. • The Protrieve sheath should be sutured to the skin to prevent migration intraoperatively.
Background
Deep vein thrombosis (DVT) is a common vascular condition associated with significant morbidity and mortality. Iliocaval DVTs can develop from both acute and chronic etiologies. Acute DVTs form as a result of Virchow’s triad, which consists of hypercoagulability, stasis, and endothelial injury. Chronic DVTs can also form in the setting of anatomic abnormalities, such as May-Thurner Syndrome or other forms of venous compression.1–3 Additionally, inferior vena cava (IVC) DVT etiologies can be iatrogenic from the prolonged use of IVC filters. 4 Due to the proximal location and involvement of major venous structures, iliocaval and IVC DVTs have been treated with both therapeutic anticoagulation and surgical intervention, given the increased risk of thromboembolism.5–7 Anticoagulation can prevent thrombus propagation. However, up to 40% of patients may fail anticoagulation and experience clot propagation. Furthermore, anticoagulation lacks the thrombolytic activity to hasten thrombus resolution. 8 Therefore, it does not mitigate the immediate risk associated with the thrombus, such as pulmonary embolism (PE), leg swelling, and phlegmasia. Persistent thrombus also has long-term risks including post-thrombotic syndrome and chronic venous insufficiency. Current guidelines for operative interventions for both iliocaval and IVC DVTs include minimally invasive endovascular thrombectomy.4,9,10
Endovascular intervention via mechanical or aspiration thrombectomy has complication rates of 3-5% for DVTs.3,5–8,11–14 Given the high efficacy with minimal exclusion criteria, multiple thrombectomy systems have been developed and utilized over the past decade. Recent technological advances include the ClotTriever and FlowTriever systems (Inari Medical, Irvine, California), Penumbra system, AngioJet, AngioVac, and Jet-I, which are effective and successful in the treatment of occlusive iliocaval DVTs.15,16 Published literature shows patency rates over 90% after treatment of DVTs using the ClotTriever device at 12 months. 17 However, there was still a risk of thromboembolic complications as prior devices did not include embolic protection mechanisms. To mitigate the risk of thromboembolism during thrombectomy procedures, temporary IVC filter placement has been used with a reported IVC thrombus capture of 31%. 18 However, while they can reduce the risk of thromboembolism during the procedure, there are associated risks of filter migration, caval perforation, and the need for an additional procedure for retrieval of the filter.4,10 Furthermore, IVC filters reduce the risk of large PEs, but smaller emboli can get through the fenestrations. Other techniques include using balloon occlusion and aspiration to temporarily halt flow during clot manipulation; however, it can be technically challenging to employ this technique, and studies have not been done on its effectiveness in preventing PE.
The Protrieve sheath (Inari Medical, Irvine, California) is a novel complement to the preexisting ClotTriever and FlowTriever systems and offers temporary embolic protection during thrombectomy. Through the sheath, an expandable 33.5 mm nitinol mesh funnel is deployed with IVC apposition, allowing the capture of thromboemboli that may become dislodged during the thrombectomy procedure and decrease the risk of PE. Unlike temporary IVC filters, it can be deployed and removed during the same procedure and does not have the associated risks of IVC filter placement. Furthermore, it has smaller fenestrations, allowing for the capture of smaller emboli. Prior case reports demonstrate the feasibility of the Protrieve sheath during iliocaval thrombectomy.19,20 However, these studies contained only a handful of patients, resulting in a paucity of data on the safety profile, efficacy, and effectiveness of the device. The purpose of this study is to evaluate the effectiveness of the Inari Protrieve sheath at preventing PE following iliocaval and IVC thrombectomy as well as assess the learning curve for the technical and operative skills needed.
Methods
Study Population
This is a multicenter retrospective observational study involving data from two medical institutions. IRB approval was obtained at both institutions. The study included thirteen adult patients 18 years or older with acute IVC or iliocaval DVT who underwent mechanical thrombectomy with embolic protection using the Protrieve sheath (Inari Medical, Irvine, California) between September 2022 and July 2023. Thrombectomy was performed by vascular surgery or Interventional Radiology. Patient characteristics, including age, sex, comorbidities, radiographic and procedural details, and active medications, were collected.
Primary and Secondary Outcomes
The primary outcome was postoperative embolic events, specifically PE, which were identified by computed tomography (CT) scans. Computed tomography scans were only obtained if patients were symptomatic. Secondary outcomes included technical success, perioperative complications, including mortality, stroke, myocardial infarction, and recurrent DVT at 30 days, and patency at 3 and 6 months. Technical success was defined as thrombus clearance of over 70% and restoration of patent venous flow. 16 Venous patency at follow-up was defined as a patent IVC and bilateral iliac veins on follow-up CT venogram or normal compressibility on venous duplex ultrasound. Data was retrospectively collected by providers at each medical center via the electronic medical record.
Devices
The Protrieve system consists of a 26F outer diameter sheath with a 20F inner diameter. It utilizes a 33.5 mm self-expanding nitinol mesh funnel that creates full apposition of the IVC. The ClotTriever mechanical thrombectomy system includes a nitinol coring catheter with a braided collection bag and a 13F or 16F sheath with a self-expanding nitinol funnel. The FlowTriever suction thrombectomy system includes various sizes of three self-expanding nitinol mesh disks to disrupt the clot from vessel walls and a large bore suction catheter (16F, 20F, or 24F) to remove the dislodged clot. All three systems are used over a 0.035” guidewire.
Technique
Patients were brought to the angiogram suite and positioned supine. Entry into the right internal jugular (IJ) vein was achieved under ultrasound guidance with a micropuncture kit. A Glide or Glide Advantage wire (Terumo Interventional Systems, Somerset, New Jersey) was inserted followed by serial dilation via the Seldinger technique up to 26F. If a prior IVC filter was present, filter removal was attempted first. In cases where filters were not able to be removed safely, the Protrieve funnel was placed immediately proximal to the prior IVC filter. Only the FlowTriever system was used to traverse the embedded IVC filter due to the risk of entanglement with the ClotTriever system. Next, the Protrieve device was advanced over the wire to the suprarenal IVC below the level of the heart. The position was confirmed with fluoroscopy and the funnel was deployed. Systemic heparin was given, and activated clotting time was confirmed to be between 250 and 300 s. Venograms were performed to identify the iliocaval thrombosis. ClotTriever and/or FlowTriever systems were then used to perform the mechanical thrombectomy. When applicable, balloon angioplasty and stent placement were used to treat venous stenoses. Intravenous ultrasound (IVUS) and completion venograms were used to confirm venous patency. Once technical success was achieved, the Protrieve funnel was aspirated to remove any emboli that had become dislodged and were captured by the funnel. Finally, the Protrieve sheath was collapsed and removed at the conclusion of the case. Manual pressure was held, and a dressing was placed.
Results
A total of thirteen patients underwent thrombectomy with the Inari FlowTriever or ClotTriever with Protrieve sheath placement. Ten patients (76.9%) underwent thrombectomy with vascular surgery and three (23.1%) with interventional radiology. The median age was 55 (IQR 43-60), and 61.5% were men.
Patient Demographics and Venous Thrombus Extent.
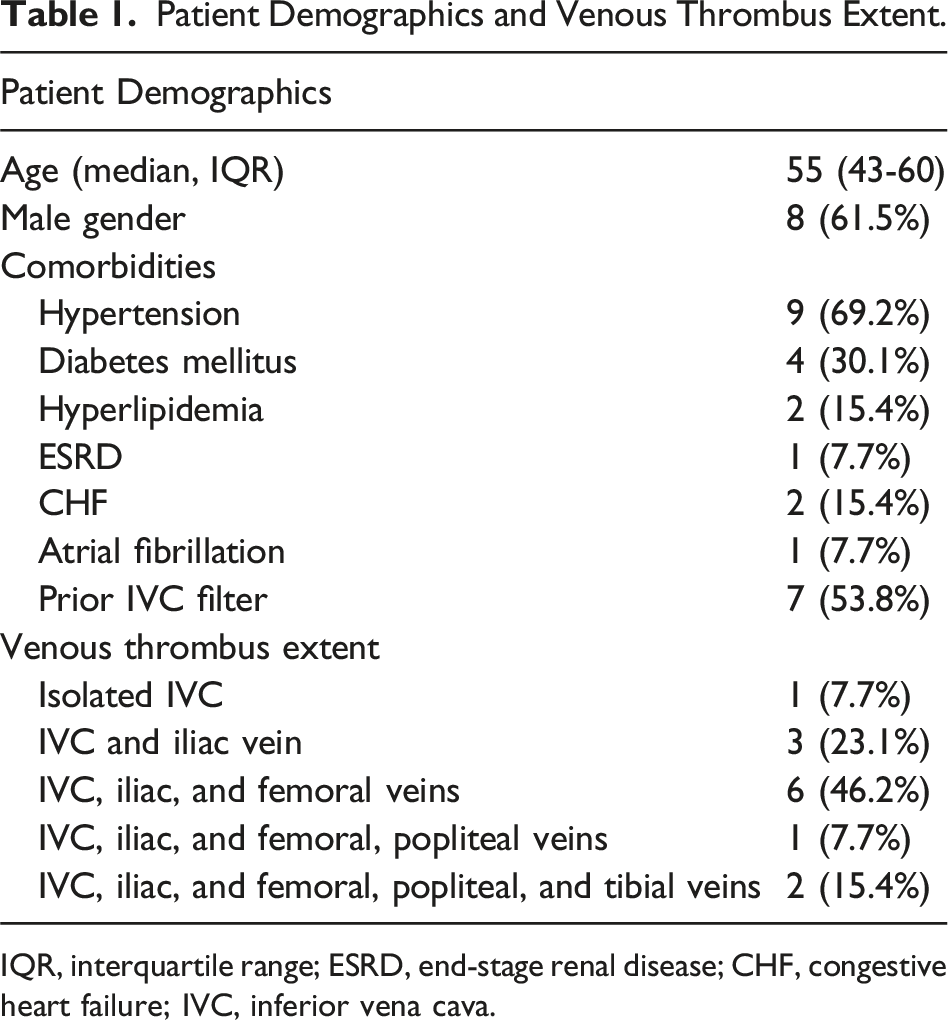
IQR, interquartile range; ESRD, end-stage renal disease; CHF, congestive heart failure; IVC, inferior vena cava.
All thirteen patients had technical success of thrombus removal. Among the seven patients with IVC filters, successful IVC filter retrieval was achieved in five of the seven patients (71.4%). These included patients with thrombus involving (1) the IVC with bilateral iliofemoral, popliteal, and tibial veins; (2) bilateral iliofemoral veins; (3) the IVC and bilateral common iliac veins; (4) the IVC and right lower extremity deep venous system; and (5) the IVC with bilateral popliteal vein involvement. In the two remaining patients, IVC filters could not be safely removed. One of these patients had extensive thrombus involving the IVC, left common and external iliac veins, femoral, popliteal, and tibial veins, while the other had thrombus extending from the right iliac vein into the femoral and popliteal veins. Two patients (15.4%) developed postoperative subsegmental PE. Initially, the first patient was treated for extensive thrombus involving the IVC, left common and external iliac veins, femoral, popliteal, and tibial veins. The second patient was initially treated for thrombus limited to the bilateral iliofemoral veins. Three patients (23.1%) required placement of an IVC filter due to either a contraindication to anticoagulation or hypercoagulability refractory to anticoagulation. Of those three patients who required IVC filter placement, two were placed for recurrent thrombus despite therapeutic anticoagulation, and one was placed due to a contraindication to anticoagulation due to recent spine surgery. Five patients (38.5%) required venous stenting.
The median hospital length of stay was nine days (IQR 5-13). All patients were discharged on therapeutic anticoagulation. Additionally, five patients were also discharged on antiplatelet therapy.
Patient Outcomes, Complications, and Long-Term Patency.
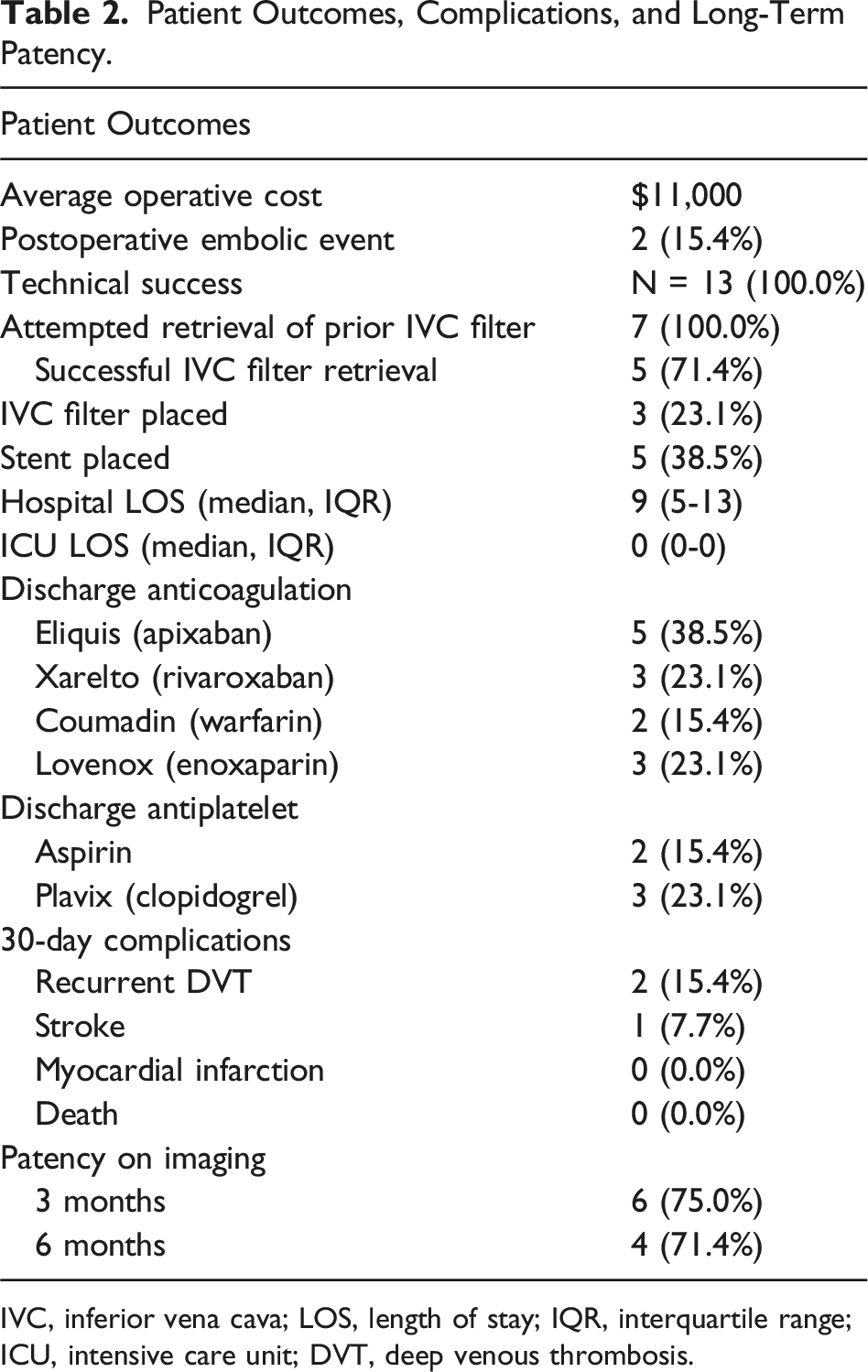
IVC, inferior vena cava; LOS, length of stay; IQR, interquartile range; ICU, intensive care unit; DVT, deep venous thrombosis.
Patient Characteristics, Procedural Details, and Outcomes for Protrieve-Assisted Thrombectomy.
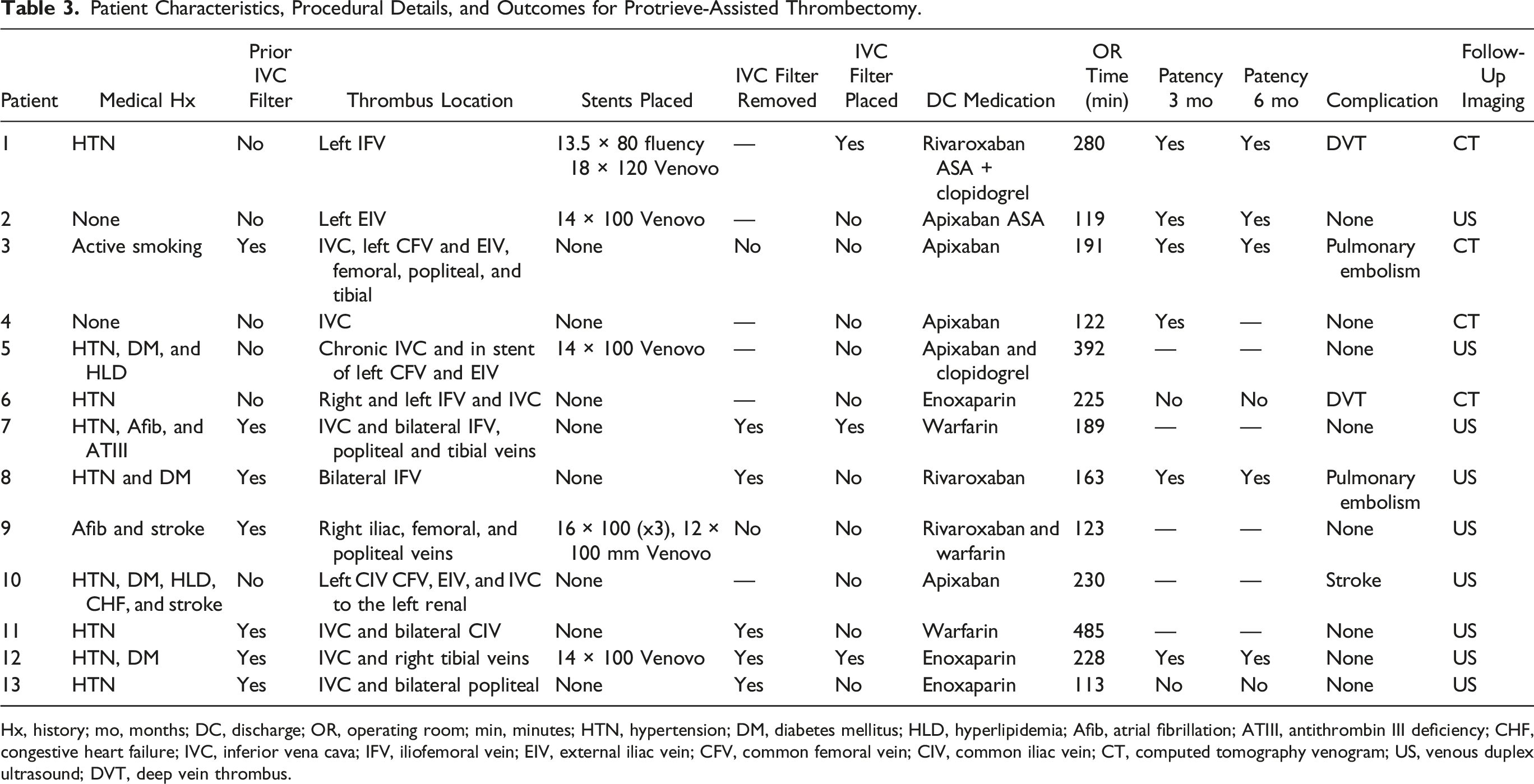
Hx, history; mo, months; DC, discharge; OR, operating room; min, minutes; HTN, hypertension; DM, diabetes mellitus; HLD, hyperlipidemia; Afib, atrial fibrillation; ATIII, antithrombin III deficiency; CHF, congestive heart failure; IVC, inferior vena cava; IFV, iliofemoral vein; EIV, external iliac vein; CFV, common femoral vein; CIV, common iliac vein; CT, computed tomography venogram; US, venous duplex ultrasound; DVT, deep vein thrombus.
Discussion
IVC filters are typically used for critically ill patients, including those with malignancies, who are at risk for PE and have contraindications to or failure of therapeutic anticoagulation. The use of temporary IVC filters to mitigate PE has grown in popularity over the past few years.18,21 Over 85% of IVC filters were placed with temporary intent and should have been removed once the patient is able to tolerate anticoagulation or the risk of PE has subsided. However, only 20-35% of them are successfully retrieved.22,23 Inferior vena cava filters have increased risks associated with prolonged use, including migration to the heart or lungs, filter fractures and embolization, IVC thrombosis or occlusion with extension to the lower extremities, and rarely IVC perforation.4,10,24 With the increasing prevalence of IVC filters that have not been removed, we are likely to see an increase in patients with IVC filter-associated DVT. To safely treat these patients, an embolic protection device will need to be used during the thrombectomy procedure.
Mechanical thrombectomy has been shown to be an effective treatment for DVTs.3,5–8,11–14 Due to its high efficacy, endovascular approach, and minimal exclusion criteria, multiple thrombectomy systems have been developed for improved outcomes. Newer commercially available mechanical thrombectomy devices include the ClotTriever and FlowTriever systems, which have been shown to successfully treat occlusive DVTs.15,16 However, these devices do not protect the patient if a clot embolism occurs. For patients at a high risk of thromboembolism during mechanical thrombectomy, temporary IVC filters have been used to prevent PE, as they have been shown to reduce the rate of new PE events from 11.3% to 1.4%. 25 However, the use of a temporary IVC filter requires an additional procedure after the thrombectomy procedure to remove it, along with the risks of IVC filter placement mentioned previously. The Protrieve sheath (Inari Medical, Irvine, California) is a novel complement to the preexisting ClotTriever and FlowTriever systems, as it offers temporary embolic protection during thrombectomy and can be removed at the conclusion of the procedure. There is a paucity in the current literature regarding the use of this device for complex iliocaval and IVC filter thrombosis. In this study, we discuss our results as well as the learning curve of using the Inari Protrieve sheath and how our practice evolved to mitigate future embolic complications.
There are limited studies that demonstrate the use of mechanical thrombectomy to treat iliocaval DVTs and IVC filter thrombosis. A large portion of the published data supporting ClotTriever is derived from the CLOUT registry, which demonstrates a success rate of over 90% for iliofemoral venous thrombosis. 26 The data for IVC thrombus is more variable. A collection of case series showed success rates between 70 and 90% for mechanical thrombectomy of IVC thrombus.15,16 This study is consistent with the literature with all of our patients having a successful immediate postoperative outcome. The CLOUT registry shows an 80% patency rate at 6 months. This study also demonstrates similar long-term outcomes comparable to the current CLOUT registry 26 75% at 3 months and 71% at 6 months. This discrepancy is likely due to the smaller sample size.
When reviewing the cases in this study, we analyzed the surgical treatment of complex DVTs that required innovation in technique. Routinely, we attempted thrombectomy through the right IJ access site in the supine position. In cases with completely occluded iliocaval DVTs, which were unable to be transversed with smaller caliber wires, a retrograde approach from the popliteal vein was used. This approach required the patient to be repositioned prone, with care taken to not dislodge the Protrieve sheath. Retrograde wires could be snared via the right IJ access site and externalized. Thrombectomy was then performed via either access site.
We also encountered cases with extensive iliocaval DVTs with extension into the femoral and popliteal veins. These were challenging to treat with thrombectomy due to the length limitations of the ClotTriever and FlowTriever systems. In these cases, additional access sites at the contralateral common femoral vein or ipsilateral popliteal vein were used.
This study contains a comparable recurrent DVT rate to that of prior literature at 15%. 15 The first patient in this study with recurrent DVT had a history of antithrombin III deficiency and antiphospholipid syndrome on therapeutic warfarin. The second patient with recurrent DVT had a history of advanced metastatic esophageal adenocarcinoma with intermittent gastrointestinal bleeding while on anticoagulation. Both patients with recurrent DVTs had underlying hypercoagulable conditions that required an IVC filter and subsequently developed an IVC filter-associated thrombosis. Subsequently, both patients underwent repeat Protrieve sheath placement, successful removal of their IVC filter with forceps, and repeat thrombectomy with the ClotTriever system with no subsequent recurrence of their DVT.
Literature describing the Protrieve embolic protection sheath is from case reports, which demonstrated feasibility and ease of use in conjunction with Inari thrombectomy devices for treating IVC thrombus.19,20 A prior case series using the ClotTriever device and an IVC filter present demonstrated a PE rate of 13%. This study is comparable with a PE rate of 15%, which we attribute to the initial learning curve associated with the Protrieve sheath.
The embolic events occurred during our initial cases and prompted a refinement in our technique to mitigate future complications. We hypothesized that the embolic events occurred due to intraoperative mechanical adjustment of the Protrieve sheath. The sheath has a hydrophilic coating, which makes it prone to sliding. The sliding action likely disrupted the caval wall apposition and sheath migration. In these cases, the funnel would have to be collapsed in order to be repositioned, which would also lead to a disruption of embolic protection. To address this, in all subsequent cases, our protocol evolved, and we secured the Protrieve sheath to the skin using sutures to prevent migration and preserve continuous embolic protection.
The second PE is suspected to have occurred during the removal of the Protrieve sheath in exchange for a CavaClear (Philips, Andover, Massachusetts) laser sheath for IVC filter removal. Unfortunately, due to length limitations, the CavaClear system was unable to be telescoped through the Protrieve sheath and required device exchange over the wire. Removal of the IVC filter without proximal embolic protection likely led to embolic showering, causing the subsegmental PE. This case underscored the critical importance of maintaining continuous embolic protection throughout the entirety of the procedure. In response, we revised our protocol to minimize any lapses in protection, incorporating strategies such as dual venous access to allow for uninterrupted Protrieve deployment, even during device exchanges.
While our early experience demonstrates that the Protrieve sheath provides embolic protection during mechanical thrombectomy, cost may limit its use in resource-limited settings or in cases where embolic risk is perceived to be low. Costs, however, may vary significantly depending on the hospital’s payer mix, billing practices, and reimbursement models, such as private insurance, Medicare, or bundled payment systems. However, using IVC filters for embolic protection during mechanical thrombectomy procedures also has associated costs with the mean costs of IVC placements being over $5000 and retrievals costing over $2,000, 27 with the average margin being −$1706.18. 28 Other potential barriers to broader implementation include institutional cost-containment policies, lack of reimbursement, and the learning curve associated with device usage.
Limitations
The limitations of this study include a retrospective design. We also had a small sample size; therefore, our findings may not be representative of the overall population. Due to the retrospective nature of this study, there was a lack of controls. Propensity matching to patients that underwent mechanical thrombectomy without an embolic protection sheath was not performed. Additionally, as only symptomatic patients were assessed for PE, we were unable to determine definitively that the patients who did not have further imaging did not develop subclinical embolisms. Moreover, quantifiable data on the amount of emboli captured by the Protrieve sheath was also not consistently available in operative dictations, limiting the conclusions we could draw on the ability of the sheath to protect against large clot burdens. This study also had limited long-term follow-up to demonstrate continued patency without development of post-thrombotic syndrome. Larger studies are needed to validate these results and determine the efficacy of the Inari Protrieve sheath.
Conclusion
The use of the Inari Protrieve sheath can mitigate the risk of PE when attempting to remove thrombus from the IVC or iliofemoral veins. Due to the hydrophilic coating of the shaft of the sheath, periprocedural migration can occur. Repositioning of the sheath and funnel results in lapses of embolic protection. We recommend firmly securing the sheath at the skin insertion site with 0-silk suture to prevent periprocedural migration.
Footnotes
Authors’ Note
Presentation Information: Early Experience using Venous Sheath with Embolic Protection during Thrombectomy of Inferior Vena Cava and Complex Iliofemoral Deep Vein Thrombosis. 2025 Annual Scientific Meeting of the Southern CA Chapter of the American College of Surgeons. Santa Barbara, California. 2025.
Author Contributions
Mennatalla Hegazi, MD—writing original draft preparation and reviewing/editing. Peter Nguyen, MD—writing original draft preparation. Nii-Kabu Kabutey, MD—supervision and writing: review/editing. Isabella Kuo, MD—writing: review/editing. Samuel Chen, MD—writing: review/editing. Sheela Patel, MD—writing: review/editing. Roy M Fujitani, MD—supervision and writing: review/editing. Anthony Chau, MD—supervision and writing: review/editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anthony Chau: Consultant for Inari.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data sets generated during the current study are not available publicly as it contains de-identified patient information.