
Abstract
Background
Previous single-center reports have demonstrated a longer time from traumatic leg injury to fasciotomy in pediatric trauma patients (PTPs) with compartment syndrome. We hypothesized most fasciotomies in isolated pediatric lower extremity trauma (LET) are delayed (
Methods
The 2017-2020 TQIP database was queried for PTPs
Results
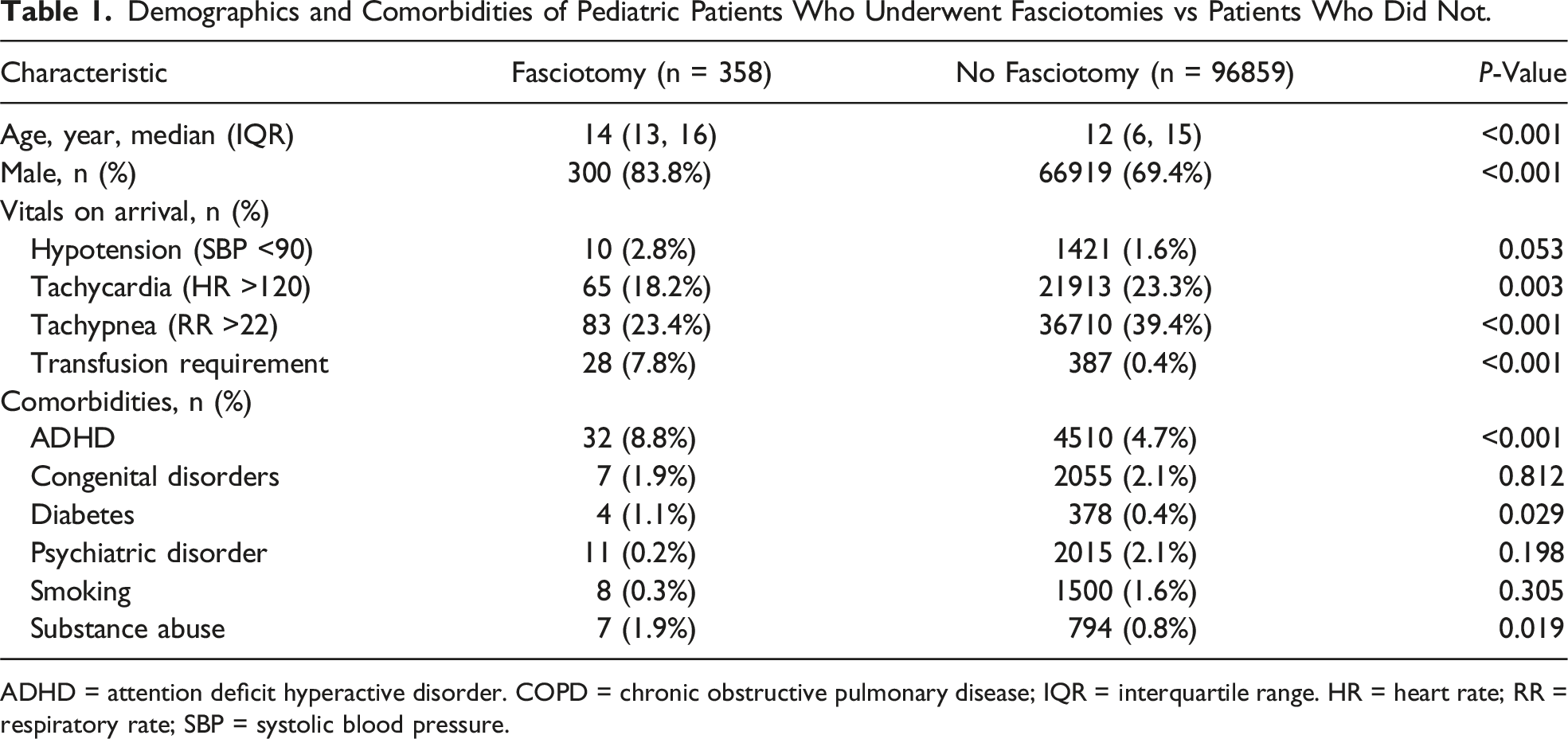
From 97,217 PTPs, 358 (0.4%) underwent a fasciotomy, with a majority being delayed (60.3%); the median time to fasciotomy was 9.6 hours. Patients undergoing fasciotomy were older (median age 14 vs 12 years, P < 0.001), had a higher rate of severe LET (4.9% vs 1.2%, P < 0.001), and had tibial fracture (70.7% vs 27.6%, P < 0.001). They also had increased rates of in-hospital complications (14.2% vs 0.6%, P < 0.001), limb loss (1.1% vs <0.1%, P < 0.001), and longer median length of stay (LOS) (5 vs 2 days, P < 0.001). The most injured vessel in those undergoing fasciotomy was the popliteal artery (9.9%). Independent risk factors associated with fasciotomy included injuries to the popliteal vein (OR 30.72, CI 11.06-85.29, P < 0.001), femoral vein (OR 18.19, CI 6.40-51.69, P < 0.001), and popliteal artery (OR 13.74, CI 8.45-22.34, P < 0.001) and tibial fracture (OR 7.46, CI 5.57-10.00, P < 0.001).
Discussion
Most fasciotomies were delayed for PTPs with isolated lower extremity injury. Popliteal vein injury increases the risk for fasciotomy 30-fold. Patients undergoing fasciotomy tend to have more complications and longer LOS.
Key Takeaways
• Most fasciotomies occur in a delayed fashion for pediatric trauma patients. • Popliteal vein injury increases the risk for fasciotomy 30-fold in pediatrics. • Delay in fasciotomy could be due to delay in diagnosing compartment syndrome.
Introduction
Compartment syndrome (CS) is a clinical condition characterized by elevated pressure within a muscle compartment, leading to serious consequences, including neurological damage and ischemia. 1 This condition, first detailed by Richard von Volkman in the 19th century, 2 has long been acknowledged as a surgical emergency due to its potential to cause ischemia, muscle necrosis, permanent neurological damage, and limb loss.3,4
In adult trauma patients, CS has been linked to specific injury types such as long bone fractures, crush injuries, soft tissue damage, and vascular injuries.5,6 Although combined arterial and venous injuries (AVs) were once considered a strong indication for prophylactic fasciotomy, recent evidence supports close observation instead. 7 While injury patterns in adults have been thoroughly studied, the correlation between various traumatic injuries and CS in pediatric patients remains underexplored. Diagnosing CS in children is particularly challenging due to communication barriers and limited cooperation, complicating the largely clinical diagnosis, which typically includes symptoms such as pain, pallor, paresthesia, pulselessness, and paralysis or muscle weakness. 8
Lower extremity fasciotomy to decompress all affected compartments remains the standard of care for the treatment of CS in order to prevent long-term damage and/or limb loss. 9 Unlike adult patients, pediatric patients demonstrate a remarkable capacity for recovery with good functional outcomes after developing CS. 10 However, the risk of morbidity after delayed lower extremity fasciotomy in children remains a pressing concern. Additionally, the physiological responses to injury and subsequent healing differ significantly from adults, and thus, a more tailored approach may be required in children.
This study aimed to evaluate the time elapsed from presentation in the emergency department (ED) to the performance of lower extremity fasciotomy and examine specific injury patterns to identify potential risk factors. We hypothesized that the majority of pediatric patients with isolated lower extremity trauma undergo a lower extremity fasciotomy in a delayed fashion (exceeding 6 hours post-admission) and aimed to uncover the underlying risk factors for all pediatric fasciotomies.
Methods
A waiver of consent was obtained from our local institutional review board, as this study involved a deidentified national database. The Trauma Quality Improvement Program (TQIP) database, which combines data from over 900 trauma centers, was used to identify a retrospective cohort (2017-2020) of deidentified patients Pediatric fasciotomy patient selection.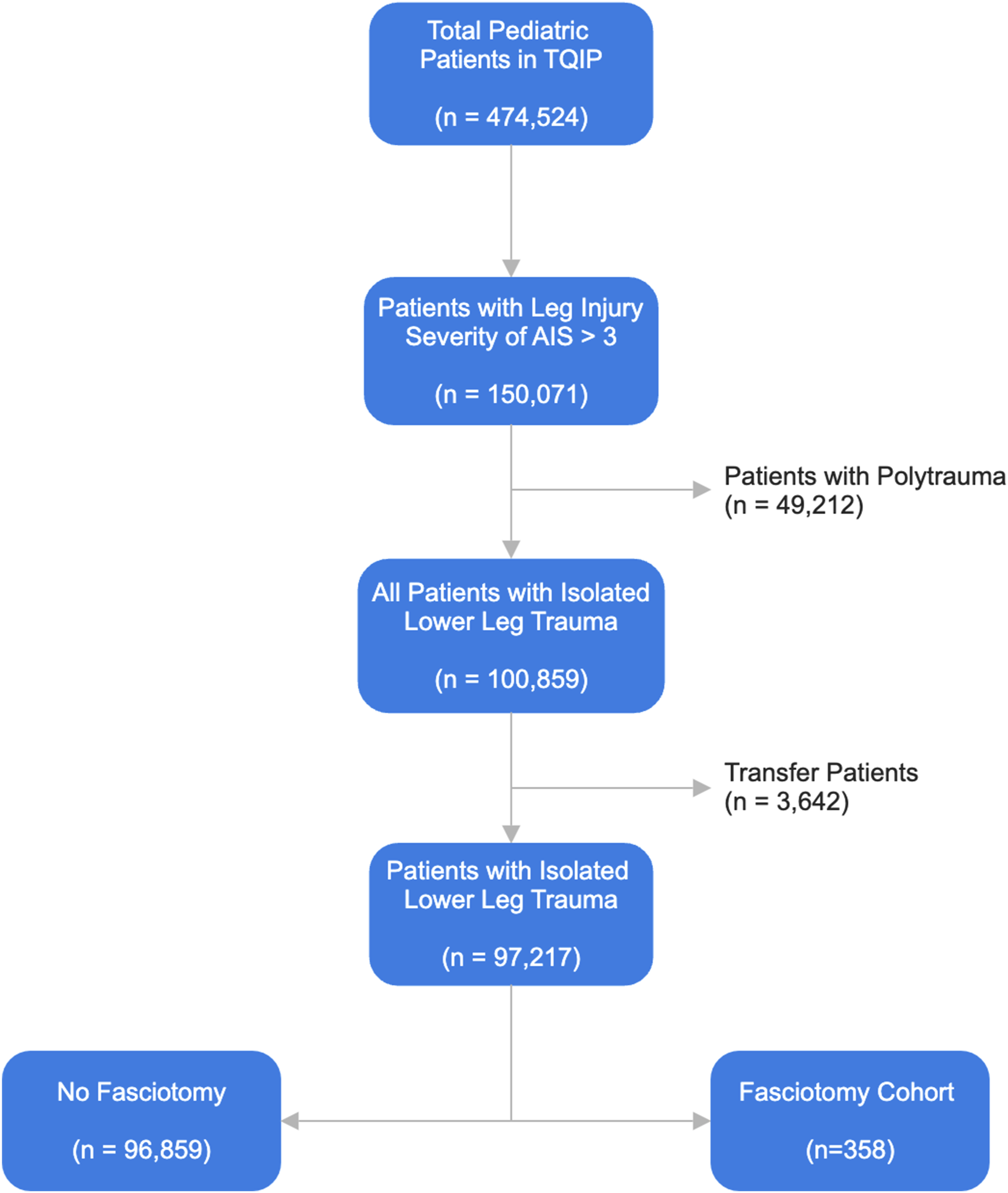
Patients were then classified into 2 groups: those who underwent fasciotomy at any point during hospitalization and those who did not. Age, sex, and comorbidities were analyzed. Comorbidities included attention-deficit hyperactivity disorder, congenital disorders, psychiatric disorders, smoking history, substance use disorder, and diabetes. The injury profile included mechanism of injury, crush injury, fractures of the lower extremity bones, nerve injury, and vascular injury to the leg. Vitals on arrival were recorded and included: hypotension (systolic blood pressure <90, tachycardia (heart rate >120), and tachypnea (respiratory rate >22).
Other outcomes measured included in-hospital complications such as cardiac arrest, superficial surgical site infection (SSI), deep SSI, pulmonary embolism (PE), pressure ulcer, acute respiratory distress syndrome, unplanned return to operating room (UROR), and unplanned intensive care unit (ICU) admission. We also analyzed the rate of limb loss, including both below-knee amputation and above-knee amputation identified as occurring within the same hospitalization. We also collected information on total hospital length of stay (LOS), ICU LOS, and ventilator days.
A Mann-Whitney U test was used to compare continuous variables for bivariate analyses and a chi-square to compare categorical variables for bivariate analysis. Categorical data was reported as percentages and continuous data was reported as medians with interquartile range. A multivariable logistic regression analysis was also performed to determine the associated risk of lower extremity fasciotomy in all patients. The variables entered into the model included age, sex, comorbidities, mechanism, severity of the injury (AIS
Results
Characteristics of Pediatric Fasciotomy Patients
From the 97217 pediatric patients with isolated leg injury, 358 (0.4%) underwent a fasciotomy at any point during hospitalization. The majority (60.3%) occurred in a delayed fashion, with a median time of 9.6 hours to fasciotomy from time of arrival (Figure 2). Patients undergoing fasciotomy were older (median age 14 vs 12 years, P < 0.001), with a higher proportion of males (83.8% vs 69.4%, P < 0.001). There was no difference in the rate of death in the ED between both groups (non-fasciotomy 0.2% vs fasciotomy 0%, P = 0.444). The rate of packed red blood cell transfusion was significantly higher in the fasciotomy group compared to those who did not undergo fasciotomy (7.8% vs 0.4%, P < 0.001) (Table 1). Percentage of fasciotomies performed by hour. Demographics and Comorbidities of Pediatric Patients Who Underwent Fasciotomies vs Patients Who Did Not. ADHD = attention deficit hyperactive disorder. COPD = chronic obstructive pulmonary disease; IQR = interquartile range. HR = heart rate; RR = respiratory rate; SBP = systolic blood pressure.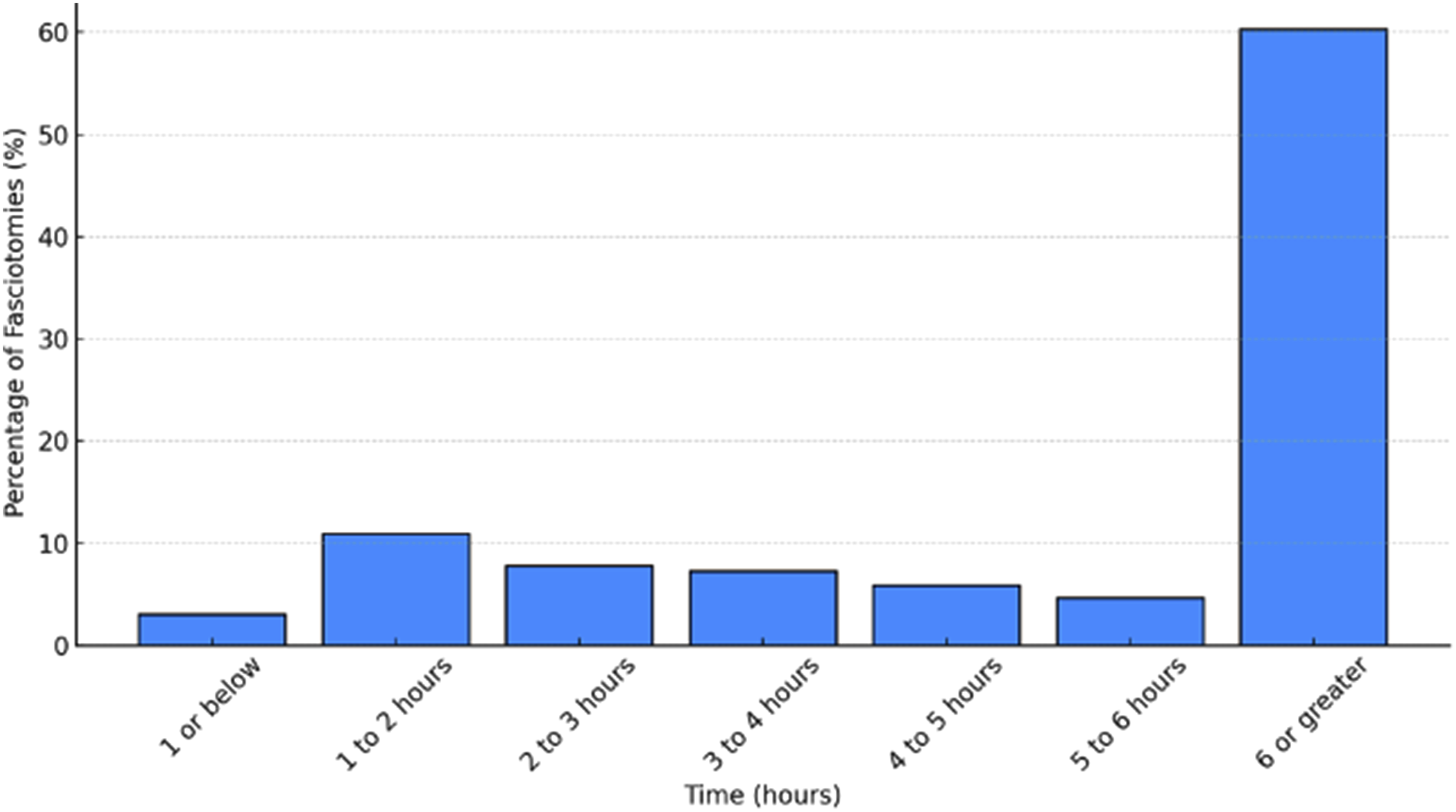
Injury Profile of Pediatric Fasciotomy Patients
Injury Profile of Pediatric Patients Who Underwent Fasciotomies vs Patients Who Did Not.
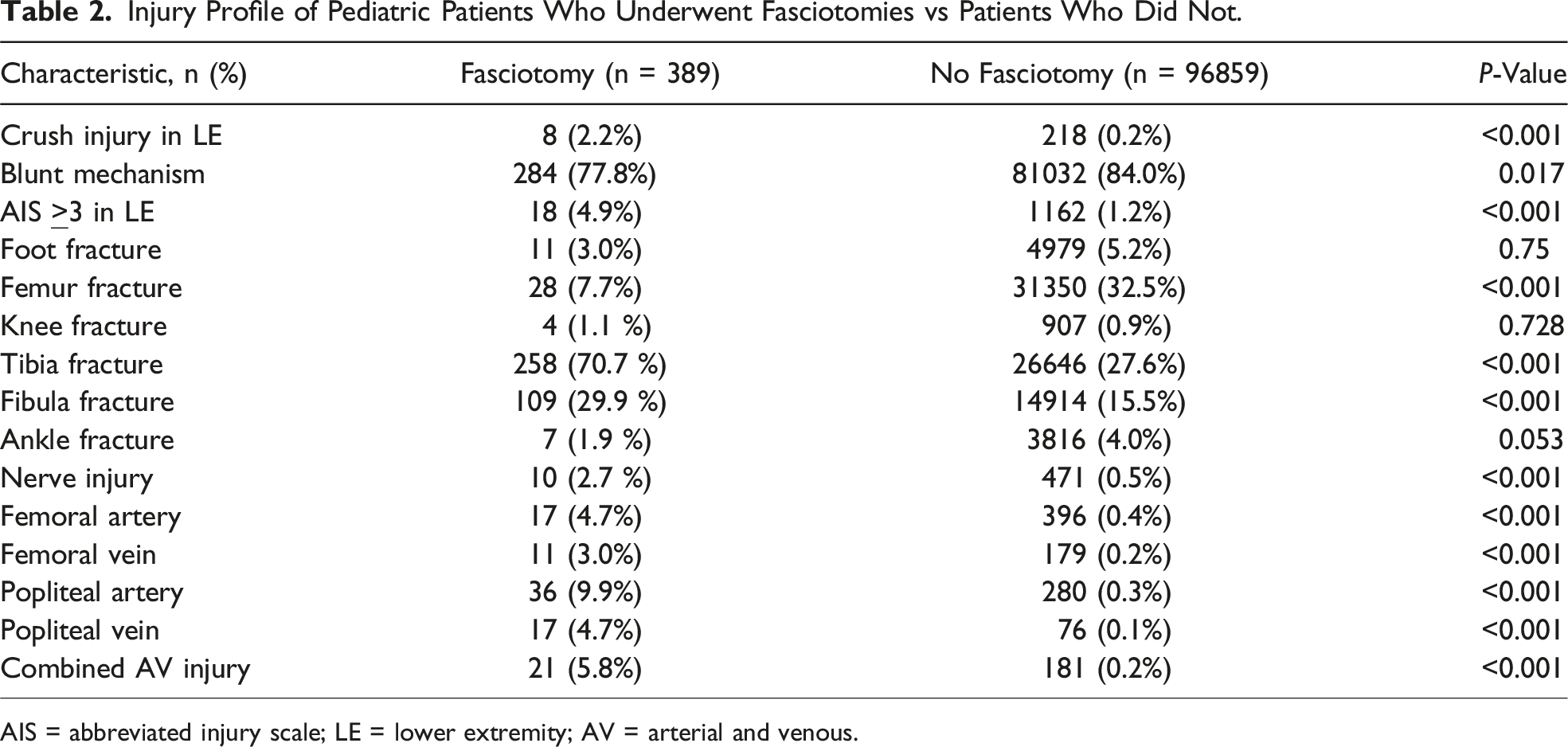
AIS = abbreviated injury scale; LE = lower extremity; AV = arterial and venous.
Complications in Pediatric Fasciotomy Patients
Complications in Pediatric Patients Who Underwent Fasciotomies vs Patients Who Did Not.
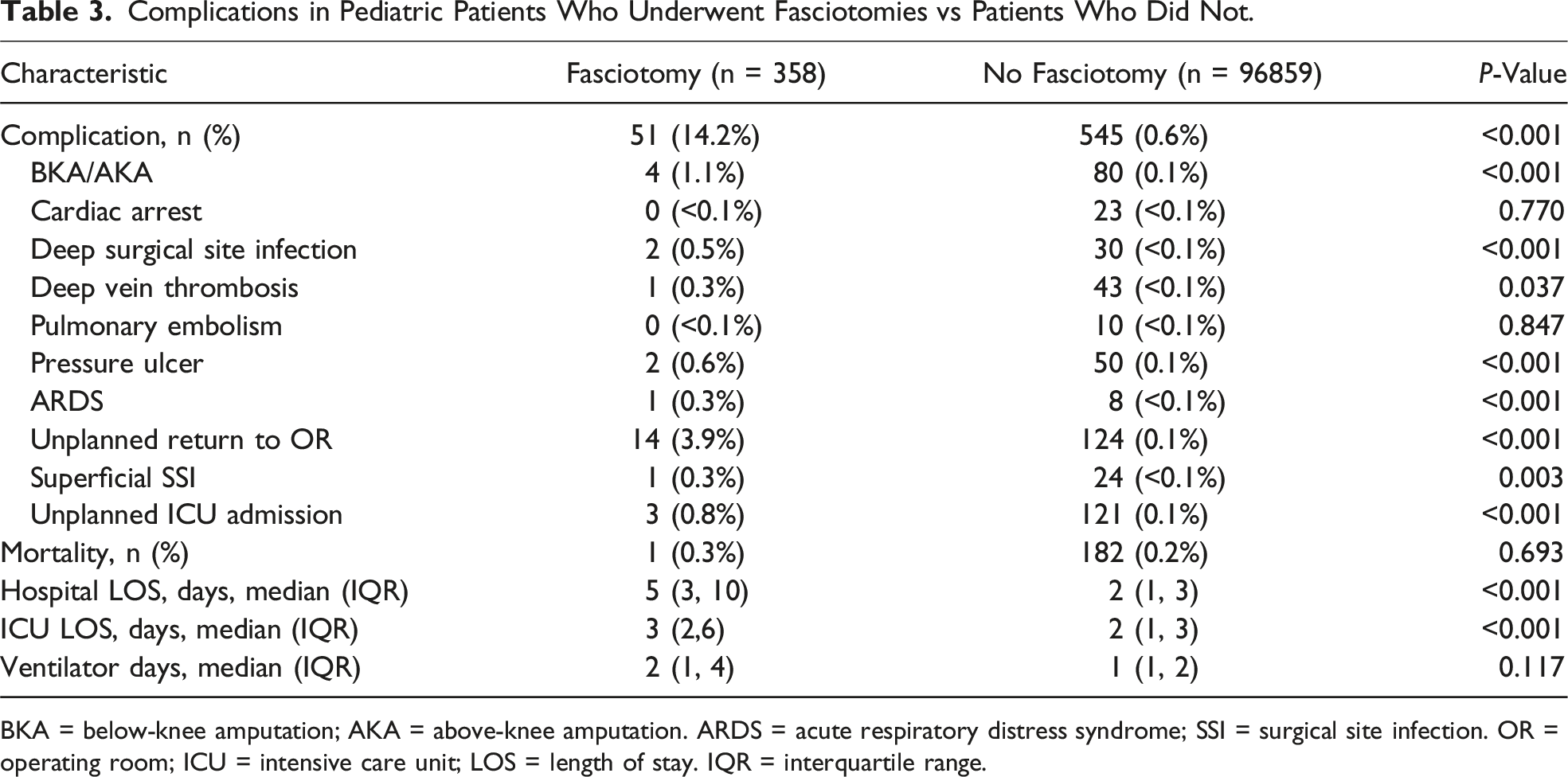
BKA = below-knee amputation; AKA = above-knee amputation. ARDS = acute respiratory distress syndrome; SSI = surgical site infection. OR = operating room; ICU = intensive care unit; LOS = length of stay. IQR = interquartile range.
Risk Factors for Fasciotomy Using a Multivariable Regression Analysis
Multivariable Logistic Regression Analysis Evaluating Associated Risk of Fasciotomy in Pediatric Patients With Isolated Lower Extremity Trauma.
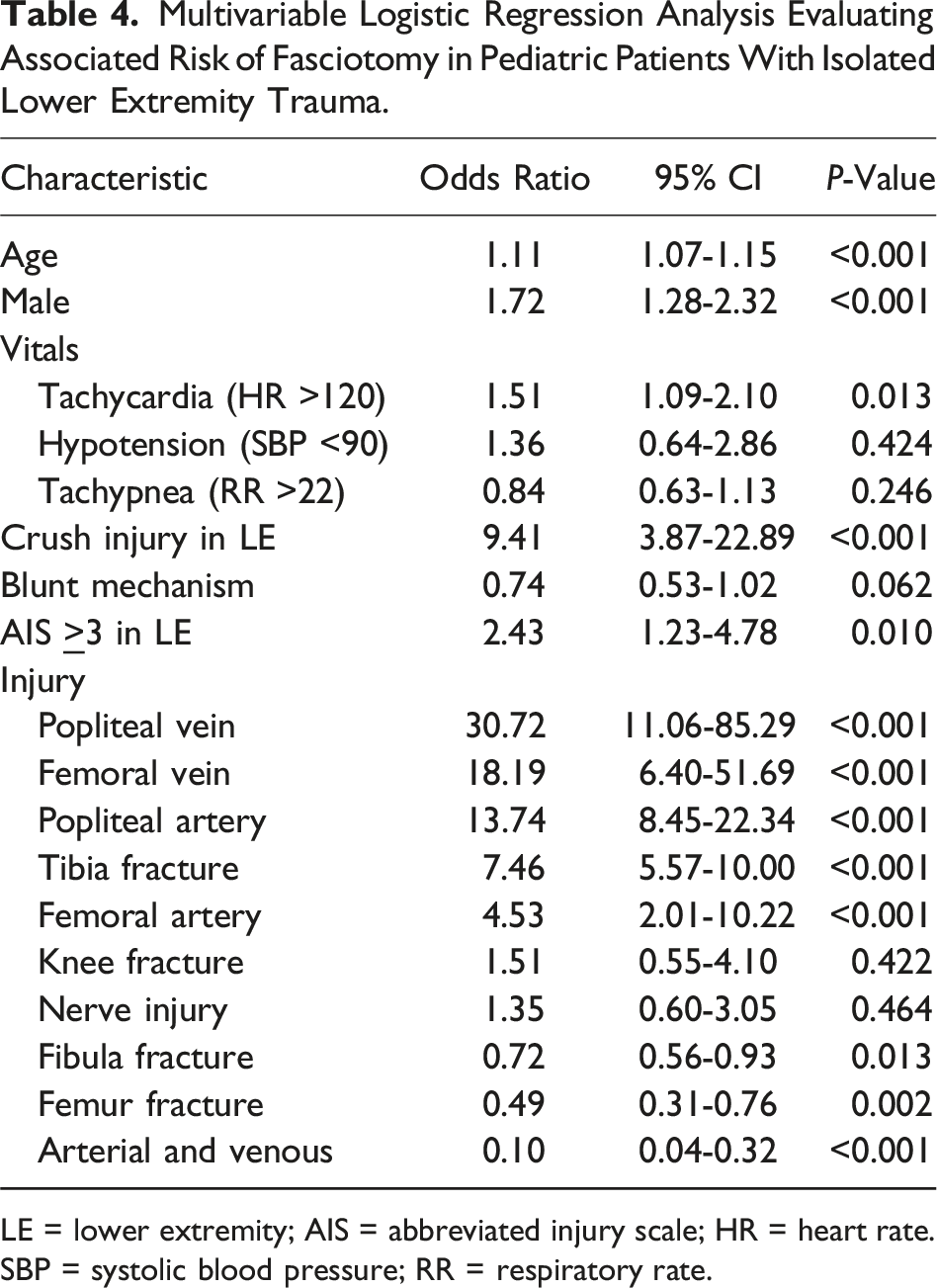
LE = lower extremity; AIS = abbreviated injury scale; HR = heart rate. SBP = systolic blood pressure; RR = respiratory rate.
Comparison of Delayed Fasciotomy to Nondelayed Fasciotomy Patients
Tibial fracture was more often seen in patients with delayed fasciotomy compared to patients who did not have a delay (81.0% vs 58.5%, P < 0.001). However, vascular injuries including injuries to the popliteal artery (18.3% vs 4.6%, P < 0.001) and popliteal vein (11.3% vs 0.5%, P < 0.001) and combined AV injury (13.4% vs 0.9%, P < 0.001) were seen more frequently in the cohort without delay. Overall complication rates were higher in the delayed fasciotomy group compared to the cohort who did not experience a delay (18.1% vs 8.5%, P = 0.011). The most common complications were compartment syndrome (14.0% vs 6.3%, P = 0.024) and unplanned return to the OR (6.6% vs 0%, P = 0.002) (Supplemental Tables 1,2,3,4).
Discussion
Compartment syndrome secondary to trauma in pediatrics is a rare but serious condition occurring in 0.4% of the patients identified in this national study of isolated lower extremity injuries. Interestingly, popliteal vein injury was the strongest associated risk factor. The rarity of this condition, combined with the difficulty in diagnosing CS in children, supports our finding that most fasciotomies in pediatric trauma patients with isolated lower extremity injuries are performed in a delayed manner, suggesting the need for continued vigilance during hospitalization to help avoid limb loss. This delay may partially be attributed to challenges in prompt diagnosis and decision-making regarding the timing of fasciotomy in children. 15 The significantly higher rate of blood transfusion within the first 4 hours in the fasciotomy group highlights the potential role of early blood product usage as a marker for severe vascular or soft tissue injury necessitating fasciotomy. The lack of extensive pediatric-focused research on the correlation between specific injury profiles and the risk of developing CS highlights the importance of this study.
The literature evaluating the prevalence, trends, and timing of pediatric fasciotomies is limited. Lin et al conducted a systematic review and meta-analysis, identifying just over 200 pediatric patients undergoing fasciotomies across all extremities, with the majority involving the lower extremity. The mean time from injury to fasciotomy in that cohort was 25 hours. There was no significant difference in the time to fasciotomy between patients who eventually regained full functional recovery and those who did not. 16 This finding aligns with another case series with 21 pediatric patients experiencing a median delay of 20 hours to fasciotomy but returned to pre-injury activity levels, though nearly 40% reported minor complications. 10 These studies highlight the remarkable capacity of children to recover even when fasciotomies are significantly delayed. While these studies indicate that the delay does not have a long-term impact on the functionality of the patient’s limb, our study did show a higher rate of all complications in delayed fasciotomy compared to patients without a delay. This increase in overall complication rates could lead to prolonged hospitalizations and increased health care costs, as well as increased stress on the patient. There are multiple reasons why these studies differ from our findings, where our national average time to fasciotomy was under 10 hours. These previous studies assessed the time to fasciotomy for all extremities and in all cases. In polytrauma, diagnosing CS in specific extremities could add complexity, potentially increasing the average time to fasciotomy. Furthermore, patients with severe polytrauma may have undergone life-saving procedures prior to fasciotomy, increasing their time to fasciotomy. In this study, we elected to exclude polytrauma patients in order to draw direct comparisons between 2 groups with minimal confounders from other injuries. Our study also showed a lower complication rate of ∼15% but a higher rate of limb loss in the fasciotomy cohort compared to the prior studies. The differences in complications may be due to several factors. First, our larger national cohort likely provides a more comprehensive view, reducing the impact of singular patient outcomes on overall results. Smaller sample sizes in previous studies mean that individual variances in timing to fasciotomy could disproportionately affect their findings. Second, variations in medical practices and resource availability across different regions and institutions could influence both the timing of intervention and the complication rates, which may be associated with disparities and social determinants of health. 17 Lastly, differences in follow-up duration and methods for tracking complications could result in underreporting or inconsistent reporting of adverse outcomes in smaller studies.
The delay in performing fasciotomies in children might be attributed to the difficulty in identifying the early signs of CS, which is further complicated by communication challenges with younger patients. The traditional 5 P’s mnemonic (pain, paresthesia, pallor, pulselessness, and paralysis) used for adults may not be as effective in a pediatric setting. Additionally, using adjuncts like compartment pressure measurements has potential pitfalls. 18 These pitfalls include the invasive nature of the procedure, the potential for false negatives, and the variability in pressure thresholds for different patients. Bae et al proposed an alternative approach tailored for children, the 3 A’s (agitation, anxiety, and increasing analgesia requirements), to facilitate earlier detection of CS. 8 This method aims to capture more subtle and behaviorally evident signs that may be more reliable indicators in a pediatric population.
Historically, femur fractures were the injury most associated with CS in children. However, recent studies have indicated a shift toward a stronger association with below-knee leg fractures. 8 This change is partly attributed to evolving clinical practices, such as early operative intervention for femur fractures. Flynn et al reinforced this shift in focus by reporting a greater association between tibial fractures and CS. 19 Our study is novel as it examines extra-skeletal associations with CS in children. We identified vascular injuries, particularly popliteal vein injuries, as the strongest associated risk factors for fasciotomy after isolated pediatric leg trauma. The increased risk of fasciotomy related to vascular injury seen in our study, compared to previous studies, may be due to the difficulty in diagnosing vascular injuries in children. In pediatric populations, plain film radiographs are commonly obtained and can easily diagnose orthopedic injuries. However, computed tomography scans, which are more effective in detecting vascular injuries, are used more judiciously in children compared to adults. This cautious use of CT scans may lead to delayed diagnosis of vascular injuries, resulting in expanding hematomas in the lower leg and subsequent CS. Furthermore, advancements in orthopedic fracture management, such as the use of spica casts and intramedullary fixation, may also reduce the risk of CS related to long bone fractures. These modern techniques likely contribute to the observed shift from femur fractures to lower leg fractures and vascular trauma as the primary injuries associated with CS in children.
Combined AV injuries have been implicated in increased risk of fasciotomy in previous studies. Interestingly, our study did not find a correlation between combined AV injuries and an increased risk of fasciotomy after isolated lower extremity trauma in pediatric patients. While there was a higher incidence of AV injuries in the fasciotomy group, our multivariable regression analysis did not show evidence of increased risk for fasciotomy independently with combined AV injury, unlike the single-vessel injuries that were identified as risk factors. This finding contrasts with adult trauma literature. Branco et al evaluated nearly 300 adult patients who underwent fasciotomy and found that about 40% had combined AV injuries, which were associated with an increased risk for fasciotomy. 20 Some authors have advocated that a combined AV injury is a relative indication for prophylactic fasciotomy, 2 while others have argued for a more conservative watchful waiting approach. 7 There are several potential reasons why our study did not show a higher risk of fasciotomy in combined AV injury patients. One possibility is the broad definition of AV injury used in various studies. Different combinations of vascular injuries could have varying clinical significance, especially if the injured vessels are smaller in caliber or located in different compartments. Additionally, pediatric patients may have different physiological responses and healing capabilities compared to adults, potentially influencing the outcomes of combined AV injuries. Another reason could be the advancements in diagnostic imaging and surgical techniques, which may have improved the management of AV injuries and reduced the necessity for fasciotomy. Lastly, differences in study design, patient populations, and inclusion criteria could also account for the discrepancies between our findings and those of previous studies.
Limitations to this study include reporting and selection bias, which can occur in any large database study. A potential confounder includes that timing to fasciotomy was based on presentation to the ED and not time from injury, which may be varied in each case and may have led to a shortened time to fasciotomy when compared to prior studies. The shorter time to fasciotomy observed in our cohort compared to prior studies may be explained by our inclusion criteria, which focused exclusively on patients with isolated lower extremity injuries. Unlike polytrauma cohorts, where life-threatening injuries often delay the timing of fasciotomy, our approach minimized this confounder and allowed for more direct comparisons. However, this limits the generalizability of our findings to more complex trauma populations, and future studies should investigate the impact of polytrauma on fasciotomy timing and outcomes. In addition, CS may have arisen in a delayed fashion; thus, the terminology delayed fasciotomy should not be taken as delayed treatment for all patients included in this cohort. However, in a large database study, it would not be possible to have access to this specific granular information. In addition, TQIP does not have symptomology, which would be highly relevant to determine the rate of CS preceding fasciotomy. Also, TQIP does not include patient-centric outcomes such as chronic pain, neuropathy, or muscle weakness, which can be seen as potential long-term complications from delayed fasciotomy. Furthermore, TQIP does not include details for return to the OR, which leads to uncertainty about whether it was related to the lower extremity trauma or due to a different injury. Another limitation is that TQIP lacks pre-hospital information that could be clinically relevant including tourniquet usage, blood loss at the scene, and time to arrival at the hospital. The Trauma Quality Improvement Program also does not include post-discharge complications, so we would not have data regarding patients who developed complications following their index admission. Finally, given the nature of a large database study, we are unable to establish causality for specific injuries resulting in increased risk for fasciotomy as evidenced by why an isolated popliteal vein injury is associated with an increased risk of fasciotomy, whereas an AV injury is not.
Compartment syndrome remains a rare but serious condition in children with lower extremity injuries. Most fasciotomies in these patients are performed in a delayed fashion, often exceeding 6 hours. This is associated with substantial risks, including a higher rate of limb loss. This national analysis identified vascular injuries as associated risk factors for fasciotomy. While advancements in orthopedic management and diagnostic imaging have influenced injury profiles and outcomes, diagnostic algorithms for potential vascular injuries have not been as thoroughly constructed. Future prospective multicenter studies will be needed to create criteria for CT implementation to aid in the identification of vascular injuries. Further research is also needed to develop tailored protocols for early detection and treatment of CS in pediatric trauma patients.
Supplemental Material
Supplemental Material - Risk Factors and Timing of Fasciotomy for Isolated Pediatric Lower Extremity Trauma
Supplemental Material for Risk Factors and Timing of Fasciotomy for Isolated Pediatric Lower Extremity Trauma by Mennatalla Hegazi, Jeffry Nahmias, Michael Lekawa, Matthew Dolich, Allen Kong, Cristobal Barrios, and Areg Grigorian in The American Surgeon™
Footnotes
Author Contributions
Jeffry Nahmias MD MHPE: supervision and writing—review/editing (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data sets generated during the current study are available in the Trauma Quality Improvement Program Database.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.