
Abstract
• Pregnant trauma patients (PTPs) with (+)Utox were at a more advanced gestational age, had higher rates of uterine contractions, and were more frequently victims of domestic violence. • There were no differences in maternal complications between (+)Utox and (−)Utox PTPs. • (+)Utox PTPs had higher rates of head and extremity injuries. THC and methamphetamine were the most commonly detected substances.Key Takeaways
Introduction
Trauma is a leading cause of maternal and fetal morbidity and mortality, with pregnant women representing a uniquely vulnerable population. 1 The physiologic and anatomical changes experienced during pregnancy increase the complexity of trauma management and can lead to significant challenges in the provision of optimal care. 1 In addition, the presence of substance use may exacerbate existing risks and contribute to poor clinical outcomes in a generalized trauma population as well as select subset populations including pregnant trauma patients (PTPs). 2
Previous reports have demonstrated that illicit substance use, such as tetrahydrocannabinol (THC), the primary psychoactive component in marijuana, increases the likelihood of both sustaining and causing injuries, as well as being associated with higher rates of complications. 3 Additionally, the number of women using illicit substances during pregnancy has increased 4-fold in the past two decades and poses a dual threat, not only to the mother but also to the developing fetus, with potentially lifelong consequences. 4 Prenatal exposure to substances, such as alcohol, opioids, and stimulants, has been linked to various adverse effects including low birth weight, preterm delivery, newborn growth deficits, and stillbirth. 4
Despite the growing awareness of the interplay between substance use and trauma, few studies have focused on the rate of illicit substance use among PTPs. A deeper understanding of the clinical consequences in this patient population is essential for informing best practices in trauma management, optimizing maternal and fetal outcomes, and targeting public health interventions aimed at mitigating the risks associated with substance use during pregnancy. Therefore, this study aimed to evaluate injury patterns, mechanisms of trauma, and clinical outcomes of PTPs with positive urine toxicology ((+)Utox) admitted to trauma centers in Southern California. Given the diverse demographic makeup of the population in Southern California, it is particularly important to consider the role of race and ethnicity in the context of trauma and substance use during pregnancy. Hispanic females represent a significant portion of the population in this region, and understanding their unique experiences and challenges is important for developing targeted interventions and improving clinical outcomes. Research has shown that certain racial and ethnic groups, including Hispanics, face distinct barriers to healthcare access and are disproportionately affected by social determinants of health such as intimate partner violence (IPV) and substance abuse.5,6 We hypothesized that PTPs presenting with (+)Utox would have a higher rate of in-hospital complications compared to PTPs testing negative ((−)Utox).
Methods
This is a post hoc analysis of a multicenter retrospective study (2016-2021) from 12 Level-I and Level-II trauma centers in Southern California. Approval for this study was granted by the Institutional Review Board of all participating centers and a waiver of informed consent granted. PTPs ages 18 years and older were included. Prisoners and all patients with missing data regarding urine toxicology were excluded. Patients with positive opiates were also excluded since these patients may have received opioids pre-hospital or in-hospital for analgesia, prior to urine toxicology sampling. Data collected was stored in a centralized REDCap data collection tool. 7
PTPs were divided into two groups: those with (+)Utox and those with a (−)Utox for all drugs and negative serum alcohol. The primary outcome was an in-hospital complication including sepsis, stroke, myocardial infarction, pneumonia, acute kidney injury, acute renal failure, deep vein thrombosis, pulmonary embolism, urinary tract infection, fetal delivery, and mortality. Other variables collected included the injury profile such as the injury severity score (ISS) and injuries to the head, neck, chest, abdomen, pelvis, and extremities. We also collected demographics including maternal age, gestational age in weeks, mechanism of trauma, vitals on arrival, abdominal tenderness, premature rupture of membranes (PROM), fetal heart rate, and length of stay (LOS). Recorded laboratory studies included rhesus (Rh) factor, hemoglobin, white blood cell count, fibrinogen, serum alcohol level, and urine toxicology. When performed, imaging data tabulated included obstetric ultrasound, Extended Focused Assessment with Sonography in Trauma (E-FAST), chest radiograph, computed tomography (CT) imaging, and magnetic resonance imaging (MRI). Data on uterine contractions were collected using cardiotocography, a method that measures the frequency and intensity of uterine contractions alongside fetal heart rate. This technique involves the use of an external monitor placed on the abdomen of the pregnant patient, which detects the pressure changes associated with uterine contractions.
All categorical variables were coded as binary and analyzed with the Chi-square test. Continuous variables were analyzed with the Mann-Whitney U test. All P-values were two-sided, with a statistical significance level of <0.05. All analyses were performed with IBM SPSS Statistics for Windows (Version 28, IBM Corp., Armonk, NY).
Results
Demographics and Substance Use of PTPs With a (+)Utox vs a (−)Utox
Demographics and Injury Characteristics of Pregnant Trauma Patients Stratified by Utox.
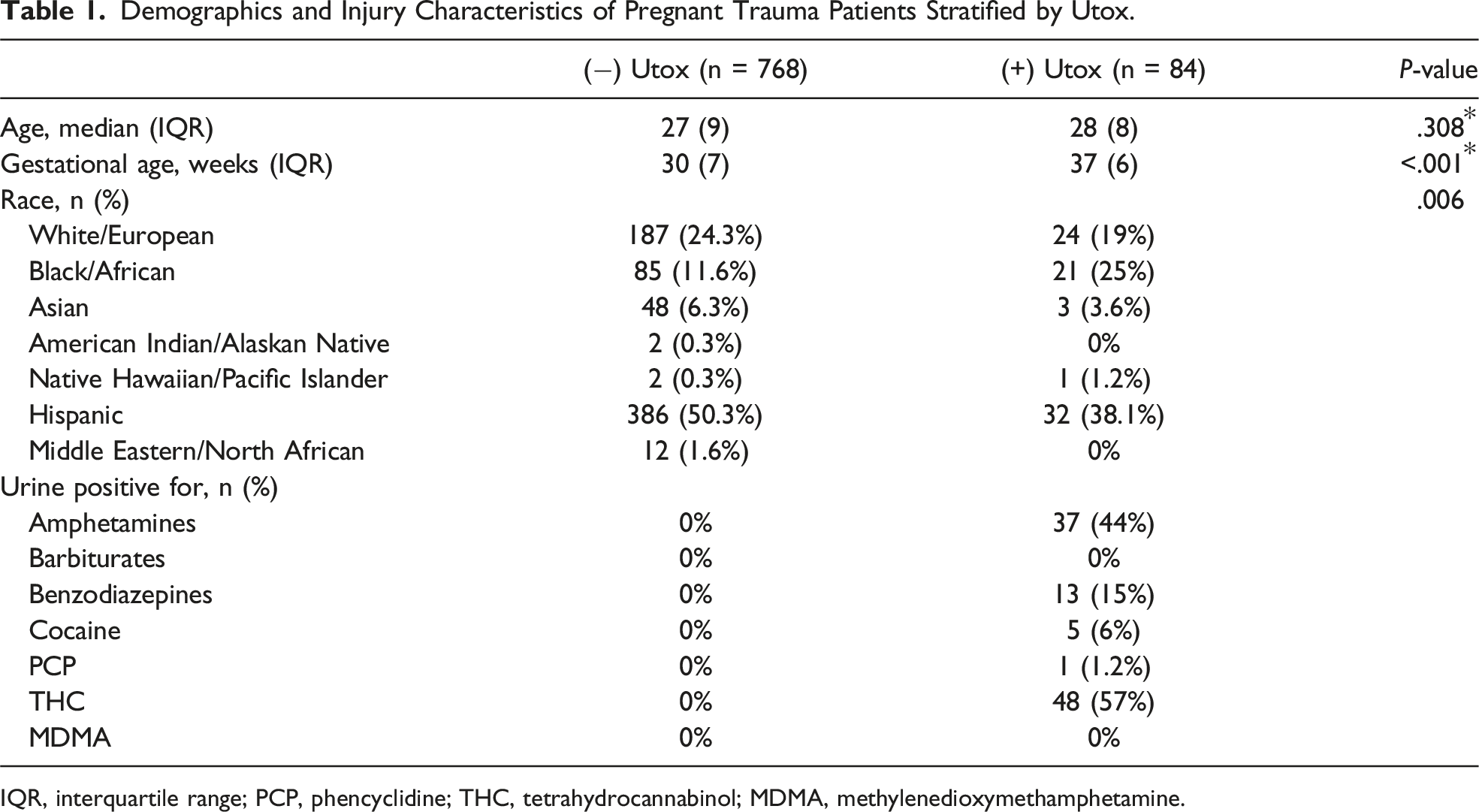
IQR, interquartile range; PCP, phencyclidine; THC, tetrahydrocannabinol; MDMA, methylenedioxymethamphetamine.
Mechanism of Injury for PTPs With a (+)Utox vs a (−)Utox
Mechanism of Injury for Pregnant Trauma Patients Stratified by Utox.
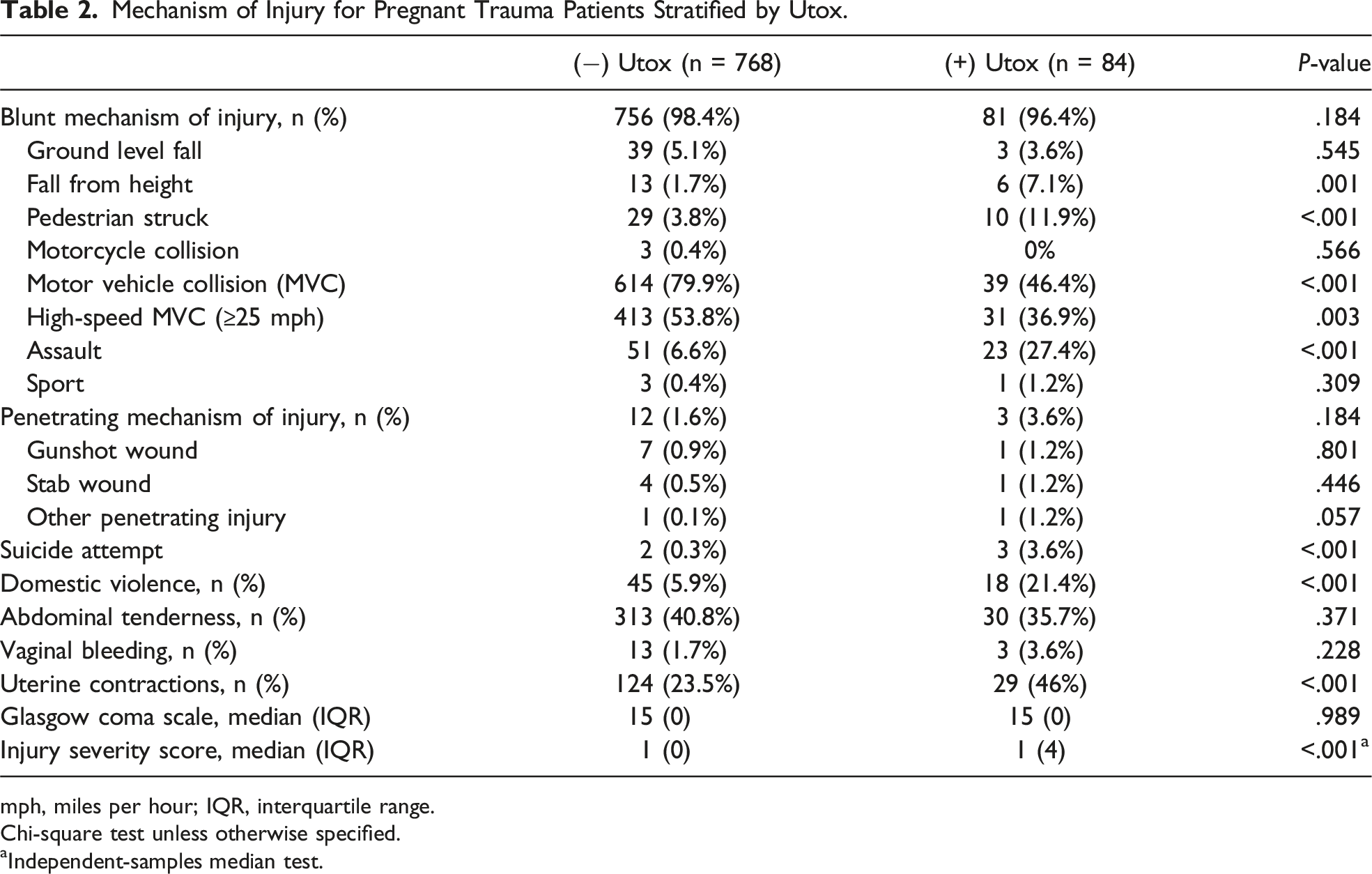
mph, miles per hour; IQR, interquartile range.
Chi-square test unless otherwise specified.
aIndependent-samples median test.
Injury Profile for PTPs With a (+)Utox vs a (−)Utox
Diagnostic Modalities, Identified Injuries, and Fetal Complications in Pregnant Trauma Patients Stratified by Fetal Delivery.
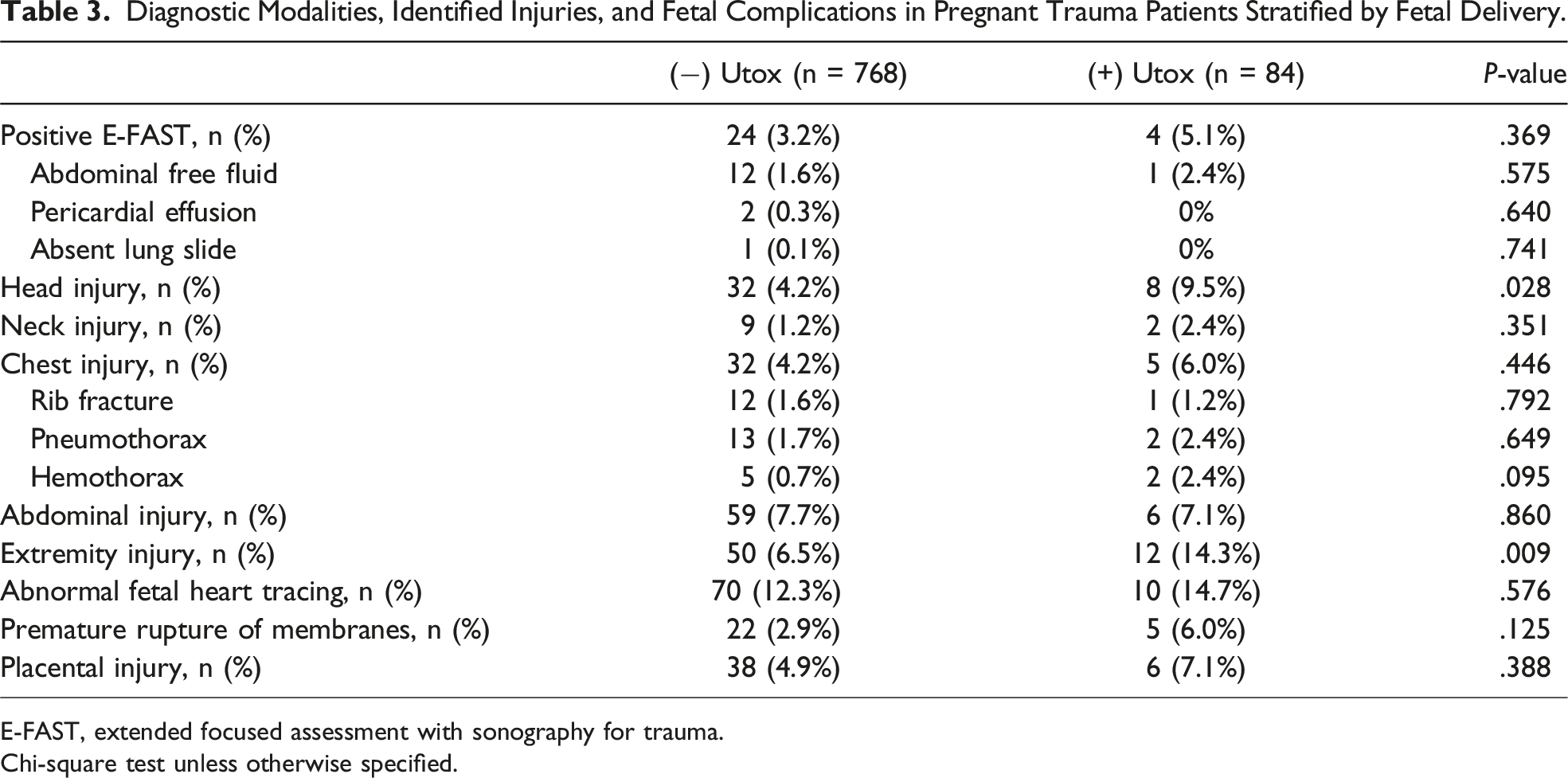
E-FAST, extended focused assessment with sonography for trauma.
Chi-square test unless otherwise specified.
In-Hospital Complications for PTPs With a (+)Utox vs a (−)Utox
Complications and Outcomes of Pregnant Trauma Patients Stratified by Fetal Delivery.
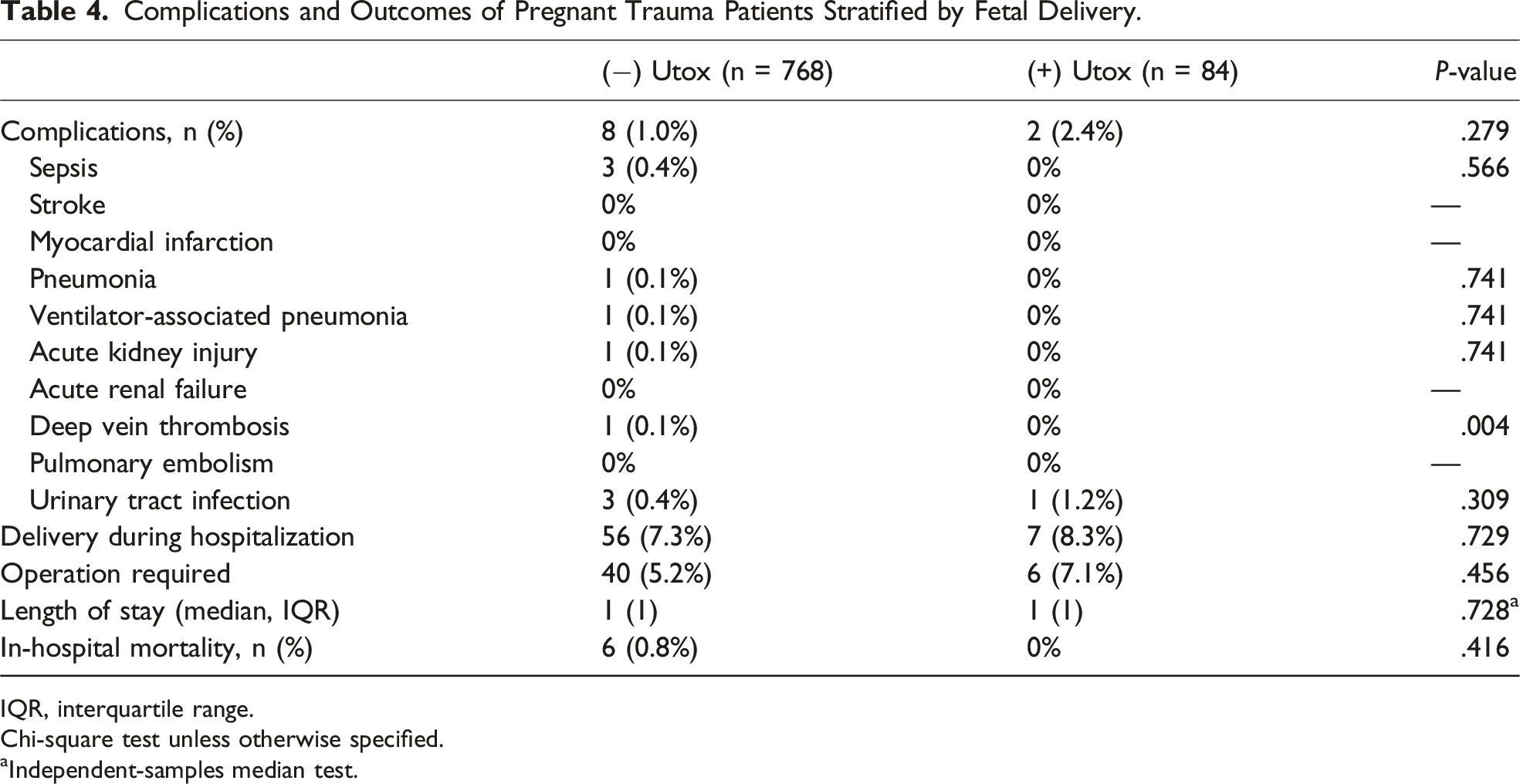
IQR, interquartile range.
Chi-square test unless otherwise specified.
aIndependent-samples median test.
Discussion
Our study sought to investigate the clinical outcomes of PTPs with positive urine toxicology screens. We found that PTPs with (+)Utox were at a more advanced gestational age, had a higher likelihood of experiencing uterine contractions, and were more frequently victims of domestic violence. There were no differences in complications between both groups. Additionally, patients with (+)Utox were more likely to sustain head and extremity injuries. The most commonly detected substances were THC and methamphetamine.
In our study, both (+) and (−)Utox PTPs demonstrated similar rates of in-hospital complications. This finding contrasts with some existing literature that has suggested an association between substance use and increased adverse outcomes in trauma patients. 8 One possible explanation for this observation in our study could be the relatively short LOS for both groups, with a median of only 1 day. This brief hospitalization period may not have been sufficient to capture the full range of complications that could arise in PTPs with substance use, as some complications may develop or become evident after discharge. Additionally, the short LOS could also indicate that the majority of the patients in both groups experienced less severe injuries, which may have contributed to the similar rates of in-hospital complications observed. It is important for future studies to consider longer follow-up periods and examine post-discharge outcomes. The national rate of THC usage has been reported to be just under 20%. 9 This has been consistently increasing with now more than 20 states having legalized recreational marijuana. 10 THC was the most prevalent substance detected in this study, which aligns with previous research highlighting the increasing use of cannabis during pregnancy. 11 Studies have reported that prenatal exposure to THC is associated with low birth weight, preterm delivery, and neurodevelopmental abnormalities. 11 However, further research is needed to establish the causal relationship between THC use and adverse outcomes in PTPs. Methamphetamine use was also common in our study population, which is concerning given the known risks to both the mother and fetus, such as placental abruption and fetal distress, as well as long-term consequences for the child, including cognitive and behavioral deficits. 12 This highlights the need for ongoing primary and secondary prevention efforts for pregnant women and PTPs, respectively.
The increased incidence of uterine contractions in the (+)Utox group may be associated with the physiological effects of substances such as methamphetamines, which were the second most commonly detected substance in this cohort. 13 Methamphetamines can stimulate uterine activity, potentially leading to premature labor, placental abruption, or uterine rupture.13,14 However, it is important to note that the presence of methamphetamines in the urine does not necessarily indicate recent use or intoxication due to the long-term detection window of the drug. Therefore, while there is an observed association between methamphetamine presence and uterine contractions, this study cannot definitively establish a causal relationship. The presence of frequent uterine contractions in the (+)Utox group also highlights the importance of close monitoring and timely intervention to prevent preterm birth and other complications. 15
The incidence of domestic violence in pregnant patients has been reported to range between 10%-20%, but it is likely significantly underreported. 16 Our study, which spans 5 years of data, found a higher incidence of domestic violence among PTPs with (+)Utox screens. This finding is consistent with existing literature, which has demonstrated that substance use is a known risk factor for experiencing domestic violence, likely because pregnant women with substance use disorders are more likely to have intimate partners who also use substances, and this co-occurrence increases the likelihood of IPV, particularly when methamphetamines are involved.8,12 This is alarming because methamphetamines were the second most common illicit substance found on urine toxicology in this study across Southern California. Health care providers should be cognizant of this association and have increased vigilance with screening PTPs with a (+)Utox for domestic violence. This may include resources for alternative housing assistance or safety plans as well as treatment of mental health disorders and substance abuse. Our study also found that PTPs with positive urine toxicology screens had higher rates of head and extremity injuries compared to those with negative screens. These injury patterns can be closely associated with domestic violence, which was significantly more prevalent in the (+)Utox group. Domestic violence is known to result in physical trauma, particularly to the head and extremities, and the increased prevalence of such injuries in the (+)Utox group likely reflects this association. 17 The link between substance use and domestic violence further complicates the clinical management of these patients. 18 Substance abuse can exacerbate the risk of violence and injury, creating a cycle of trauma and drug use. 18 As pregnancy advances, the use of illicit substances may increase due to a variety of factors, including stress, lack of social support, and ongoing domestic violence.18,19 This escalation in drug use can, in turn, lead to more severe trauma and higher rates of complications.18,19
Previous studies have shown that drug use can alter injury patterns in the general adult population. 2 Our study is among the first to specifically investigate the types of injuries sustained by PTPs with (+)Utox. The mechanisms behind this association are not fully understood, but they may be related to the effects of substances on cognitive and motor functions. However, we again cannot attribute any causal relationship to any particular substance given the retrospective nature of this study. Additionally, the circumstances leading to trauma, such as risky behaviors or impaired judgment while under the influence, could also contribute to the distinct injury patterns observed in this population.
Limitations of this study include its retrospective design, which hinders our ability to establish causality and may introduce potential biases in patient selection and data collection. Also, the study was conducted by trauma centers primarily in Southern California, which may limit the generalizability of the findings. Additionally, the urine toxicology screen may not accurately reflect the prevalence of substance use among the study population, as some substances may not be detected or have already been metabolized at the time of testing. Alternatively, substances such as THC may result positive within a urine toxicology for up to 4 weeks, thus may not reflect intoxication at the time of trauma or upon arrival. 20 We cannot definitively determine whether patients were impaired at the time of hospital admission. Urine toxicology screens detect drug metabolites that can remain in the system for an extended period, resulting in positive levels of this drug in the urine. We do not have data on the timeline between drug ingestion and hospital admission; therefore, it is unclear if the substances detected were directly contributing to the patient’s trauma or clinical presentation. Additionally, our study is a snapshot in time and lacks follow-up data on the outcomes of the pregnancies after discharge. We do not have information on long-term maternal or fetal outcomes, including major disabilities or fetal loss. The relatively short length of hospital stay for most patients means that many potential complications or adverse outcomes may not have been captured. Furthermore, while we observed associations between positive urine toxicology, domestic violence, and specific injury patterns, we do not have detailed data on the context or severity of the domestic violence experienced by these patients. Future studies should aim to clarify the underlying mechanisms and causal relationships, as well as explore potential strategies to improve outcomes for both the mother and fetus in this high-risk population.
Conclusion
Our study highlights the need for further research on the clinical outcomes of PTPs with positive urine toxicology screens, particularly in relation to THC and methamphetamine use. The higher rates of domestic violence and specific injury patterns identified in this population underscore the importance of comprehensive care and targeted interventions for these vulnerable patients.
Footnotes
Author Contributions
I Clark: data interpretation, manuscript writing/editing, critical revisions. J Nahmias: Protocol/project development, data interpretation, manuscript writing/editing, critical revisions. M Jebbia: Data interpretation, manuscript writing/editing, critical revisions. N Aryan: Data collection or management, data interpretation, critical revisions. A Lucas: Data collection or management, data interpretation, critical revisions. N Fierro: Data collection or management, data interpretation, critical revisions. N Dhillon: Data collection or management, data interpretation, critical revisions. E Ley: Data collection or management, data interpretation, critical revisions. J Smith: Data collection or management, data interpretation, critical revisions. S Burruss: Data collection or management, data interpretation, critical revisions. ADahan: Data collection or management, data interpretation, critical revisions. A Johnson: Data collection or management, data interpretation, critical revisions. W Ganske: Data collection or management, data interpretation, critical revisions. W Biffl: Data collection or management, data interpretation, critical revisions. D Bayat: Data collection or management, data interpretation, critical revisions. M Castelo: Data collection or management, data interpretation, critical revisions. D Wintz: Data collection or management, data interpretation, critical revisions. D Zheng: Data collection or management, data interpretation, critical revisions. A Tillou: Data collection or management, data interpretation, critical revisions. R Coimbra: Data collection or management, data interpretation, critical revisions. R Tuli: Data collection or management, data interpretation, critical revisions. J Santorelli: Data collection or management, data interpretation, critical revisions. B Emigh: Data collection or management, data interpretation, critical revisions. M Schellenberg: Data collection or management, data interpretation, critical revisions. K Inaba: Data collection or management, data interpretation, critical revisions. T Duncan: Data collection or management, data interpretation, critical revisions. G Diaz: Data collection or management, data interpretation, critical revisions. E Tay-Lasso: Data collection or management, data interpretation, critical revisions. D Zezoff: Data collection or management, data interpretation, critical revisions. A Grigorian: Protocol/project development, data interpretation, manuscript writing/editing, critical revisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.