
Abstract
Background
Solid pseudopapillary neoplasms (SPNs) arising in the body or tail of the pancreas can be amenable to laparoscopic distal pancreatectomy with or without concomitant splenectomy. The purpose of this study was to evaluate laparoscopic distal pancreatectomy for SPN using the Warshaw technique as a means to preserve spleens in children.
Methods
We reviewed our database of SPN patients 19 years and younger (January 2006-December 2023). Five had a laparoscopic Warshaw procedure. Using the volumetric analysis tool in Sectra, a pediatric radiologist calculated preoperative tumor, pancreas, and spleen volumes (including postoperative organ volumes) on computed tomography. Descriptive statistics were performed.
Results
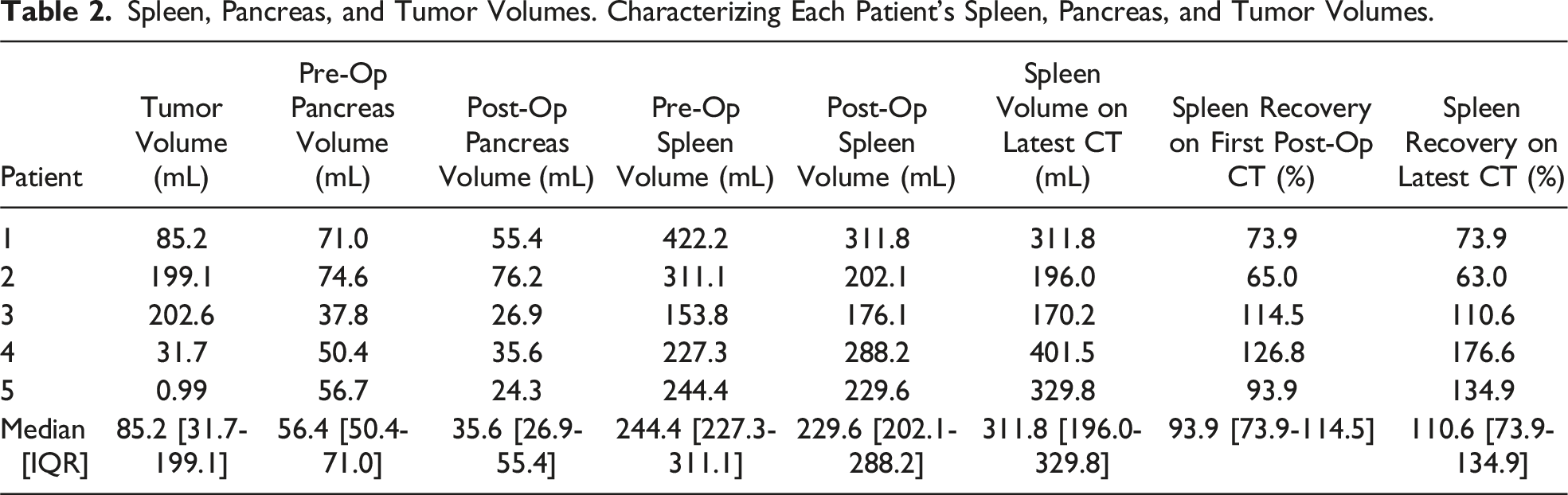
All five spleens were salvaged, although small infarcts occurred centrally in four patients. Splenic volumes on first imaging after Warshaw averaged 93.9% of preoperative size. Splenic volumes were preserved over time, as the most recent scans averaged 110.6% of the preoperative spleen volume. Collateral flow through the short gastric arteries, inferred from dilation on scans, increased in all patients. Median tumor volume was 85.2 mL, and all SPN were resected with negative margins. No relapse occurred (median follow up: 407 days). Median estimated blood loss was 100 mL, median length of procedure was 4.9 hours, and median inpatient length of stay was 3 days. A multimodal pain regimen, including preoperative TAP blocks, non-opiate, and opiate medications, resulted in a median 81 Morphine Milligram Equivalents (MMEs) administered during the hospital stay.
Conclusion
Laparoscopic Warshaw for SPN in children appears highly effective at preserving splenic volume without compromising oncologic fidelity or consuming excess inpatient resources.
• Warshaw principles are applicable to laparoscopic distal pancreatectomy for solid pseudopapillary neoplasms of the body and tail of the pancreas. • This cohort study of five children having laparoscopic distal pancreatectomy for solid pseudopapillary neoplasms, while applying Warshaw principles, showed remarkable potential to preserve spleens durably and to maintain oncologic fidelity.Key Takeaways
Introduction
Solid pseudopapillary neoplasms (SPNs) of the pancreas are rare, comprising 1% of pancreatic tumors, and can arise in children and adolescents. 1 The pathogenesis of the tumor is unknown at the cellular level, although a common feature is activated or nuclear-localized beta-catenin.2-4 SPNs can arise across the entire gland (ie, head, body, or tail), which challenges glandular and splenic preservation while maintaining oncologic integrity.
In the pediatric population, SPNs are the most common tumor of the pancreas; however, these low-grade malignancies rarely affect children, with an incidence of 0.1-0.2 per 1,000,000 pediatric patients aged 0-14 years. 5 SPNs predominantly affect females for unclear reasons. When an SPN is diagnosed in childhood, the tumor often produces symptoms, such as abdominal pain in 47-81% of patients, likely related to ductal obstruction that incites mild pancreatitis, or nonspecific symptoms such as nausea, vomiting, early satiety, anorexia, and weight loss 1 when large and imposing mass effect. Indeed, these low-grade malignancies can become quite large and are located at the head of the pancreas in slightly less than half of cases. Moreover, these tumors tend to parasitize blood supply and drainage from the primary splenic vasculature, which can complicate resection of SPN in any location. 6
For SPN of the pancreas, surgical resection remains the cornerstone of treatment, with a 95% 5-year survival after complete extirpation.1,4 A key consideration when resecting an SPN arising in the body or tail involves preservation of the spleen, which is essential for supporting immune function, especially among the pediatric population who have a lifetime ahead of possible immune compromise and vulnerability to overwhelming post-splenectomy infection. 7 Surgically, splenic preservation is challenging in the context of SPN, as inflammation, desmoplasia, and angiogenesis will increase the difficulty in separating the tumor and the major splenic vasculature, from which its blood supply often is parasitized, and will risk its spill. 6 To avoid these issues of bleeding and tumor rupture, distal pancreatectomy can be accomplished with en bloc resection of the splenic vessels but requires preservation of the short gastric arteries if the spleen is to be salvaged (ie, Warshaw technique). 8 Given the rarity of SPN and other pancreatic tumors in children, little has been published on technical considerations to preserve the spleen in these younger ages when completing a distal pancreatomy, whether through an open or minimally invasive approach. The Warshaw technique requires a careful “double division” of the splenic artery and vein, while meticulously preserving the collateral blood supply to the spleen via the short gastric arteries. Comparatively, the Kimura technique, which preserves the main splenic vessels, primarily relies on a tissue plane between uninvolved pancreas and the vasculature, rendering the Warshaw technique the better option for treating SPNs that tend to generate inflammation and incorporate tributaries from the tumor to the splenic vein. 9 Although typically an open procedure, our center previously reported on efficacy of the MIS Warshaw technique to preserve spleens in two SPN patients. 6
In this manuscript, we are updating the previous series from two to five patients, as well as now evaluating sustainability of splenic preservation over time and documenting the source of collateral blood flow that is physiologic and expected, and should not be considered pathogenic varices. Given the rarity of SPNs in children, and that most current data on the use of the Warshaw technique is reported from open cases among adult patients, we aimed to evaluate the postoperative size and perfusion of the spleen to establish the long-term durability of the procedure, while documenting oncologic fidelity with this approach when applied laparoscopically. We hypothesized that the splenic volume will be preserved over time and is sufficient to allow for preserved immune function in children.
Methods
This single center, retrospective, and descriptive study was approved by the Institutional Review Board under #100734. We reviewed our consecutive database of SPN patients 19 years and younger who had their operation between January 2006 and December 2023. The study identified five patients who underwent a minimally invasive distal pancreatectomy with spleen preservation using the Warshaw technique, of which one was completed robotically. Using the volumetric analysis tool in Sectra, the institutional digital picture archiving and communication system (PACS) imaging system, a pediatric-trained radiologist, blinded to all other data, calculated preoperative tumor, pancreas, and spleen volumes on computed tomography along with measurements from all follow up CT scans by measuring the residual pancreas and entire spleen. The technique involved multiplying the slice thicknesses of each area of interest and summing the volumes from each slice to get the total volume (Figure 1). CT scans were exclusively used as the source of data. Ultrasound imaging, although utilized in patient care, was not used for any volume measurement. Descriptive statistics were performed using Excel software, with data reported as medians with interquartile ranges. Measurement methodology is consistent with those previously reported.
6
Measurement of volumes on CT Scan. (A) Representative preoperative slice highlighting the pancreas body at 12 o’clock, pancreatic mass at 1 o’clock, and spleen at 2 o’clock. (B) Representative postoperative slice highlighting the pancreas body at 12 o’clock, spleen at 2 o’clock, and splenic infarct at 5 o’clock.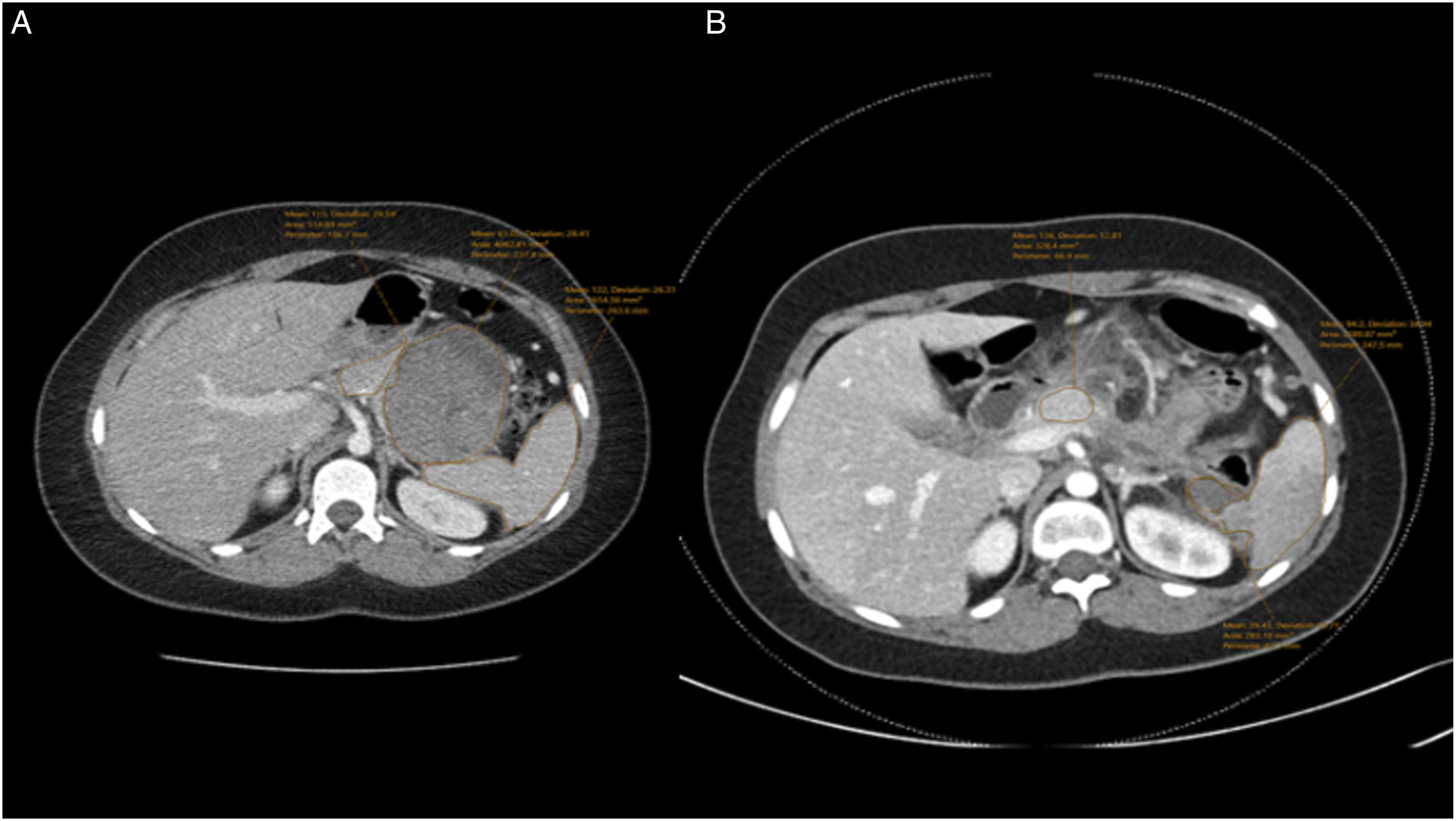
Results
Cohort Description
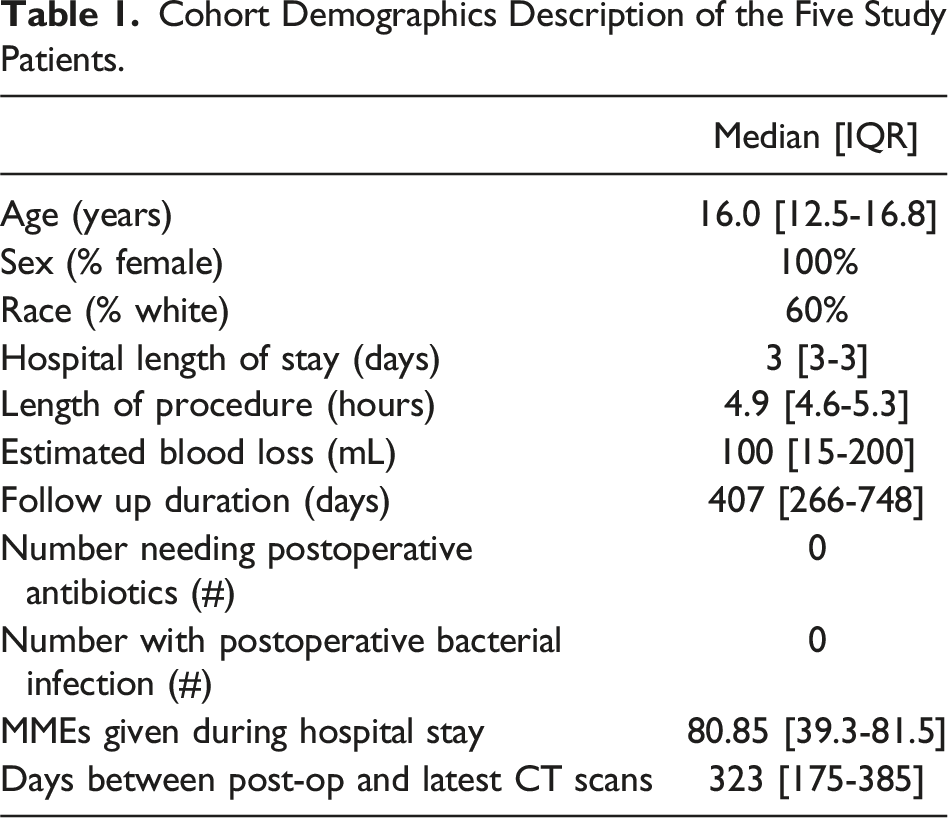
Cohort Demographics Description of the Five Study Patients.
Splenic Preservation, Operative Details, and Imaging Follow up
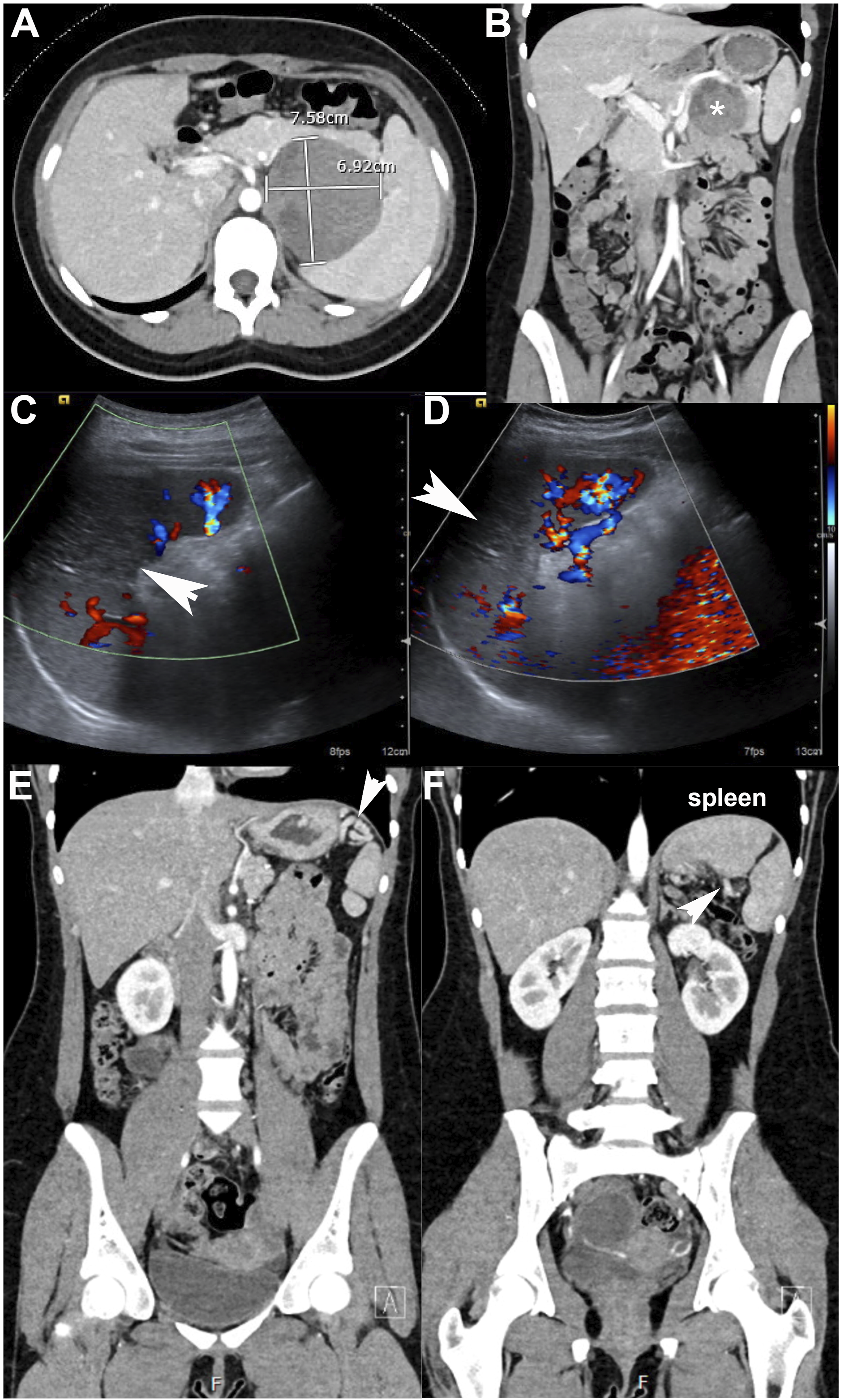
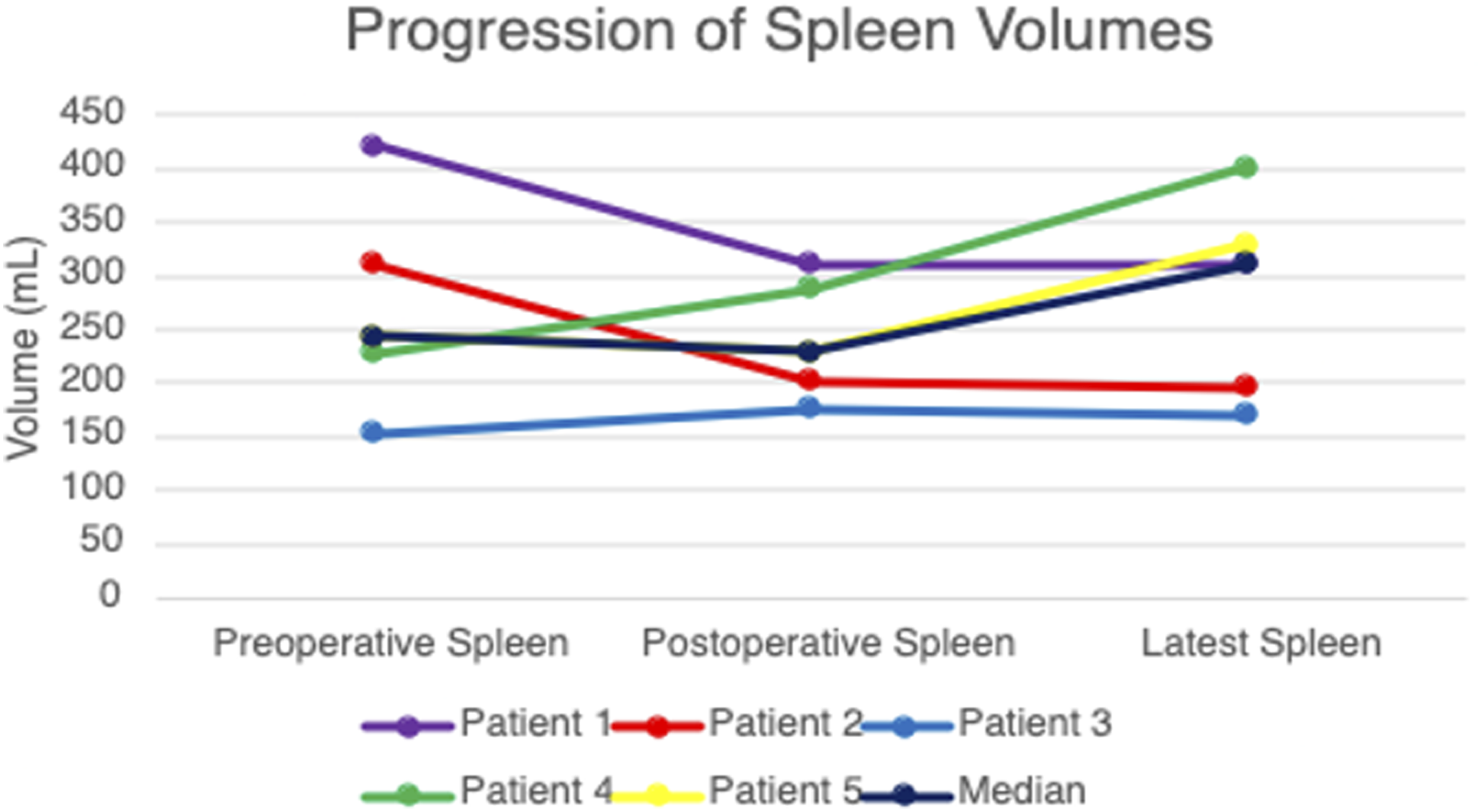
All spleens were preserved in each laparoscopic distal pancreatectomy for SPN using Warshaw principles (Figure 2). On initial postoperative imaging, which was completed a median 22 days [15-91] after the date of surgery, small infarcts occurred centrally in four patients (Figure 3) with median splenic volumes measured at 93.9% [73.9-114.5] of preoperative size (Table 2). Over time, splenic volumes remained stable, as the most recent scans showed a median of 110.6% [73.9-134.9] of the preoperative spleen volume (median CT scan follow up: 323 days [175-385]; Figure 4). Collateral blood flow through the short gastric arteries, inferred from dilation on imaging, increased in all patients. The median operating time was 4.9 hours [4.6-5.3], with a median estimated blood loss of 100 mL [15-200]. Postoperative length of stay was a median of 3 days [3-3], with a median 80.9 MMEs [39.3-81.5] administered during the hospital stay (Table 1). Minimally invasive distal pancreatectomy for SPN applying Warshaw principles in a child. (A) (B) Large distal pancreas SPN (solid pseudopapillary neoplasm) with marked angiogenesis. VB: vasa brevia (ie, short gastric arteries). (C) (D) View of SPN extending through posterior pancreas (P) into retroperitoneum. Splenic vein (SV) coursing through SPN. (E) (F) Window for medial transection of pancreas with splenic vein (SV) already divided with vascular stapler. Meticulous dissection in hilum of spleen to preserve short gastric arteries. (G) Specimen placed in retrieval bag for delivery through extended umbilical incision. (H) Final photo showing stapled edge of pancreas (P), tumor bed, and short gastric arteries extending from stomach to spleen. Progression of the spleen on imaging. (A) (B) Preoperative CT scan shows presumed SPN in body and tail of pancreas extending to hilum of spleen. (C) (D) First postoperative ultrasound (4 weeks) shows good upper and lower pole perfusion to spleen but with small central infarct (arrowhead). (E) (F) Last postoperative CT scan 3 years later that shows return to preoperative spleen volume with small, contracted central scar and collateral blood flow via short gastric arteries (arrowheads). Spleen, Pancreas, and Tumor Volumes. Characterizing Each Patient’s Spleen, Pancreas, and Tumor Volumes. Progression of spleen volumes. All spleens were preserved with recovery of splenic volume over time.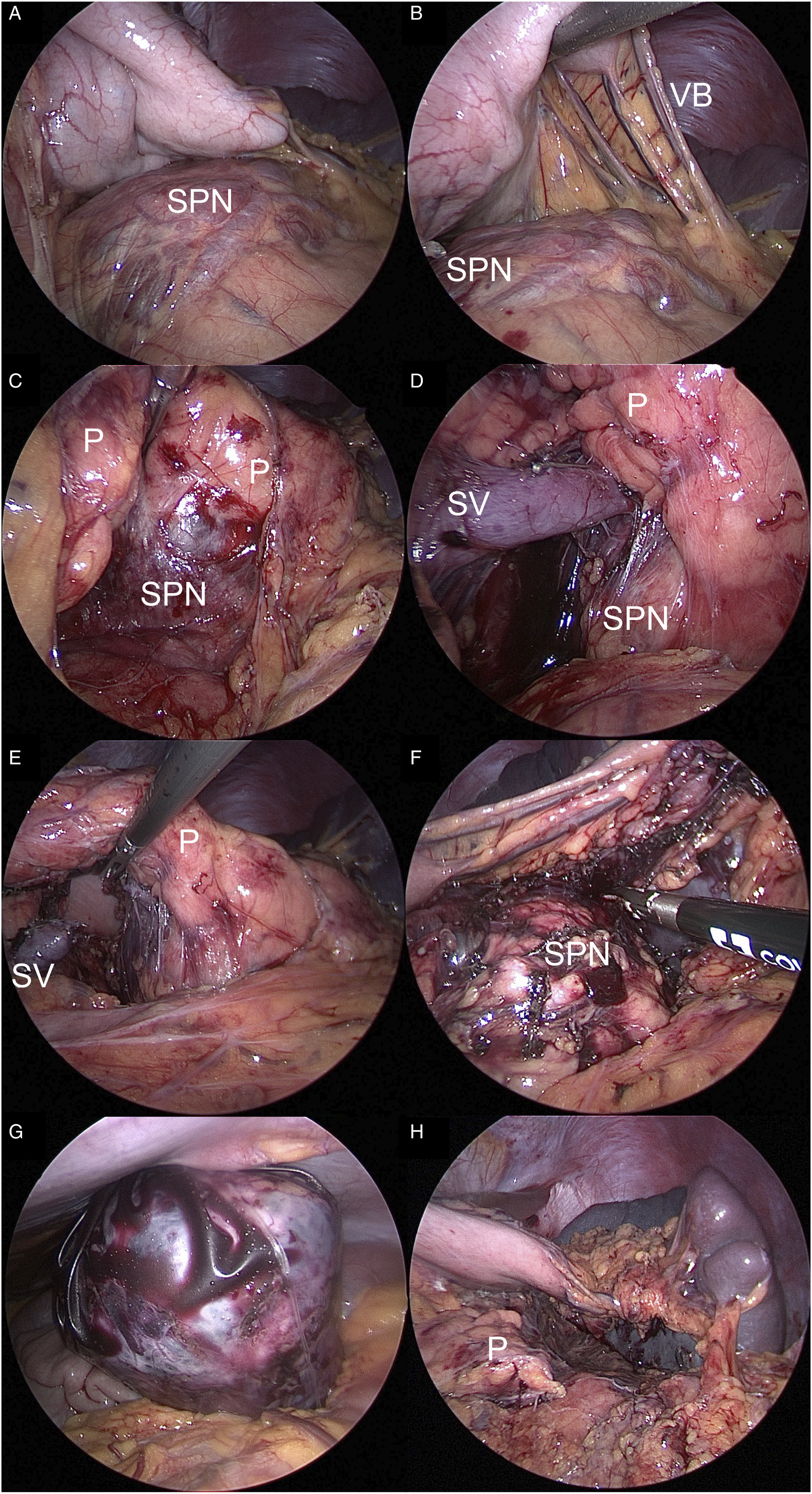
Oncologic Fidelity, Splenic Function, and Diabetes
All SPN were resected with negative margins and without gross tumor spill. No lymph node metastases were identified with a median 6 lymph nodes6,7 evaluated per patient. No relapse occurred (median follow up: 407 days [266-748]). Preoperative pancreas volumes were a median of 56.4 [50.4-71.0], and postoperatively were 35.6 [26.9-55.4]. No instances of a documented bacterial infection have been reported to date, with no patient receiving postoperative antibiotics either. One patient developed diabetes over a year after their procedure for unclear reasons, as the measured glandular volume should have sufficed regarding endocrine function.
Discussion
This study foremost showed that splenic preservation is highly effective when applying the Warshaw principles for distal pancreatectomy in children having SPN and can be completed with meticulous minimally invasive techniques achieving long-term splenic volumes and excellent oncologic fidelity. Albeit single center and relatively small, this study is the most comprehensive reported in children to date using this minimally invasive approach and the only to assess long-term spleen preservation and collateral blood supply.
For all patients, CT scans were obtained preoperatively. Follow up CT imaging was performed typically around four weeks and again roughly one year after resection. Although US was obtained at interval time points, CT imaging was the preference to document collateral blood supply and drainage, as well as to monitor for local relapse. In three patients, the immediate postoperative CT scans showed an initial small reduction in spleen volume compared to preoperative measurements, but this minor injury was followed by enlargement of the spleen on subsequent imaging and was sustained across time. We suspect these minor changes in splenic volumes are due to initial ischemia and remodeling as collateral blood flow is restored via the short gastric arteries, which appeared to dilate physiologically with time. But, variables in patient convalescence from their procedure could impact these subtle, early changes in splenic volume as well. Nevertheless, the splenic hila all appeared well vascularized with initial increases in tortuosity and distension of the short gastric vessels on late postoperative imaging, highlighting the continued splenic perfusion via the short gastric arteries and recruitment of sufficient blood flow to heal any infarct. Over subsequent scans, these collateral vessels remained unchanged after their initial dilation and growth to compensate for the change as primary source of perfusion. Moreover, initial postoperative imaging showed a small central infarct with reduced flow in all but one spleen. All infarcts completely resolved over time on subsequent CT scans or ultrasounds. These results are similar to those from Zhou’s 2024 study where all infarcted spleens recovered within 12 months. 10 For the patients whose compensatory spleen volumes were greater than their comparative preoperative spleen volumes, this observation may be explained from ischemia-induced organ growth or alternatively from secondary edema and/or venous congestion.
A critical assumption made in this study is that splenic volume and recovery from infarct translates to adequate splenic immune function. To date, there is no report on the effects of spleen preservation applying Warshaw principles on preventing overwhelming infection. 11 However, Wang et al have investigated platelet count, lymphocyte grouping, immunoglobulins, and serum tuftsin levels as markers of splenic immune function and noted no difference compared to healthy controls regarding these values. 12 Investigating specific markers of spleen immune activity in a prospective study would be useful to identify whether splenic immune function continues to be preserved. For our patient population, we ensured that all received splenectomy vaccines preoperatively, and we recommend other centers do the same for any distal pancreatectomies with en bloc resection of the splenic vessels while preserving the short gastric arteries.
Importantly, oncologic fidelity with this spleen-preserving approach was maintained over time. A pediatric-trained pathologist analyzed all surgical specimens carefully to confirm the diagnosis of SPN and to document negative tumor margins and lymph node involvement. Patients were scheduled for follow up imaging via US or CT scan to monitor for relapse in addition to the spleen perfusion. Patient recovery from this minimally invasive surgical approach also was optimized by utilizing a multimodal pain management strategy, including TAP blocks, non-opiate alternative pain medications to minimize opioid use. With these strategies, patients experienced a relatively short hospital stay with no documented bacterial sepsis in this series.
Of the five patients, only one developed diabetes, which emerged over a year after their procedure. The patient is undergoing workup to determine whether this is type I or type II, and we do not have evidence that this diagnosis is related or not to their distal pancreatectomy.
The authors acknowledge several limitations with this cohort study. First, it is a single center study of only five patients. That said, SPN occur rarely in children with roughly half being amenable to distal pancreatectomy, which together limit broader experience with these documented techniques herein. During this manuscript review process, we have completed two additional Warshaw procedures in young adolescents having a distal SPN with successful spleen preservation, but these patients have yet to attain sufficient follow up for inclusion in this case series. Nevertheless, this series afforded the opportunity to detail sustainability of splenic salvage applying Warshaw principles, to outline the evolution of collateral blood flow through the short gastric arteries, and to characterize how an early, small central infarct can be expected but resolves within a brief time period. Second, the authors acknowledge that this advanced minimally invasive approach for a low-grade malignancy may only be applicable for surgeons with specific skills in pediatric surgical oncology and who practice at quaternary children’s hospitals. Lastly, the postoperative imaging protocol was not standardized across this patient population. Each patient had a different number of follow up imaging studies and were occasionally followed up with ultrasound imaging as opposed to CT scans. This protocol can be standardized at our center for future studies, and we recommend other centers consider the same. This study emphasizes that the Warshaw technique as a means of spleen preservation when performing distal pancreatectomy for SPN can be accomplished successfully and minimally invasively in the pediatric population. As more data are collected, this technique should be investigated in a multi-center fashion with a larger patient population to verify durability of the approach and to document splenic immune function more precisely.
In summary, the authors assert that the Warshaw principles can be applied to minimally invasive distal pancreatectomy for SPN in the pediatric population, as it allows maintaining of strict oncologic principles, while preserving the spleen and pancreas.
Abbreviations
Solid pseudopapillary neoplasm
Minimally invasive surgery
Distal pancreatectomy
Warshaw procedure
Spleen preservation
Footnotes
Authors Contribution
R.C.: formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization, and project administration. C.K.: methodology, formal analysis, and writing—review and editing. N.J.: methodology, formal analysis, and writing—review and editing. H.M.: methodology and writing—review and editing. C.H.: resources and writing—review and editing. S.M.: Investigation and writing—review and editing. Z.I.: methodology, resources, writing—review and editing, and supervision. L.H.: conceptualization, methodology, writing—original draft, writing—review and editing, visualization, supervision, and project administration.
Authors Note
This study was presented orally in the Oncology Session at IPEG 2024.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.