
Abstract
Cardiac injuries pose challenging diagnostic and management dilemmas. Cardiac trauma can be classified by mechanism into blunt and penetrating injuries. Penetrating trauma has an overall higher mortality and is more likely to require operative intervention. Due to the lethality of any cardiac injury, prompt diagnosis and treatment is critical for survival. The initial management of suspected cardiac injury should start with Advanced Trauma Life Support (ATLS) protocols followed shortly by directed diagnosis and management, which usually begins with a focused assessment with sonography in trauma (FAST) examination. In contrast to traditional ATLS protocols, some centers have adopted an assessment of “circulation before “airway” and “breathing”; however, this is an evolving concept. In this article, we provide an overview on the management of penetrating and blunt cardiac injuries, including use of physical exam, laboratory tests, imaging, and surgery.
Penetrating Cardiac Injury
Incidence
Penetrating cardiac injuries are primarily the result of a stab or firearm injury, 1 although they may also be related to other impaled foreign objects.2-4 The right ventricle is the most commonly involved chamber due to its anterior position within the chest. This is followed by the left ventricle and right atrium. 5 The coronary arteries are also at risk for injury with the left anterior descending (LAD) most frequently involved (87.5%) followed by the right coronary artery (RCA).
The location and mechanism of injury correlates with survival. A study by Tang et al reported a survival rate of 31% for right ventricular wounds, 26% for left ventricle, 20% for right atrium, and 5% for left atrium injuries respectively. This is in part due to an increased rate of concomitant injuries (ie, injuries to other cardiac chambers and/or the great vessels), as well as complex defects in patients sustaining atrial trauma. 5 The presence of cardiac tamponade is also associated with a higher survival rate, which may be attributed to the fact that it can be expeditiously treated with surgical intervention. 6 Patients with cardiac gunshot wounds have lower survival compared to stab wounds, with rates between 16-43% reported in the literature.6-8 This is due to a combination of increased risk of multi-chamber injuries, concomitant mediastinal injury, and increased force/velocity associated with firearms.5,8
Diagnosis
The diagnosis of penetrating cardiac injuries should be initially predicated on the location of wounds and clinical stability. Hemodynamically stable patients can undergo an extensive workup while the unstable patient requires emergent surgical intervention with transport to the operating room as soon as feasible (Figure 1). Cardiac trauma can present in three ways: hemorrhagic shock, pericardial tamponade, or cardiac failure. Injury within the cardiac box (defined as the space bordered by the clavicles and sternal notch superiorly, the midclavicular lines laterally, the costal margins inferiorly and these borders projected posteriorly to the back) should raise suspicion for penetrating cardiac trauma; however, vigilance must remain even with wounds located outside of this region, especially gunshot wounds.9,10 Highlighting this, Kim et al analyzed the incidence of cardiac injury following wounds within and outside the cardiac box at a single Level 1 trauma center and found that stab wounds within the cardiac box were associated with a higher risk of cardiac injury (14.3% vs 2.4%) while there was no statistical difference in incidence for patients with gunshot wounds within or outside the cardiac box (9.1% vs 3%, P = 0.32). Algorithm for penetrating cardiac injury.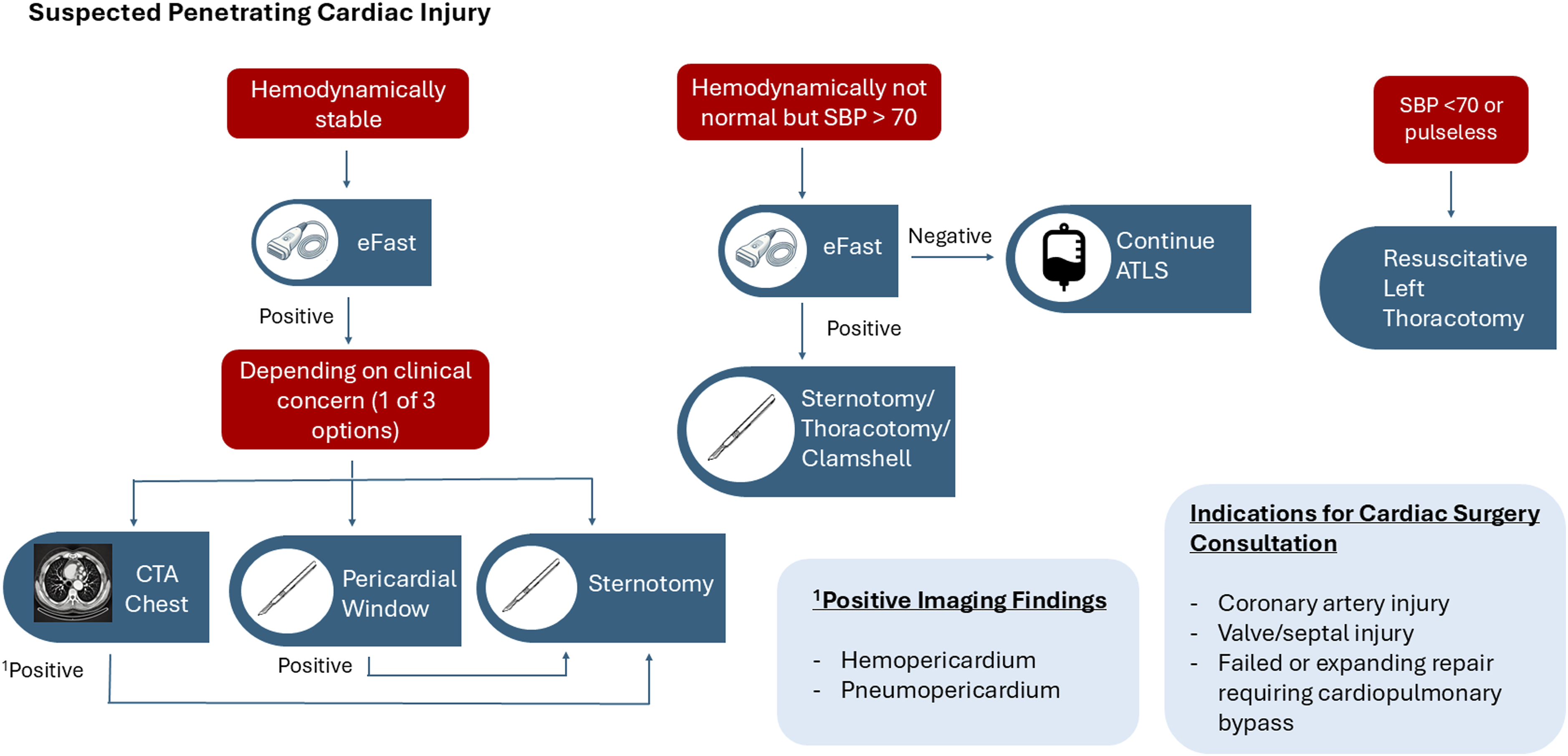
Beck’s triad of hypotension, muffled heart sounds and distended neck veins can be suggestive of cardiac tamponade; however, this is only present in at most 10% of all patients with tamponade, with a much lower number of trauma patients having this combination of findings. 11 This is due to the potential for concomitant hemorrhagic shock from blood loss elsewhere and the relative infrequency of each clinical finding in the setting of a pericardial effusion. Stolz et al reported individual sensitivities of muffled heart sounds ranging from 18.5% to 61.4%, jugular venous distension ranging from 2.7% to 10.9%, and hypotension leading to a diagnosis of tamponade ranging from 18.5% to 61.4%. 12
Ultrasound as part of the focused assessment with sonography in trauma (FAST) exam has proven to be an effective method of diagnosing pericardial fluid in the setting of trauma. It has a sensitivity ranging from 56-90% and a specificity from 92%-96% with a negative predictive value of 93% for diagnosing occult penetrating cardiac injury.8,13 However, the accuracy of ultrasound can be confounded by a left hemothorax, as this may signal a cardiac injury that is evacuating into the left thorax and thus may not have a pericardial effusion on ultrasound imaging. 14 Furthermore, ultrasound may not be readily available at every institution and the results are operator dependent.15,16 If the FAST is equivocal and the patient remains hemodynamically stable, options for management purported by the Western Trauma Association (WTA) penetrating thoracic injury algorithm include video assisted thoracoscopic surgery and/or a pericardial window. 17 Alternatively, a computed tomography scan may be completed to evaluate the trajectory and help assess for injury within the mediastinum as pneumopericardium or hemopericardium can also be suggestive of cardiac injury. 18 Hounsfield units (HU) can be used to differentiate between a transudative effusion and acute hemorrhage. 19 The HU for acute hemorrhage is typically 30-45; however, clotted blood can have a higher HU between 50-100.19-21 Extravasated contrast due to continued active bleeding from a laceration will have HU > 180. 19
Management
Hemodynamically Normal Patient
Hemodynamics remains the main initial determinant of algorithms for cardiac trauma. However, parameters such as the quantified size of pericardial fluid, laboratory evaluations, and/or clinical exam may help guide treatment. If the patient is hemodynamically stable and workup is suggestive but not definitive for cardiac injury, a pericardial window can be performed to confirm the diagnosis. The sensitivity and specificity of the subxiphoid pericardial window ranges from 92-100% and 95-100%, respectively. 22 Performance of this procedure includes starting with a 5-6 cm vertical incision made over the xiphoid process. Dissection is carried through deeper tissues and the linea alba. The xiphoid process may be resected for improved pericardial exposure if needed. The sternum is retracted anteriorly and the pericardium is grasped and opened with scissors. Oftentimes, the tense pericardium, as in the case of pericardial tamponade, can be challenging to open with scissors. In this situation, the use of a scalpel is recommended. Care should be made to optimize visualization including a lighted retractor or headlamp during this critical step. Historically, the presence of any hemopericardium mandated sternotomy; thus, the presence of a false positive could increase patient morbidity. More recent studies have put forth an approach where a small amount of hemopericardium can be irrigated and monitored for active bleeding as it may represent a minor self-limited cardiac, pericardial or anterior mediastinal injury.23,24 This has not met widespread adoption in resource-rich settings such as the United States due to concerns for delayed hemorrhage resulting in a potentially preventable death. Notably, the pericardium can also be exposed trans-abdominally via an open or laparoscopic approach with similar effectiveness in the setting of concomitant abdominal exploration.25,26
Hemodynamically Abnormal Patient
Patients who present with or go into cardiac arrest should undergo an emergency department (ED) thoracotomy when indicated. WTA guidelines recommend ED thoracotomy for patients with penetrating thoracic trauma with less than 15 minutes of prehospital cardiopulmonary resuscitation (CPR) and less than 10 minutes of prehospital CPR for blunt thoracic trauma. 27 The Eastern Association for the Surgery of Trauma (EAST) guidelines for ED thoracotomy are predicated on the presence of signs of life. There is a strong recommendation for ED thoracotomy in patients who are pulseless with signs of life after penetrating thoracic trauma. Conditional recommendations for ED thoracotomy include patients who are pulseless without signs of life after penetrating thoracic or extra-thoracic trauma and patients who are pulseless with signs of life after penetrating extra-thoracic trauma and blunt injury. 27 To perform a resuscitative ED thoracotomy, an incision is made in the left 4th or 5th intercostal space starting at the lateral border of the sternum and extending to the bed along the curve of the ribs (upward towards the axilla). The chest is opened and the inferior pulmonary ligament is taken down to allow retraction of the lung. In the event of cardiac arrest, the descending aorta should be cross-clamped, taking care to avoid injury to the esophagus. The pericardium is sharply opened (oftentimes with a scalpel if the pericardium is tense and cannot be grasped) anterior and parallel to the phrenic nerve, tamponade is released and the heart is delivered. The heart can then be examined for signs of injury and/or performance of cardiac massage. Injuries can be temporized using digital pressure. There are some reports of the use of adjuncts for hemorrhage control such as balloon occlusion or control with a sterile skin stapler prior to transport to the operating room for definitive repair.28-30
Survival rates following ED thoracotomy are highest in patients with penetrating cardiac injuries compared to all other thoracic or abdominal injuries. 31 However, one study from a trauma registry in Atlanta found the need for an ED thoracotomy was an independent predictor of mortality in patients with penetrating cardiac injury. 8 Time to intervention particularly in the setting of hemodynamic instability was also found to correlate with mortality. 32 Another study demonstrated that patients had a higher survival rate if their surgery was performed within 30 minutes of arrival. 5
Current WTA guidelines recommend proceeding to the operating room for a median sternotomy or a left anterolateral thoracotomy in hemodynamically unstable patients with a positive pericardial FAST. 33 Choice of incision depends on suspicion for location of injury. Lateral or posterior injuries are better approached via a thoracotomy as described above. Alternatively, the median sternotomy offers excellent anterior penetrating injury exposure as well as overall exposure, including visualization of the heart and anterior mediastinum. Following sternotomy, the pericardium should be lifted with forceps and opened with scissors. As previously mentioned, if the pericardium is tense from distension, then it can be incised with a scalpel and the opening can then be extended with scissors. Anterior injuries can be easily identified and addressed by suture repair with a polypropylene non-absorbable suture with a pledget (ie, pericardium, polytetrafluoroethylene (PTFE), or felt) on a large needle. Posterior injuries can be identified by lifting the heart, keeping in mind that this may induce bradycardia, hypotension and/or cardiac arrest due to impaired venous return. Short periods of cardiac arrest might be tolerated and can assist with wound closure but long periods of cardiac arrest should be avoided. To minimize the risk of hemodynamic compromise with this maneuver, the heart can be sequentially elevated with laparotomy pads to allow adaptation to positional change. If this is not feasible then consideration for cardiopulmonary bypass is warranted. 34
Direct to Operating Room Resuscitation for Cardiac Trauma
Several trauma centers have developed a protocol for direct to operating room (DOR) resuscitation to accelerate surgical management of patients who might have previously succumbed to their injuries. 35 The most common criteria resulting in DOR activations were penetrating mechanisms to the cardiac box. Time from injury to definitive management is an independent predictor of survival for penetrating cardiac injury, particularly those with isolated cardiac injuries and tamponade who may most benefit from a DOR protocol. 5
Techniques for Definitive Repair
Atrial injuries can be repaired by placing a Satinsky clamp under the injury. The defect can then be closed using running 5-0 or 6-0 prolene suture in a horizontal mattress fashion. 29 If the atrial walls are thin, pledgets or autologous pericardial patches can be used to reinforce the repair.
Simple ventricular lacerations can be repaired with 3-0 or 4-0 polypropylene suture in a horizontal mattress configuration. 29 The horizontal mattress approach serves to minimize risk for injuring a coronary artery. The suture needle must be passed under and beyond the coronary artery and then secured in a horizontal mattress fashion. Immediate discoloration of the tissue, dyskinesia, or arrythmia should prompt removal of the suture. Pledgets may help reinforce repairs and minimize blood loss although they are generally not necessary in the left ventricle due to the thicker myocardium. While there is no consensus needle for cardiac injury repair, many recommend use of a tapered needle (eg, MH).28,29
The general approach to coronary artery injuries is to ligate small branches or distal vessels while bypassing proximal injuries. 29 If ligation is performed, the myocardium should be closely observed for signs of cardiac arrythmia, ischemia or infarction. Major injuries to the proximal LAD artery, circumflex, diagonal, or RCA should prompt cardiac surgery consultation for bypass. The left internal mammary artery is often the conduit of choice in an elective coronary bypass; however, its use can be limited in the setting of an emergent thoracotomy or active myocardial infarction. Saphenous vein is the most commonly employed graft for emergency situations as it can be harvested more expeditiously than a mammary or radial artery. 36 One aspect of surgical management that may impact complications is the closure of the pericardium following repair. Some authors recommend closure to minimize risk of cardiac injury during re-entry should the patient require repeat sternotomy in the future, whereas others cite increased risk for pericarditis/tamponade even in the setting of drain placement and thus favor not closing the pericardium.29,37 Regardless most authors recommend placement of a mediastinal drain (eg, 24-32 French chest tubes) and evaluation of the pleura with tube thoracostomy placement if violated. 28
Most repairs can be performed without cardiopulmonary bypass (CPB). Indications for repair of penetrating injury using CPB in the acute setting include proximal injury to the main coronary arteries, failure of repair or expansion of the defect with attempted repair and valvular injury resulting in hemodynamic compromise. 30 Intraoperative cardiothoracic surgery consultation should be obtained whenever CPB is required. However, trauma surgeons should always remain open to cardiothoracic surgery consultation at any point where their expertise may be helpful. Johnson et al examined national trends of the use of CPB in the setting of cardiothoracic trauma. This amounted to 1% of patients with cardiothoracic injuries undergoing surgery over a five-year period. The most common procedures performed in this setting were coronary vessel repairs (65%) followed by non-valvular and non-septal repairs (35%). 34 While in-hospital mortality was lower in the group undergoing repair with CPB, these patients had an increased rate of in-hospital complications included cardiac arrest, pneumonia, stroke, deep vein thrombosis, acute respiratory distress syndrome, and unplanned returns to the operating room.
Postoperative complications following penetrating cardiac injury repair include valvular injury, pericarditis, pericardial effusion/hemopericardium with or without tamponade, as well as mediastinitis. Thus, the American College of Cardiology recommend that patients undergo formal transthoracic echocardiography (TTE) to evaluate for wall motion abnormality, valve dysfunction, and/or pericardial fluid. 38 This can be followed by transesophageal echocardiography (TEE) if the TTE windows are suboptimal. On the other hand, TEE can be the initial evaluation for intraoperative concerns if a provider skilled in TEE is available. Prior studies on this topic have identified pericardial fluid as the most common immediate postoperative finding followed by wall motion abnormalities.5,39 Valvular dysfunction should merit immediate cardiac surgery consultation. Post-traumatic pericarditis is a rare occurrence and an oftentimes self-limiting condition that is treated with nonsteroidal anti-inflammatory drugs (NSAIDs) or colchicine. Most patients (89%) develop post-traumatic pericarditis within the first month. 40 Diagnostic criteria for post-traumatic pericarditis include fever, pleuritic chest pain, pericardial rub on auscultation, and/or pericardial effusion. ECG changes can be seen in up to 20% of patients with diffuse ST-segment elevations in association with PR depression being the most common finding. Laboratory testing should include a C-reactive protein (CRP), serum troponin T or I, and an erythrocyte sedimentation rate (ESR). One of these markers is elevated in at least 83% of patients with pericarditis. 40 All patients with suspected post-traumatic pericarditis should undergo a TTE to evaluate for pericardial effusion. Delayed pericarditis due to retained foreign body (eg, bullet) warrants median sternotomy and removal of the inciting foreign body. 41
Blunt Cardiac Injury
Incidence
AAST Blunt Cardiac Injury (BCI) Grading Scale.
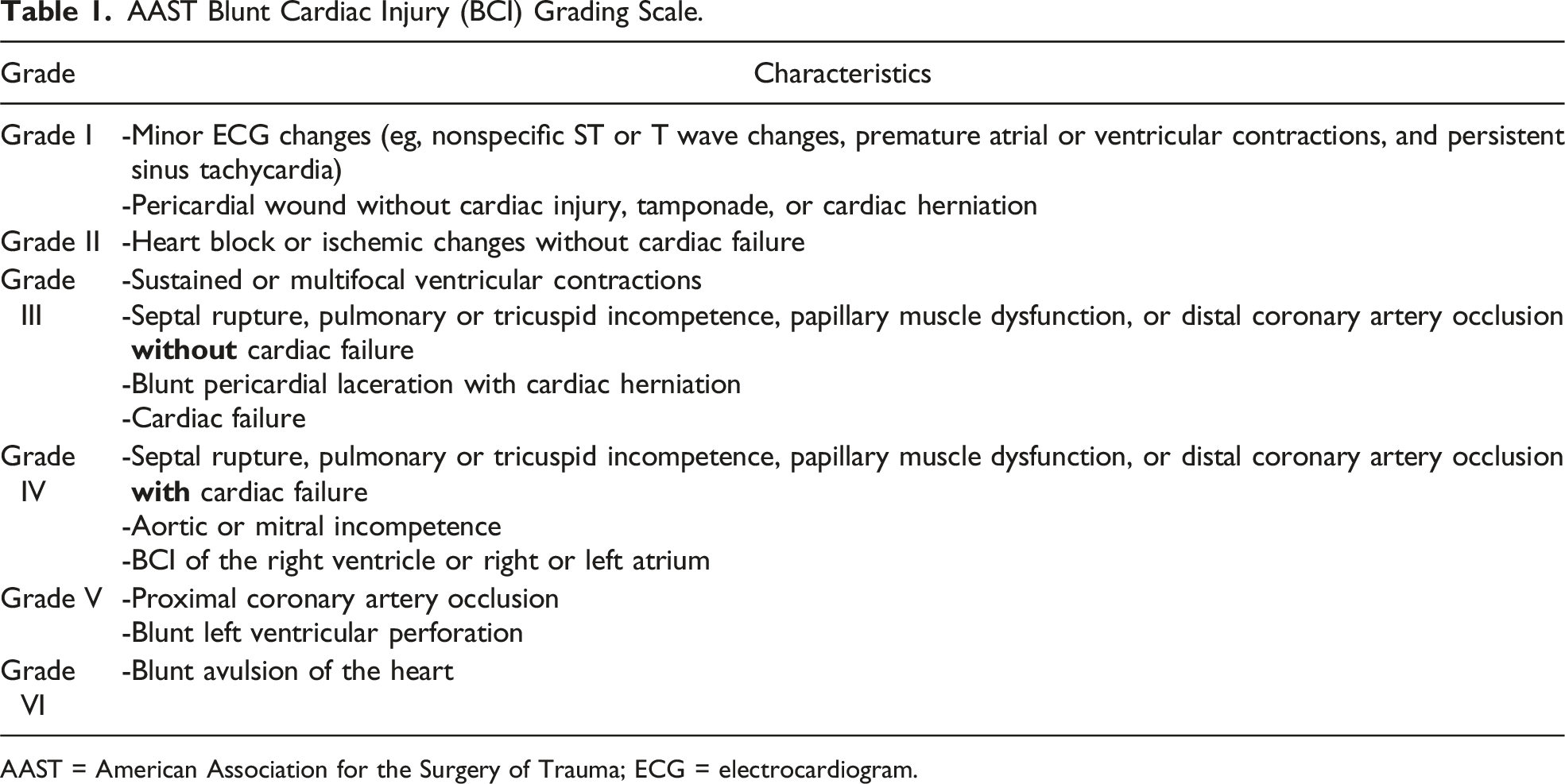
AAST = American Association for the Surgery of Trauma; ECG = electrocardiogram.
BCI may best be divided into mechanical injury to structures of the heart or electrical injury resulting from blunt force or secondary to a structural injury. Structural injuries include disruption of any portion of the heart, from the wall and coronary vessels to internal structures such as valves or chordae tendinae. Blunt coronary artery injury is extremely rare and occurs as direct impact leads to intimal disruption and thrombosis. 52 This is almost always associated with severe myocardial contusion and most commonly affects the LAD artery given its location in the anterior mediastinum. 43 This can subsequently lead to myocardial infarction, arrhythmia, ventricular failure, or delayed ventricular rupture. 53 Valve injuries are also very rare and typically occur when blunt force coincides with systole. This force results in valve, chordae tendinae, or papillary muscle rupture. The aortic valve is the most commonly affected followed by the mitral valve, although any valve injury is reported in less than 5% of post-mortem examinations of BCI patients. 54 Presentation depends on the valve affected and severity of the injury. For example, a small injury to the aortic valve could present with syncope or angina, while a large injury may result in rapid and severe cardiac failure. A murmur may or may not be present, thus these injuries are more reliably diagnosed with an echocardiogram.55-57 Pericardial rupture, also quite rare, may be the most severe form of BCI as it occurs from such a substantial force that the pericardium tears. This tear usually occurs in parallel to the phrenic nerve and can lead to herniation of the heart into the thoracic or abdominal cavity subsequently leading to torsion of the great vessels and cardiac arrest. Pericardial lacerations can bleed and result in pericardial effusions, and if large enough can result in cardiac herniation which often results in cardiac arrest.43,48,58 Hypokinesis can be seen in a segment of myocardium following BCI and is readily diagnosed on echocardiogram. Septal injuries are rare but can occur between atria or ventricles and are more frequently identified on autopsy than in patients who survive to the hospital. 47
While mechanical injuries can lead to a structural change to the heart, associated conduction changes can be more challenging to manage. Electrical disturbances can occur after BCI depending on the portion of the heart that was injured. For example, ST changes may occur with a specific coronary artery injury.52,59 The most common ECG abnormality after BCI is sinus tachycardia seen in 80% of cases, followed by atrial fibrillation. 60 However, atrial fibrillation can occur in critically ill patients for a variety of reasons and may not represent BCI. Ventricular dysrhythmias are less common but do occur with commotio cordis, a sudden cause of cardiac arrest/death in young patients when the heart undergoes blunt force during a very specific but vulnerable part of the electrical cycle (10-30 ms before the peak of the T wave). 61 Overall, arrhythmias occurring with BCI may be related to myocardial contusion or the stress of trauma resulting in catecholamine release. 48
Because the right heart is more anterior and therefore more prone to injury, right bundle branch blocks (BBB) are more common as a result of BCI compared to left BBB. 62 Additionally, if no prior ECGs are available for comparison, it is possible that an electrical abnormality represents underlying cardiac disease as opposed to acute injury. However, providers must consider any newly diagnosed ECG abnormality as potential sequelae of BCI.
Diagnosis
Workup for BCI is initially focused on identifying injuries that serve as markers for increased risk of BCI in hemodynamically stable patients. Whereas more significant BCI oftentimes is diagnostically apparent. Physical exam findings may or may not be present. Typically, exam findings of chest trauma such as ecchymoses, hematoma, or large abrasions raise suspicion for BCI but are nonspecific. Auscultation of a murmur could represent a BCI and necessitates further investigation (eg, ECG and echocardiogram). 43
ECG is often the first test in the evaluation of BCI as it is quick and easy to perform in the trauma bay. However, as previously mentioned, ECG changes are not specific for BCI and only offer adjunct information. The EAST guidelines recommend ECG for patients presenting with significant thoracic trauma, including the presence of sternal fractures, multiple rib fractures, hemopneumothorax, or other significant injuries in which BCI is suspected.63-65 The ECG alone has previously been demonstrated to be 97% sensitive for BCI; however, addition of a serum troponin can improve this to nearly 100%.60,66,67 All patients screening positive by abnormal ECG or serum troponin have traditionally been recommended to undergo telemetry monitoring for possible BCI, as previous studies found BCI may manifest up to 22 hours after presentation. 66 However, more recently Al-Khouja et al found that certain abnormal ECGs (eg, sinus tachycardia, nonspecific ST changes, and right bundle branch block) in the setting of isolated sternal fractures had a low association with BCI and these patients may not require prolonged monitoring. 68 This was followed with a multicenter study that had similar findings, suggesting that some patients do not require 24-hour telemetry monitoring and could undergo an abbreviated period of monitoring.68,69
Echocardiography is a useful tool in evaluating structural changes of the heart, including wall motion abnormalities, valve abnormalities, pericardial effusions, wall rupture, or chordae tendinae rupture. Current EAST guidelines recommend obtaining an echocardiogram only when there is prior hypotension or a significant arrhythmia (eg, atrial fibrillation, supraventricular tachycardia, or ventricular tachycardia). Thus, while it is very helpful to evaluate significant BCIs, it has little to offer in mild BCI and should not be performed in asymptomatic patients with elevated cardiac enzymes or nonspecific ECG changes.43,49
More advanced imaging such as cardiac computed tomography is available and can detect pericardial tears, effusions or other structural abnormalities. 70 However, some suggest that if using these advanced imaging techniques to differentiate BCI from myocardial infarction then a cardiologist and/or cardiac surgeon should be evaluating the patient. 43
Management
As with any trauma patient, immediate management involves basic principles of securing the airway, breathing and circulation. During the initial workup of a trauma patient, evidence of BCI may become readily apparent from cardiac monitoring, which can show dysrhythmias or tamponade (eg, hypotension with narrowed pulse pressure). Alternatively, a FAST examination may help evaluate for pericardial fluid. However, subsequent management must be dictated by one factor: whether the patient is hemodynamically stable or not. Cardiology consultation may be obtained for any patient with a new dysrhythmia, diagnosis of heart failure or hemodynamic instability due to cardiac dysfunction.
Hemodynamically Normal Patient
Dysrhythmia Management in Blunt Cardiac Injury.
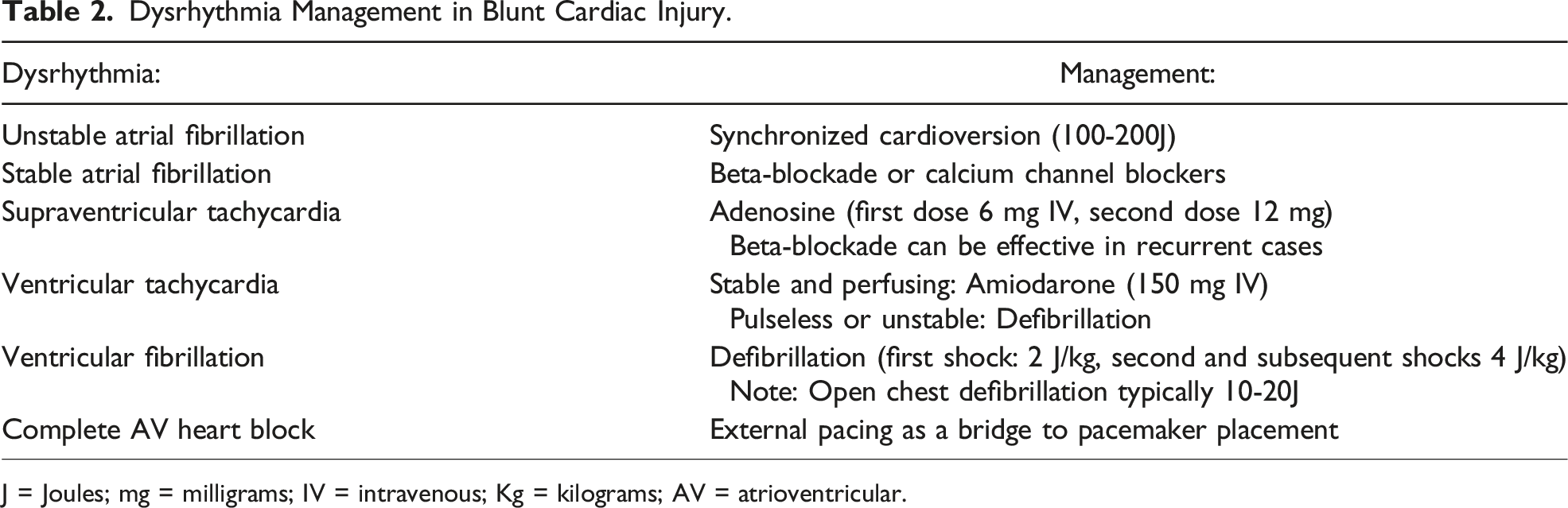
J = Joules; mg = milligrams; IV = intravenous; Kg = kilograms; AV = atrioventricular.
Management of Blunt Cardiac Injury Depending on Patient Hemodynamics.
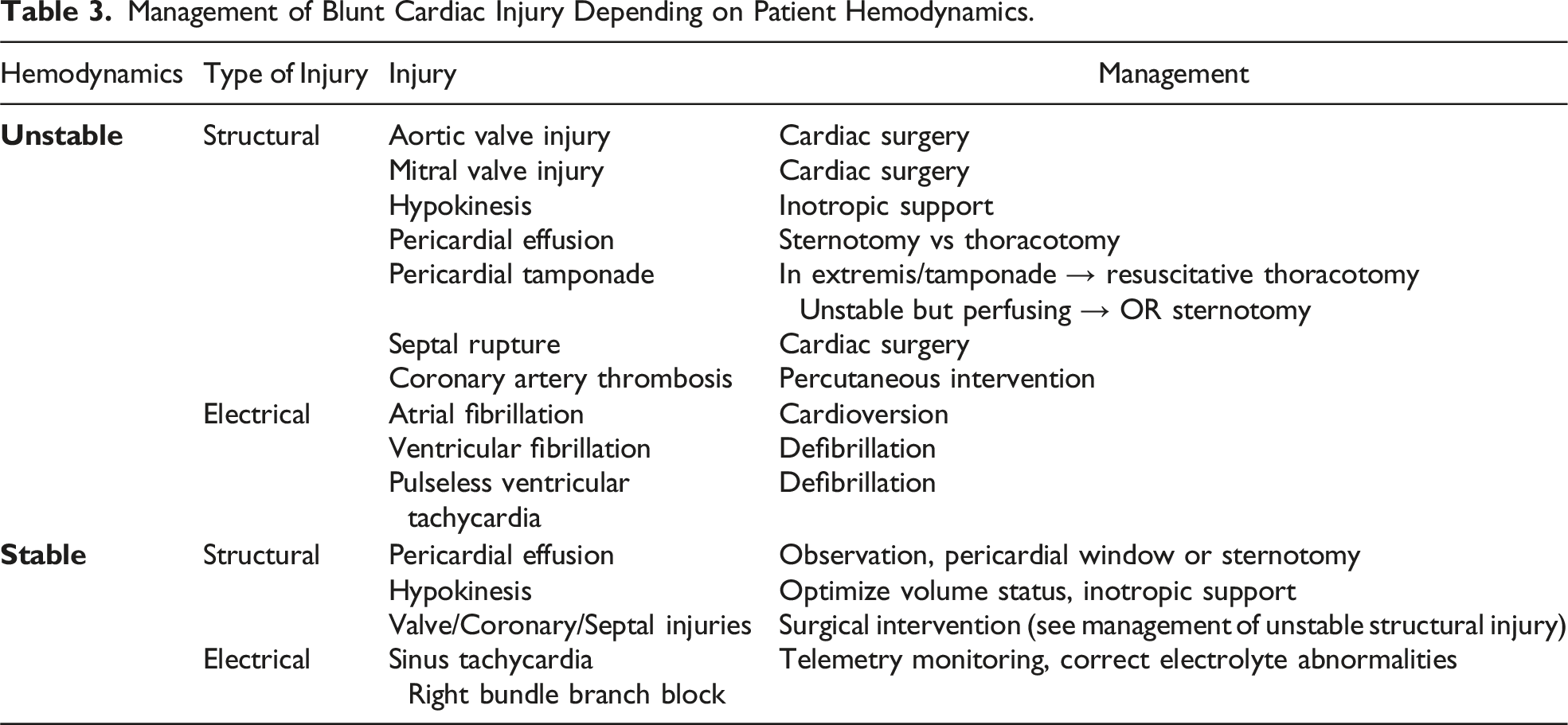
Management of pericardial effusion in an asymptomatic trauma patient without tamponade is somewhat controversial. Initial evaluation oftentimes includes a computed tomography angiography (CTA) scan of the chest which will help elucidate if the fluid is simple density or hemorrhage using Hounsefield units (HU). The HU for acute hemorrhage is typically 30-45; however, clotted blood can have a higher HU between 50-100.19-21 Smaller simple density effusions in a stable patient without other concerning features can likely be observed. Larger effusions or those with concerning features (eg, higher density) should be investigated and, if needed, intervened upon. 72 If it is suspected this effusion is from BCI and not a chronic effusion, a pericardial window may be the next step in management. If highly concerning or if a pericardial window is positive, then sternotomy should be performed.
Structural injuries such as valve, septum, or coronary injuries are not typically seen in hemodynamically normal patients; however, they can sometimes present with normal hemodynamics that quickly progress to cardiac failure. These patients require rapid surgical intervention with cardiac surgery and potentially CPB. 53
Hemodynamically Abnormal Patient
A patient in extremis with pericardial tamponade following thoracic trauma necessitates a resuscitative thoracotomy. This allows immediate decompression of the pericardium as well as control of hemorrhage. Extending the left anterolateral thoracotomy to a clamshell thoracotomy may facilitate improved exposure.43,53 Specific techniques of cardiac repair were previously discussed in the penetrating cardiac injury portion of this review. If a patient is showing hemodynamic signs of tamponade but not yet in extremis, immediate transport to the operating room for sternotomy is recommended. Endotracheal intubation should be delayed until the patient is prepped and draped as induction of anesthesia usually results in cardiac collapse. The patient should be prepped from the neck to the knees in the event that a vein harvest is required. In cases rapidly progressing to extremis, an exact diagnosis may not be known until the chest is open and the heart exposed.
Acute heart failure secondary to blunt trauma should be supported with inotropes and may require support devices such as an intra-aortic balloon pump, ventricular-assist device (eg, Impella), or extracorporeal membrane oxygenation (ECMO). 73 However, these devices should be used as a bridge to definitive repair or therapy. For example, acute heart failure due to a mitral valve injury can be supported with a device until definitive surgical repair can take place. 63
Outcomes depend largely on the severity of injuries. Joseph et al found hypotension and a serum lactate >2.5 mmol/L were the strongest predictors of mortality in patients diagnosed with BCI; however, this included all patients with the diagnosis—a wide spectrum of injury. 74
Conclusion
Traumatic cardiac injury remains a challenging entity in trauma patients due to the need for prompt diagnosis to limit morbidity and mortality. Penetrating cardiac trauma typically requires operative intervention for those who survive transport to the hospital. BCI represents a spectrum of injury with varying incidences in the literature likely due to broad and variable definitions as to what defines a BCI. Workup in both instances is predicated on the stability of the patient with stable patients undergoing imaging (ie, FAST exam +/− CT angiography) and unstable patients requiring swift operative intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.