
Abstract
When equitable care is considered, patients with disabilities are often not included. This is unfortunate because patients with disabilities experience some of the most pronounced barriers to care of any marginalized group. Special attention should go this group in order to increase access and improve quality of care. Telehealth and other technological strategies can help to decrease some of these disparities. A focus on this population needs to be included throughout medical education so that physicians can have an increasing understanding of the challenges faced as well as potential solutions.
Introduction
Disability is defined by the Center for Disease Control (CDC) as any condition of the body or mind that makes it more difficult to perform activities and interact with the surrounding world. 1 In 2022 the World Health Organization (WHO) estimated that 1.3 billion people or 16% of the global population worldwide experience a significant disability. 2 This includes physical, cognitive, developmental, behavioral, and sensory impairments. The Global report on health equity for persons with disabilities reported that due to systemic and health inequities, people with disabilities experience poorer health outcomes including morbidity, mortality, and function. 2 People with disabilities often encounter challenges such as ableism, financial insecurity, disparate healthcare expenses, lack of autonomy, delays in treatment, and limited access to suitable healthcare facilities.2,3 Surgery is recognized as an essential component of primary health care; without it we see increased mortality which is worse for all marginalized groups including people with disabilities.4,5 Most of the current literature is focused on general healthcare disparities for people with disabilities but there is little information available about their access to surgical care. In this article, our goal is to not just explore these disparities but also propose potential solutions for more equitable care.
Root Causes
Access to surgical care is directly affected by many things including socioeconomics, geography, accessibility needs, and communication barriers. Socioeconomics can have a huge effect on access because it includes insurance coverage, financial barriers, and employment inaccessibility. Unfortunately, patients with disabilities can be disproportionally affected by these socioeconomic factors. Some root causes are the same for all people but worse for people with disabilities. Health care costs are a huge driver of access not just because of the costs of care. For patients that have insurance, co-pays or deductibles can be high and there can be unforeseen costs, or other factors.
6
Patients often avoid seeking care due to concerns about these costs which can worsen outcomes because of delays in care.
6
In addition, patients with disabilities can have worse surgical outcomes regardless of their insurance status. Because children with cerebral palsy (CP) tend to have more frequent healthcare visits, their families are often connected with case managers and help with insurance options like Medicaid.7,8 One study found that patients with (CP) undergoing appendectomy had worse postoperative outcomes despite having 97% insurance rates.
6
These outcomes can include longer hospital stays, increased level of care, and higher rates of reoperation and readmission, all of which increase associated costs.
7
In one survey of U.S. adults, presence of a disability was associated with lower household income, unemployment, and educational disadvantage including a high school education ceiling.
9
Patients with disabilities face a poverty cycle because financial insecurity contributes to both transportation insecurity and employment limitations
10
(Figure 1). Decreased access to surgical care and interventions is multifactorial for disabled adults but clearly stems from several socioeconomic factors. Poverty cycle that many disabled patients face.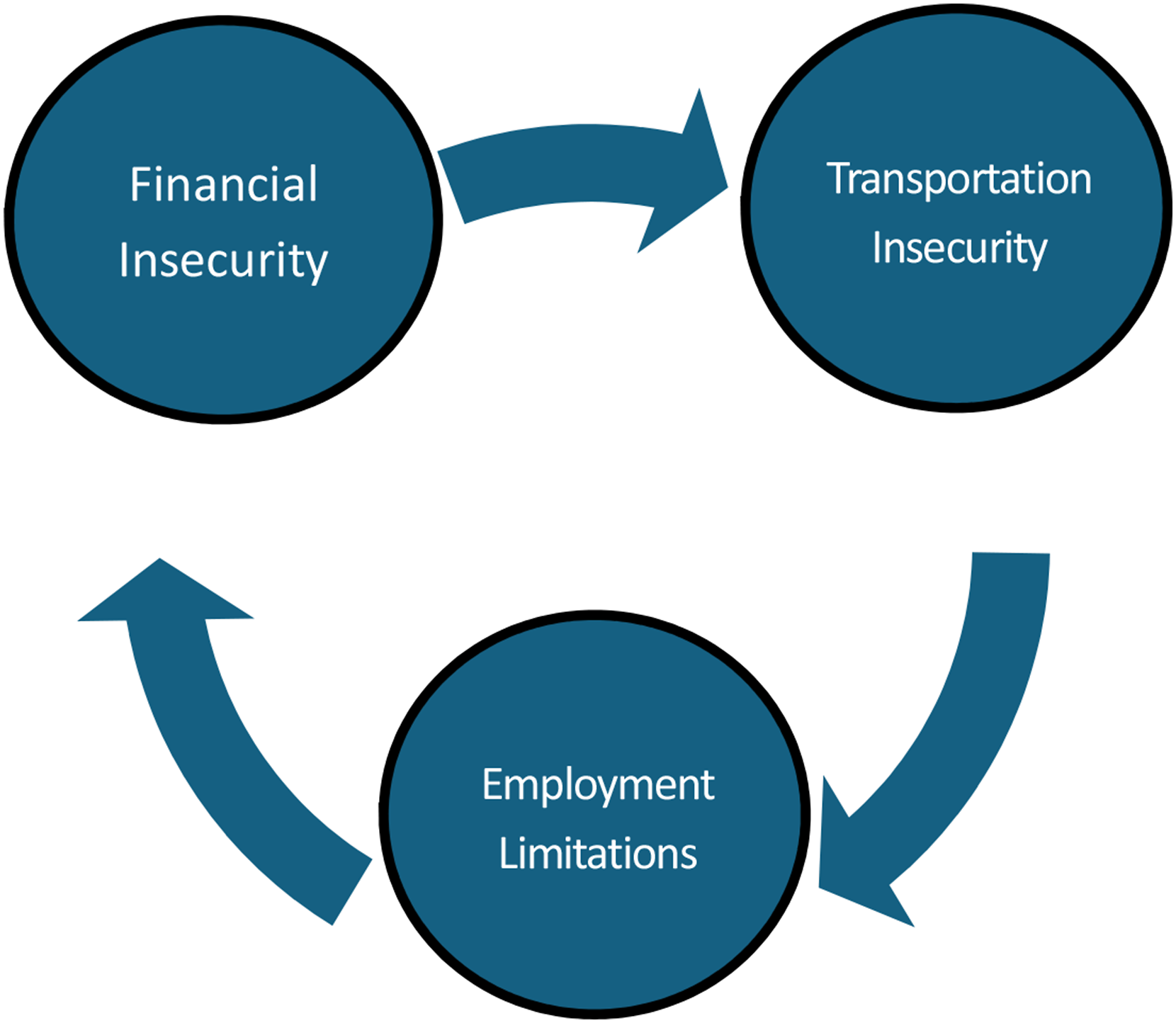
Geographic location can clearly affect access to surgical care. In rural settings, general surgeons often perform a broader scope of surgeries due to limited availability of specialized surgical services. Rural surgeons may have had limited training in these specialized operations which can create disparities in the quality of surgical care. Specialized surgical services, including neurosurgery, cardiothoracic surgery, and vascular surgery are performed less often in rural communities. 11 Overcoming geographic disparities rely on many of the same social determinants of health such as transportation and financial security. Compared to an 88% driver rate in the general population, only 65% of people with disabilities drive. In addition, 13% of people with disabilities do not own or lease a vehicle, compared to only 4% of people without disabilities. 12 These differences in vehicle access and ownership contribute not just to the ability to receive care but also to the ability to have appropriate pre- and postoperative care. In geographically segregated areas, subspecialists may not be equipped to accommodate patients with disabilities. Even in more populated areas, studies have found that subspecialists are less able to care for patients with mobility impairments. 13 Geographic constraints including decreased access to specialized surgical care contribute to the challenges faced by patients with disabilities.
Specialized physical structures are often necessary for many patients with disabilities. In a retrospective cohort study Rafaqat et al showed that major disparities in surgical outcomes exist due to the lack of appropriate facilities such as ramps, screening equipment, weighing scales, or examination tables. 14 It is important that hospitals and clinics take these important accessibility needs into consideration. In operating rooms and throughout the perioperative time there can be specific surgical schedules to adhere to. Appropriate planning by the surgical team can help prevent barriers before, on, and after the day of surgery. For example, neck and back pain is common in many patients with physical disabilities. Because this may make supine positioning more uncomfortable, the surgical team should plan for alternate methods of positioning prior to the day of surgery. 15
Patients with sensory disabilities related to communication such as those who are deaf or blind, can experience challenges throughout the surgical process that may lead to worse outcomes. For patients that are deaf or mute, sign language specialists or other devices may be able to assist in all perioperative care. This can include things related to surgery but also can include communication on how to express pain using a visual analog scale. 16 Poor assessment and treatment of postoperative pain can cause physical and psychological disturbances which can include hemodynamic instability and delayed gastric emptying. Unfortunately, language specialists may not be readily available in every institution. Without language specialists, patients may not be able to sufficiently understand the key risks and benefits of the procedure they need. Patients also may not understand key preoperative instructions, such as preoperative testing, bowel prep, antibiotics, or not eating after midnight before surgery. These things can negatively affect not just the outcome of surgery, but the ability to perform the surgery. Poor understanding of postoperative pulmonary physiotherapy including incentive spirometry can result in atelectasis and subsequent pneumonia. 16 Similar challenges are faced with the visually impaired who may be unable to follow demonstrations like how to use an incentive spirometer or perform ostomy bag changes.
Surgical Care Delivery
Patients with disabilities needing emergent surgery have higher rates of several negative sequelae including higher rates of readmission, increased infectious complications, and longer hospital and ICU stays. Abdominal procedures such as small bowel resection, ostomy creation, and exploratory laparotomy are associated with even higher readmission rates in the disabled population. Fortunately, more straightforward procedures such as hernia repairs, cholecystectomies, and appendectomies have lower complication rates. Several factors contribute to these disparate outcomes including the access barriers we have already discussed as well as communication barriers. Communication problems faced by patients with disabilities can be acute or chronic and can involve mechanical phonation difficulties or more central cognition problems. Patients may be unable to articulate needs or can have a limited understanding of their perioperative and postoperative instructions which can complicate their care.17-19
Few studies focus on the complex postoperative complications in populations with disabilities. A nationwide population-based study in Taiwan found that patients with intellectual disabilities had longer hospital stays, increased intensive care admissions, and higher rates of complications including pneumonia, bleeding, renal failure, and septicemia. 17 It is important to note that some disabilities can cause problems not directly related to their surgical care. For instance, patients with neurocognitive disorders face an increased risk of postoperative aspiration pneumonia due to impaired swallowing. 18 Because complications can be multifactorial, specialized surgical care and robust care coordination become a necessity for some patients with disabilities. 19 In a robust system, this can include dedicated case managers that can help patients navigate through all aspects of their procedure.
Beyond physical complications, the psychosocial impact that poor access to surgical care can have on patients with disabilities is profound. Those who experience a difficult postoperative course are at a heightened risk of anxiety and depression, with long-term mental health consequences that can persist for more than 12 months. 20 The historical mistreatment of marginalized groups, including patients with disabilities, has contributed to a deep-seated mistrust in the health care system, making it essential to address these systemic issues to ensure equitable surgical care not just for them but for all patients. 21
Solutions
The American Disabilities Act (ADA) was enacted in 1990 with Amendments made in 2008. It mandates that healthcare facilities must provide equal access to healthcare for all patients. Unfortunately, many physicians are not aware of ADA regulations.22,23 In physician practices where there is awareness of ADA regulations, physicians report lack of adherence including lack of equipment that can accommodate their patients with disabilities. Cost is commonly quoted as a barrier to providing necessary equipment and services 24 but when analyzed, the problem is usually more related to inappropriate budgeting. Without modified codes for patients with disabilities or extended appointment times, the costs required to accommodate patients with disabilities are not appropriately reimbursed. This places an unreconcilable financial burden on facilities and providers. Clinical guidelines for the perioperative care of patients with disabilities are also lacking. This makes specialized care an impossibility. Additionally, surgical quality metrics typically focus on postoperative courses of able-bodied patients and do not consider differences that may exist with patients with disabilities. Quality metrics fail to value accessibility which makes it less of a priority. 25 To improve, surgical teams can be trained on ADA policies, health care systems can be evaluated for ADA compliance, and electronic health record resources can be developed to highlight disabled patient needs prior to arrival for care. Surgical societies can address the lack of guidelines for patients with disabilities and advocate for coding that enables for additional time and reimbursement for accessible equipment. 26 Patient reporting cannot be the sole way that accessibility compliance is monitored. Patient advocacy systems can be created to focus on ADA shortcomings while also providing accessibility improvements throughout health care systems. 27
Providing thoughtful and inclusive accommodations in surgical facilities can significantly improve both the experience and outcomes for patients with disabilities. This is because increasing justice and decreasing disparities have been shown to improve the health of marginalized communities. For people with mental health or sensory processing disorders and for those with cognitive disabilities, quiet waiting areas can reduce overstimulation and pre-surgical anxiety. 28 Wheelchair users benefit from having designated, discreet storage areas in patient rooms to allow for convenience and unobstructed movement. 29 Additional access improvements include bi-directional bathroom doors for wheelchair navigation and ceiling-mounted lift devices to help transfer patients with mobility impairments. 30 Operating rooms should be designed with accessibility in mind by incorporating wider doorways, having adjustable surgical beds and overhead transfer systems, and installing intercom systems that provide both visual and auditory alarms.31,32 By adopting universal design principles, surgical facilities can ensure that all patients, regardless of disability status, receive the accommodations they need to feel safe, supported, and comfortable. This leads to both better outcomes and a more positive patient experience.
Surgical Training and Education
Addressing the need for comprehensive training on the care of patients with disabilities is crucial to reduce the health care disparities that this population faces in an ongoing basis. 33 Research indicates that more than half of physicians are unaware of their implicit biases toward people with disabilities. These biases often contribute to poorer health outcomes for disabled individuals even including overall shorter life expectancy.34,35 Longitudinal disability competency training should be added to medical education for both residents and medical students. This training should cover a range of skills, including the proper use of specialized equipment, tools to identify and overcome barriers to care, tailored perioperative management, and trauma informed language specific to patients with disabilities. 32 Training for attendings and hospital staff should also be implemented. These training courses should not just be longitudinal but also consistent, interactive, and organic. By understanding the importance of this, we will help promote an environment centered on inclusive excellence. 36
One efficacious approach to improving disability competency is to integrate the biopsychosocial model of care into surgical education. 37 This model encourages a more holistic understanding of the challenges and experiences patients with disabilities face. It helps trainees to appreciate the patient’s perspective on both physical and psychosocial levels. Implementing adaptive care plans with a multi-disciplinary approach and in collaboration with patient’s families can improve perioperative management. 38 Another valuable approach is to include patients with disabilities in simulation exercises that are embedded in the medical curricula. By doing so, trainees gain hands-on experience with real-world scenarios, further enhancing their ability to deliver compassionate, competent care to all patients, regardless of any disability.
Technology
Several bills were passed in the early 2010s aimed at increasing accessibility to telehealth options. These included the Telehealth Promotion Act of 2012 and the Telemedicine for the Medicare Act of 2013. 39 Shortages in primary care and other specialties will continue to rise because the number of patients entering the healthcare space far exceeds the number of medical graduates each year. Telehealth is designed to facilitate patient care across larger distances. This increase in access to care is particularly helpful for certain populations such as rural, older, medically frail, or patients with disabilities. 39 Telehealth can be used in the clinical setting and in delivery of mental health support or rehabilitation services. 40 Telehealth is only universally helpful if it has the capability for augmentative and alternative communication which is often needed in older and patients as well as patients with disabilities. 41 The integration of augmented telehealth systems can break down the socioeconomic, geographic, and communication barriers that patients with disabilities face. As technology grows, it has the potential to significantly decrease current barriers to care.
Artificial intelligence, machine learning, and deep learning are increasingly useful for a variety of healthcare needs. Machine learning relies on artificial intelligence to simulate human learning. When multiple machine learning networks are combined, they form deep neural networks that are capable of extremely complex tasks. In surgical planning, this can involve evaluating multiple diagnostic modalities to form treatment plans. 42 For patients with disabilities, getting to their appointments can often be hard, so a combination of telehealth and artificial intelligence can help decrease the disparities they face.42,43
Cases
Case study 1
One example of a health system creating an accessibility program is the Cleveland Clinic.44-46 They focused on patients with mobility impairments by implementing physical modifications like adjustable height surgical tables, wider doorways, and accessible restrooms in the perioperative area. They also educated employees about patients with disabilities including those with mobility, sensory, and cognitive impairments. A patient navigator role was created to guide patients with disabilities through all perioperative phases of care. This program led to significant reduction in perioperative complications among patients with disabilities, improved satisfaction scores, and increased surgical throughput for this their disabled population.
Case study 2
Another example of surgical access is a program developed at Massachusetts General Hospital. 47 Their initiative also addressed equipment upgrades by ensuring operating room tables were adjustable with lifts, and preoperative and postoperative areas were fully accessible. Multidisciplinary care teams with disability specialists assisted patients in the surgical planning and recovery process. This initiative helps to enhance surgical safety, reduce postoperative length of stay, and lead to higher satisfaction for patients with disabilities.
Case study 3
The adoption of artificial intelligence (AI) in surgical care for individuals with disabilities is still in its early stages. Institutions broadly have not yet integrated AI into the surgical planning process. However, research indicates that AI and its components—machine learning and predictive models—can be beneficial for both surgeons and patients. The field of neurosurgery is at the forefront of this research. A prospective study utilizing data from patients across 11 states in the United States established a predictive model for adult spinal deformity, achieving an accuracy of 75.4% in predicting length of stay (LOS) within two days. 48 Additionally, a predictive model incorporating twenty variables has been developed that effectively predicts major intraoperative or perioperative complications following adult spinal deformity surgery, demonstrating an accuracy of 87%. 49
In a retrospective review of elective inpatient surgeries within the Transitional Care Program at Brigham and Women’s Hospital, a machine learning algorithm was derived that effectively identifies patients with lumbar disc disorders at risk for non-routine discharge. 50 Some disabilities can hinder a patient’s ability to perform everyday tasks. For these individuals, surgery may be the only option. Because all surgical interventions carry inherent risks, implementation of an AI tools can assist in developing individualized surgical plans that prioritize each patient’s unique needs, ultimately promoting optimal recovery.
Conclusion
Patients with disabilities experience many barriers in access to care that should be recognized so that solutions can be found. Ways to increase accessibility and communication are central to many of the solutions needed. It is important for health care facilities to consider patients with disabilities in the production of all facilities and service lines. Surgery can present unique barriers to care that require specialized solutions. Surgical care and outcomes suffer for patients with disabilities if special attention is not paid to the special needs of these patients with disabilities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.