
Abstract
Background
Breast conserving surgery represents the preferred surgical treatment option for patients with early-stage breast cancer. Reexcision rates are generally higher for patients undergoing lumpectomies for ductal carcinoma in situ (DCIS) compared to invasive breast cancer, as the microscopic extent of disease is difficult to assess during excision. This study investigated the clinicopathological characteristics of patients undergoing BCS for pure DCIS and reexcision rates over time, including the effect of the MarginProbe™ device.
Methods
We queried our prospectively maintained Institutional Breast Cancer Database for patients diagnosed with DCIS and treated with BCS as their primary procedure from 2010-2021. The primary endpoint was the rate of reexcision. Variables of interest included age at diagnosis, race/ethnicity, mode of diagnostic imaging, mammographic breast density, method of core biopsy, nuclear grade, size of DCIS, multifocality, DCIS subtype, and MarginProbe™ use.
Results
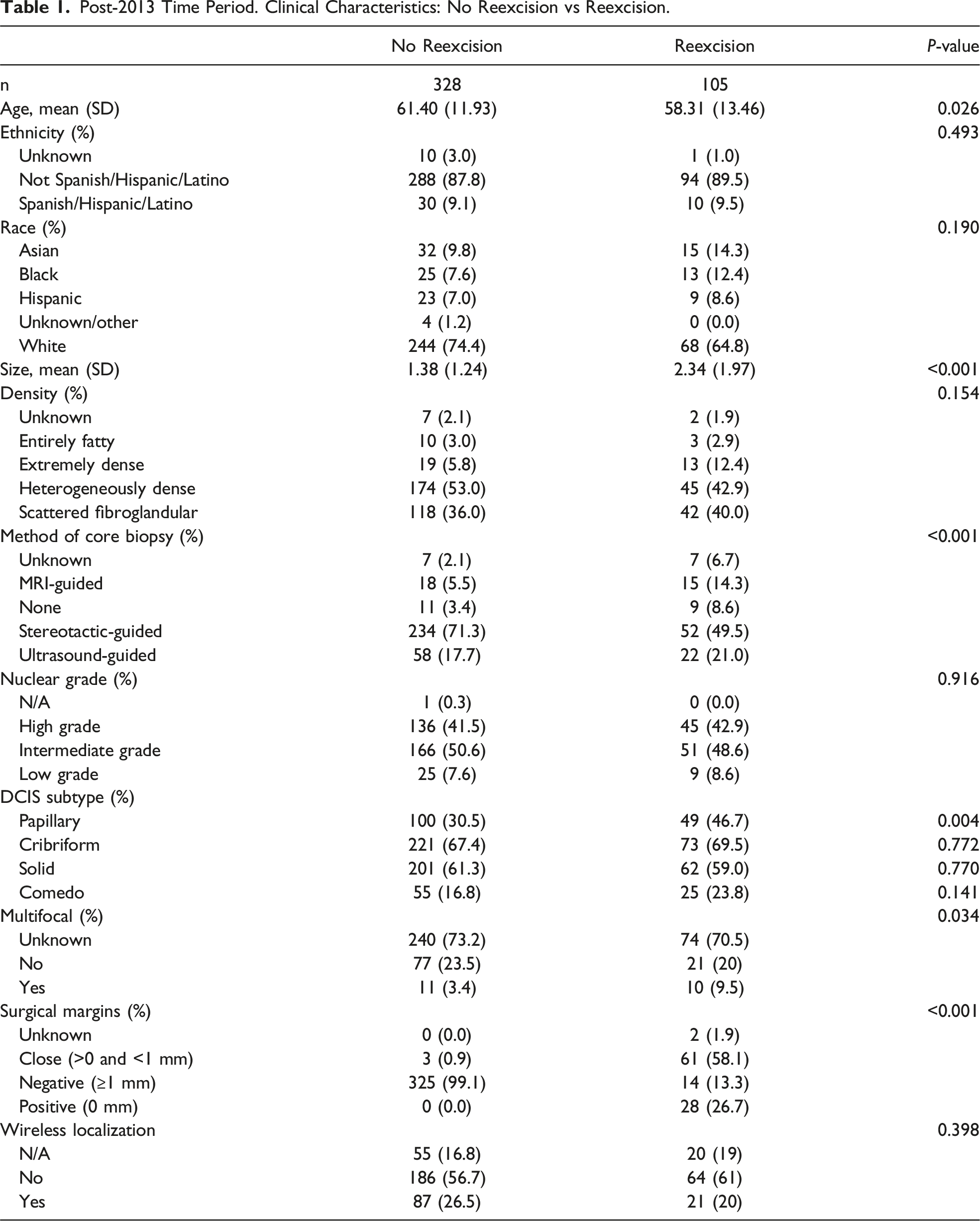
Papillary DCIS (P < 0.004) and larger size (P < 0.001) was associated with an increased reexcision rate. There were also differences in the method of core biopsy (P < 0.001), with stereotactic core biopsy predominating among patients who did not require reexcision (71.3% vs 49.5%). In an unadjusted estimate for the odds ratio for association, patients who had MarginProbe™ used were 81% less likely to require reexcision (OR = 0.19, 95% CI = 0.12, 0.31, P < 0.0001).
Conclusion
Younger age, papillary DCIS, larger DCIS size, and non-stereotactic core biopsy method were found to be associated with higher reexcision rates. Additionally, patients whose primary procedures included intraoperative margin assessment with the MarginProbe™ were significantly less likely to require reexcision.
Introduction
Breast conserving surgery (BCS) represents the preferred surgical treatment option for a majority of patients with early-stage breast cancer who are eligible for this approach. It is clear that, even in the presence of optimal post-lumpectomy radiation treatment, it is necessary to achieve clear surgical margins as positive lumpectomy margins are associated with an increased risk for ipsilateral breast tumor recurrence. 1 Involved lumpectomy margins necessitate additional surgical procedures, and patients may choose to transition to a mastectomy approach if a primary lumpectomy is unsuccessful. Furthermore, reexcision surgeries result in increased operating room (OR) time and costs thus placing a financial burden on the health care system at large. 2
While reexcision rates vary by institution and surgeon, on average, 20% of patients undergoing BCS require a reexcision procedure. 3 Reexcision rates are generally higher for patients undergoing lumpectomies for ductal carcinoma in situ (DCIS) when compared with patients with invasive breast cancer, as those lesions are often non-palpable and the microscopic extent of disease is difficult to assess at the time of excision. As a result, this is a challenging subset of patients to successfully treat with one stage lumpectomies. 3
Recent innovations have focused on techniques to provide surgeons with real-time intraoperative assessment of lumpectomy margins. One such device, the MarginProbe™ (Dilon Technologies, USA), uses radiofrequency spectroscopy to distinguish between normal and malignant tissue. 4 Immediately following surgical excision of the malignancy, the 7 mm sensor on the end of the MarginProbe™ is brought into contact with the specimen where it interrogates the six margins (superior, inferior, medial, lateral, anterior, and posterior). The device emits an audible and visual signal when it detects an involved margin thus prompting the surgeon to obtain a shave margin at the respective positive margin. This device is one of several new technologies being studied for intraoperative margin assessment.
This study aimed to investigate the clinicopathological characteristics of patients undergoing BCS for pure DCIS and the rates of reexcision over time, including the effect of the MarginProbe™ device.
Materials and Methods
Inclusion/Exclusion Criteria and Endpoints
We queried our prospectively maintained Institutional Breast Cancer Database for patients diagnosed with pure DCIS and treated with BCS as their primary procedure from 2010-2021. Histological confirmation of DCIS as the primary diagnosis was required for inclusion; cases of microinvasion were excluded. All included patients were treated with breast conservation surgery as their index procedure. Primary surgeries performed at outside facilities were excluded. Pathologic upgrades to DCIS following excisional biopsy (ie, pathology upgraded from ADH to DCIS on final pathology) were also excluded.
The primary endpoint was the rate of reexcision. Variables of interest included age at diagnosis, race/ethnicity, mode of diagnostic imaging, mammographic breast density, method of core biopsy, nuclear grade, size of DCIS, multifocality, and DCIS subtype.
Surgical Technique
Surgeons were comprised of a mix of general surgeons and breast surgical oncologists. The surgeons and the operative approach were the same in both the pre- and post-2013 time periods. Non-palpable lesions were localized with either a SAVISCOUT® or wire, at the discretion of the surgeon.
Intraoperative Margin Assessment
Prior to 2013, intraoperative margin assessment at our institution included the surgeon’s gross examination of the surgical specimen as well as interpretation of 2D specimen radiography. In 2013, the MarginProbe™ was introduced and quickly adapted by our surgeons. The MarginProbe™ was used in addition to the previously used margin assessment measures. The MarginProbe™® was not applied to the resected new margins.
Comparisons and Statistical Analysis
Patients were stratified into 2 time periods, “pre-2013” and “post-2013,” based upon the year in which the MarginProbe™® was introduced at our institution. Clear margins were defined as ≥1 mm, as a significant number of patients in both time cohorts underwent surgery prior to the release of the ASCO/SSO/ASTRO consensus guidelines recommending margins of at least 2 mm for pure DCIS, thus maintaining consistency between the 2 cohorts. Adjusted odds ratios for the association of MarginProbe™® with reexcisions were calculated using a multivariable logistic regression model controlling for age, tumor size, breast density, and DCIS subtype. Individual comparisons of continuous variables were based on t-tests, group proportions compared with one-way ANOVA, and categorical variables compared using Chi Square tests. Descriptive analyses were conducted in the R statistical software program and consisted of frequencies, proportions, and plots for trends. 5 A propensity score matched odds ratio for the association of MarginProbe™® with reexcisions—matching on age, tumor size, BRCA1/BRCA2, core biopsy method, surgical margins, and primary surgeon—was calculated using the R package MatchIt. 6
Results
Rates of reexcision over time
During our study period, there were 715 patients who underwent breast conserving surgery for DCIS. There were 226 reexcision procedures in the study period. There was a statistically significant 2% decline per year (P = 0.002) in the number reexcisions as a proportion of patients treated during the study period (Figure 1). In the pre-2013 time period, the number of reexcisions as a proportion of patients was approximately 41.9%. This decreased to 24.9% in the post-2013 time period, thus demonstrating an approximately 42.1% (SD = 27.2) decrease from the pre-2013 time period (P = 0.02). Reexcisions over time as a proportion of surgeries.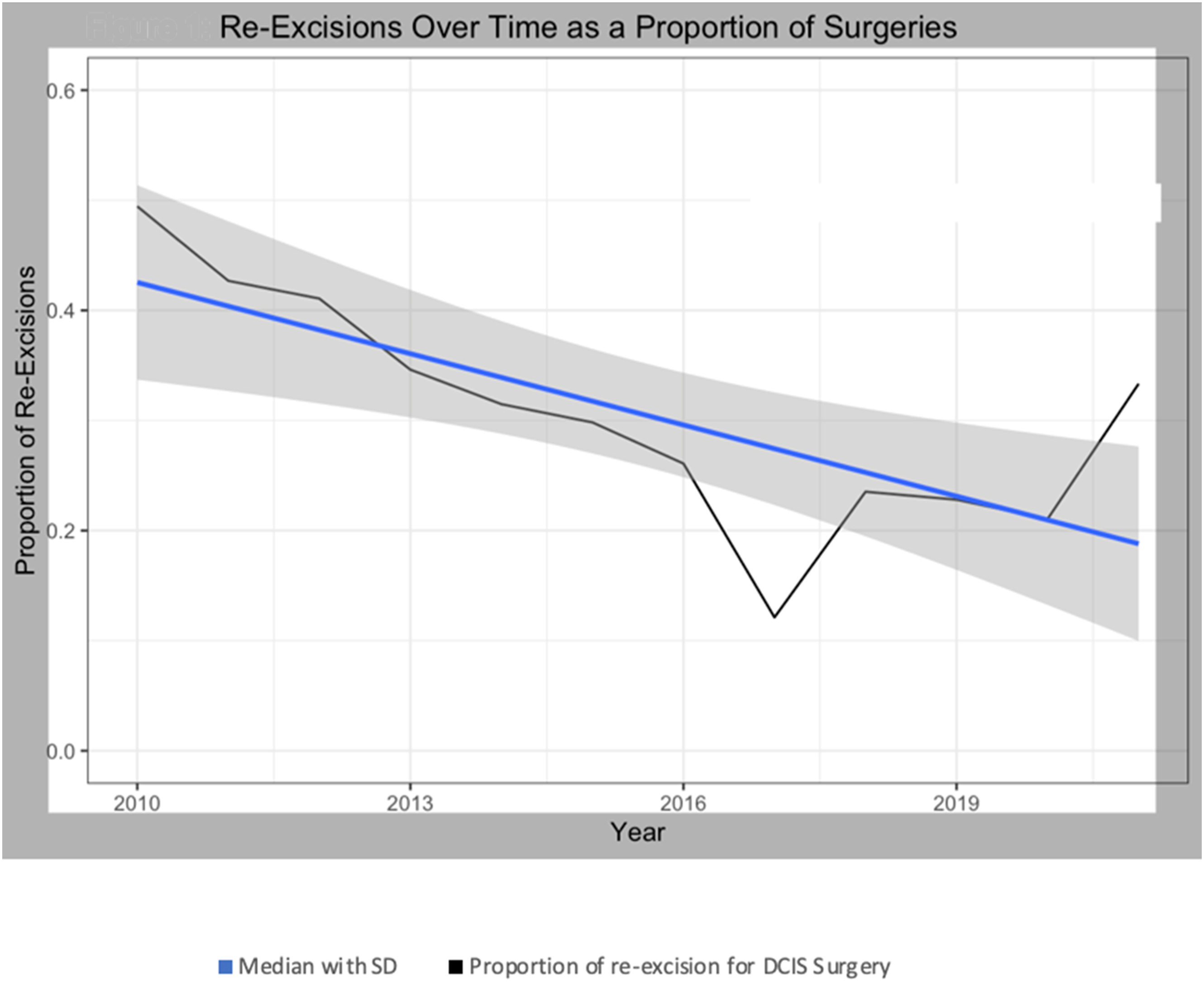
Patient and Clinicopathologic Data
Post-2013 Time Period. Clinical Characteristics: No Reexcision vs Reexcision.
Association of MarginProbe with Reexcisions
In an unadjusted estimate for the odds ratio for association, patients who had MarginProbe™ used were 81% less likely to require reexcision (OR = 0.19, 95% CI = 0.12, 0.31, P < 0.0001). In a logistic regression model with reexcision as the dependent variable and MarginProbe™ as the primary explanatory variable; controlling for age, tumor size, age at menopause, breast density, and core biopsy mode, patients for whom MarginProbe™ was used, were 65% less likely to require reexcision (OR = 0.35, 95% CI 0.17, 0.69). In a propensity score matched model matched on age, tumor size, breast density, core biopsy mode, and primary surgeon, patients for whom MarginProbe was used were 79% less likely to require reexcision (OR = 0.21, 95% CI 0.12, 0.35, P < 0.0001).
Patients Who Underwent Additional Surgery
Of patients who required reexcision, 20% (45/226) went on to mastectomies as their second procedure (Figure 2). Thirteen percent (6/45) of the patients who proceeded to mastectomy as their second procedure were BRCA1 or 2 mutation carriers. After each unsuccessful reexcision, a larger proportion of patients converted to mastectomy. In total, 26% of patients who had unsuccessful primary surgery went on to mastectomies (Figure 2). Procedure type at subsequent surgeries.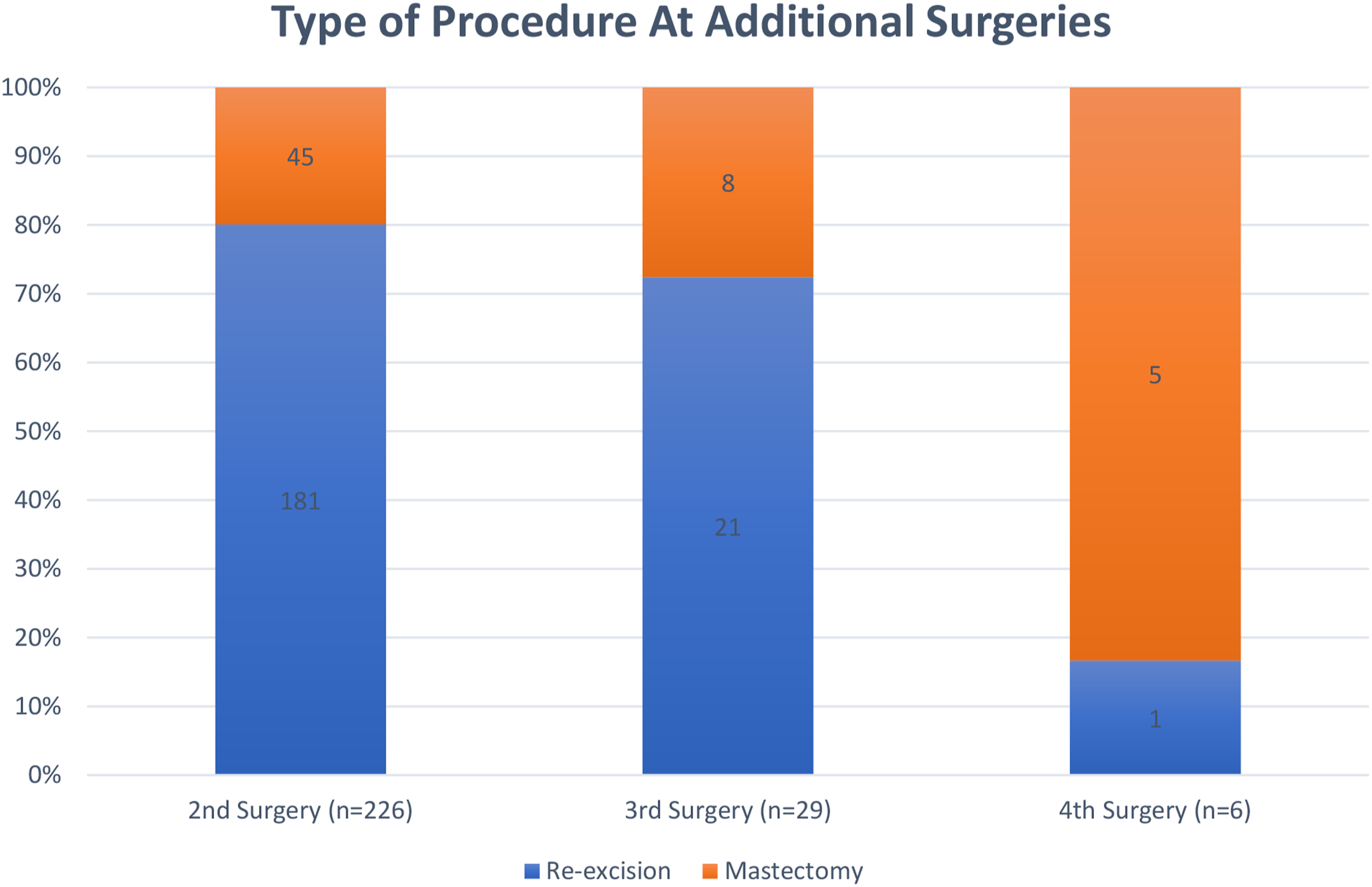
Discussion
In 2022 approximately 51,400 patients were diagnosed with DCIS, among whom 60% were treated with BCS. 6 BCS offers several advantages compared to mastectomy, however there was an associated risk of additional reexcision surgeries, which negatively impact patient experience and are a financial burden to the health care system. 2 The surgical management of DCIS can be challenging as it is often non-palpable and difficult to discern the microscopic extent of disease at the time of surgery. This study evaluated over 700 patients with pure DCIS treated with primary BCS at a single center institution and found that papillary subtype of DCIS, larger size of DCIS, and method of core biopsy were independently associated with increased rates of reexcision. Furthermore, the use of the MarginProbe™ device at the time of index surgery was associated with a significantly reduced rate of reexcision procedures.
Although required for optimal oncologic outcomes, undergoing additional surgeries required to achieve adequate margins can be associated with poorer cosmesis, patient anxiety, delay of adjuvant treatment, and increased health care costs. 7 OR times were calculated on average to be 41 minutes for margin reexcision and 132 minutes for completion mastectomy translating to total costs consisting of $301,866 and $1,460,347, respectively, including the cost of implants. 2 The MarginProbe™ has a quoted cost of $700 to $1700 per case, which pales in comparison to the cost of $1374 for reexcision and $8447 for mastectomy with reconstruction.2,8 There is some concern that surgeons may avoid offering BCS in more complex cases due to a higher likelihood of not achieving appropriate margins during the initial procedure. In a study by Silva et al, rates of mastectomies were thought to increase out of concern for reexcision costs, even in cases where BCS would be possible. However, with the majority of costs coming from mastectomy with reconstruction, incentivizing for BCS with low reexcision rates would have the greatest economic impact.9,10
One strategy to obtaining negative margins during the initial breast conserving surgery is by performing cavity shave margins which can reduce the rate of positive margins by 50%. A multicenter randomized controlled study by Chagpar et al showed that patients with stage 0-3 breast cancer who underwent breast conservation surgery with shave margins were significantly less likely to have positive margins than patients who were not treated with additional shave margins. 11 However, other retrospective studies suggest low rates of positive margins of 11%, even without additional shave margins resulting in no additional benefit of routine shave margins and creating larger lumpectomy cavities. 12 The cavities from larger lumpectomy specimens may lead to increased morbidity such as seromas and infections, as well as achieving less desirable cosmetic outcomes. 12
Various technologies have been proposed for intraoperative margin assessment to reduce the rate of reexcisions. The MarginProbe™ is used by surgeons to provide an intraoperative assessment of lumpectomy margins with a sensitivity of 70-100% and a specificity of 70-87%. 13 The MarginProbe™ was evaluated in a large multicenter, randomized, controlled study in patients with non-palpable disease and showed a 23% relative reduction in reexcision rate. 13 One limitation of the MarginProbe™ is its relatively high potential for false-positive (53.6%) or false negative (24.8%) results. Breast tissue density may influence adequate margin detection by the device, and warrants further investigation.14,15 Volumetric specimen imaging (VSI) is another method of intraoperative margin assessment, which produces a 3-dimensional and thin-slice cross sectional visualization of the lumpectomy specimen. A prospective study comparing VSI to both two-dimensional specimen radiograph and specimen tomosynthesis suggested that using VSI for margin assessment may reduce reexcision rates in patients with malignant disease. 16 A third suggested strategy is the use of a fluorescence-guided system (FGS) involving the injection of pegulicianine prior to surgery, and probing the cavity to look for signals of residual tumor to assist in obtaining adequate margins. Although they did not achieve their pre-determined endpoint, a prospective study by Smith et al showed the use of FGS achieving a sensitivity of 49.3% and specificity of 85.2%. 17
Understanding the factors associated with reexcision allows for identification of patients with DCIS who are at an elevated risk for reexcision. In our study of patients diagnosed with pure DCIS and treated with primary BCS, younger age, larger size of DCIS, and papillary subtype were associated with an increased rate of reexcision procedures, consistent with previously published data.18,19 Furthermore, as displayed in Figure 2, subsequent procedures increasingly resulted in patients undergoing a mastectomy. Discussing these data in the preoperative setting provides patients with realistic expectations and facilitates a strategy of shared decision making when deciding on the most appropriate surgical approach.
Our study also showed stereotactic guided method of core biopsy was associated with decreased reexcision rates. There are limited studies demonstrating an association between method of biopsy and reexcision risk in pure DCIS. In one study, ultrasound-guided core needle biopsy was associated with increased reexcision rates leading the authors to suggest that DCIS visualized on ultrasound may indicate more extensive disease. 20 Stereotactic biopsy is traditionally performed for lesions or calcifications not visualized on ultrasound. Taking both of these findings into consideration, it is possible that the DCIS diagnosed using stereotactic biopsy in our study was reflective of smaller disease burden successfully treated with a single stage operation. It is also possible that stereotactic guidance enables more accurate measurement of the extent of disease thus facilitating optimal excision.
Our institution’s reexcision rate of 24.9% is within the spectrum of rates previously reported in single-institution studies, which spans from 14 to 78%.21-28 The wide range of published reexcision rates may partially be due to the longstanding debate regarding the adequate margin width for women undergoing breast conservation treatment, especially when the diagnosis is DCIS. 29 Indeed, in our study cohort, there was a statistically significant 2% decline per year in the yearly number of reexcisions as a proportion of patients treated, likely secondary to international society guidelines supporting a narrower margin width for DCIS.
Recent data have shown low 5-year local recurrence rates with BCS in the setting of multifocal disease. 30 Further supporting these findings, the current study did not demonstrate an association between multifocality and need for reexcision. The increased utilization of BCS in patients with more extensive disease may present surgeons with an additional challenge to one stage lumpectomy surgery.
The current study is not without limitations including selection bias inherent to retrospective studies. This study did not report data on long-term outcomes; however, previous studies have demonstrated an association between positive margins and risk of local recurrence. Data on specimen size was not collected, and hormone-receptor status was not analyzed. Additionally, we used ≥1 mm to define clear margins to maintain consistency between the 2 cohorts. It is therefore possible that our observed decreased reexcision rate was influenced by the release of ASCO/SSO/ASTRO consensus guidelines recommendation of at least 2 mm for negative margins. However, there was a decrease in the reexcision rate with the introduction of the MarginProbe™ prior to the release of the guidelines in 2016.
A proportion of patients with unsuccessful primary lumpectomies required multiple procedures to complete their surgical treatment and 26% went on to mastectomy. Patients whose primary procedures included intraoperative margin assessment with the MarginProbe™ were significantly less likely to require reexcision. Intraoperative margin assessment is an important tool that can support BCS in the challenging population of patients with DCIS. Statistically significant factors such as size and papillary subtypes should be considered when discussing BCS.
Conclusion
Among our cohort of over 700 women treated with primary lumpectomy for pure DCIS, 26% of patients who had inadequate margins following primary surgery went on to mastectomies. Younger patient age, papillary subtype of DCIS, larger size of DCIS, and non-stereotactic core biopsy method were found to be associated with higher reexcision rates. Additionally, patients whose primary procedures included intraoperative margin assessment with the MarginProbe™ were significantly less likely to require reexcision. Knowledge of these high-risk features can facilitate shared decision-making and assist in achieving one stage lumpectomy in the challenging population of patients with pure DCIS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.