
Abstract
Background
Current guidelines recommend 24-hour telemetry monitoring for isolated sternal fractures (ISFs) with electrocardiogram (ECG) abnormalities or troponin elevation. However, a single-center study suggested ISF patients with minor ECG abnormalities (sinus tachycardia/bradycardia, nonspecific arrhythmia/ST-changes, and bundle branch block) may not require 24-hour telemetry monitoring. This study sought to corroborate this, hypothesizing ISF patients would not develop blunt cardiac injury (BCI).
Materials & Methods
A retrospective study was performed at 8 trauma centers (1/2018-8/2020). Patients with ISF (abbreviated injury scale <2 for the head/neck/face/abdomen/extremities) and minor ECG abnormalities or troponin elevations were included. Patients with multiple rib fractures or hemothorax/pneumothorax were excluded. The primary outcome was an echocardiogram confirmed BCI. The secondary outcome was significant BCI defined as cardiogenic shock, dysrhythmia requiring treatment, post-traumatic cardiac structural defects, unexplained hypotension, or cardiac-related procedures. Descriptive statistics were performed.
Results
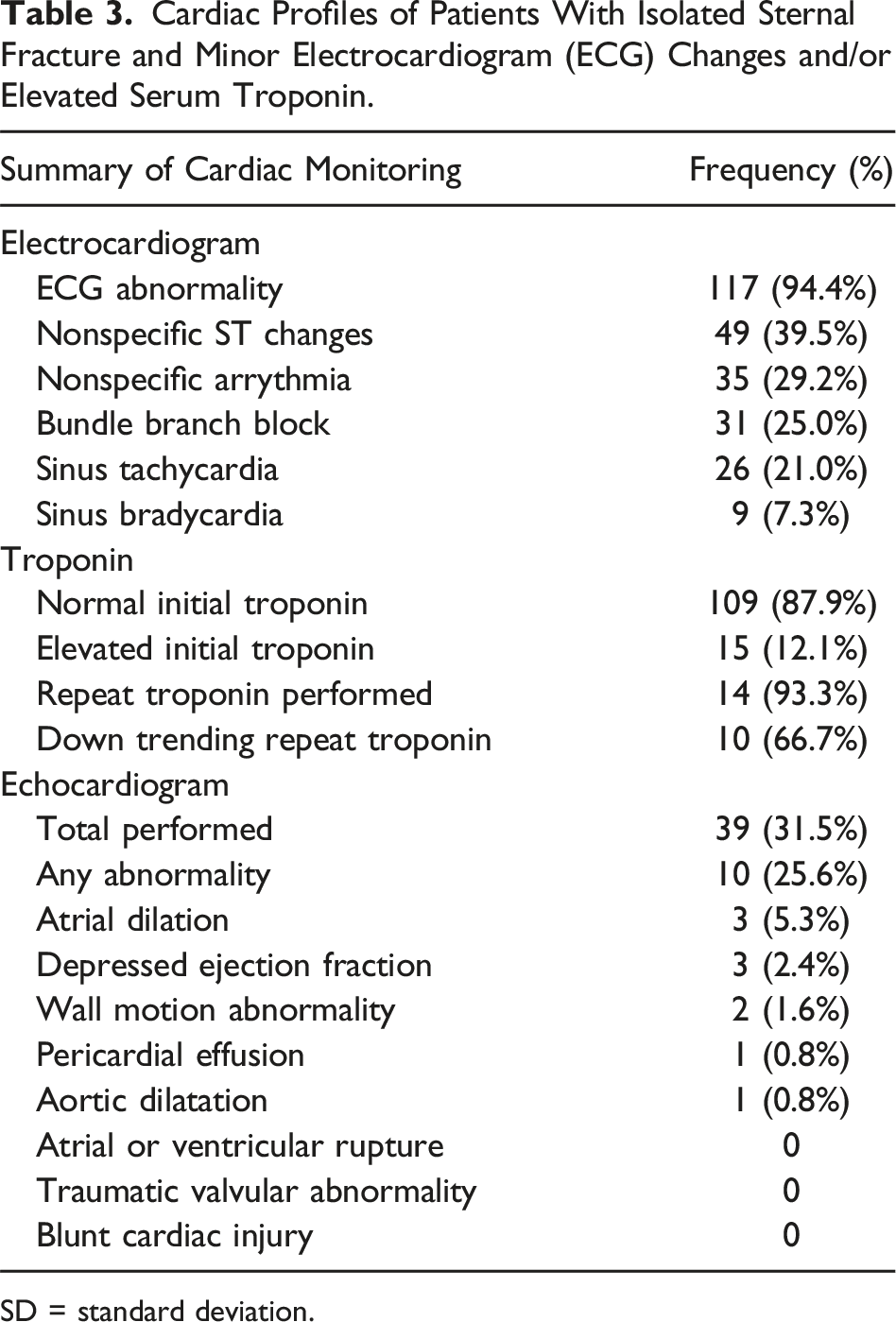
Of 124 ISF patients with minor ECG abnormalities or troponin elevation, 90% were admitted with a mean stay of 35 hours. Echocardiogram was performed for 31.5% of patients, 10 (25.6%) of which had abnormalities. However, no patient had BCI diagnosed on echocardiography. In total, 2 patients (1.6%) had a significant BCI (atrial fibrillation and supraventricular tachycardia at 10 and 82 hours after injury). No patient died.
Conclusions
Following ISF with minor ECG changes or troponin elevation, <2% suffered significant BCI, and none had an echocardiogram diagnosed BCI, despite >30% receiving echocardiogram. These findings challenge the dogma of mandatory observation periods following ISF with associated ECG abnormalities and support the lack of utility for routine echocardiography in these patients.
Key Takeaways
• Patients with isolated sternal fracture and ECG changes or troponin elevation may not need 24-hour telemetry monitoring. • Abbreviated monitoring may be appropriate for isolated sternal fractures in the setting of ECG changes and troponin elevation.
Introduction
Sternal fracture (SF) is a common injury that has varying degrees of severity and outcomes. Motor vehicle collisions (MVCs) account for nearly 90% of all SFs.1-4 Overall, 3%-6% of MVCs result in sternal fracture, and BCI is reported in 2%-42% of patients with SFs.2,3 However, other causes of blunt trauma, such as ground-level falls, falls from height, assault, or motorcycle collisions, can also result in SF.5-7 A crucial distinction must be made between isolated sternal fracture (ISF) and polytrauma sternal fracture. Sternal fractures often occur with other injuries, including rib fracture (46%), vertebral fracture (38%), retrosternal hematoma (28%), and/or hemothorax/pneumothorax. 3 While polytrauma sternal fractures may have mortality rates as high as 45%, ISFs are usually managed conservatively, and monitoring may not be required for ISFs alone.1,5-8
In 2012, the Eastern Association for the Surgery of Trauma (EAST) guidelines recommended screening for all ISF patients for blunt cardiac injury (BCI) using electrocardiogram (ECG) and troponin. 9 It was then advised to undergo 24-hour telemetry monitoring to rule out BCI if either test is positive; however, if both tests are negative, BCI is considered ruled out. 9 Additionally, an echocardiogram should only be performed if the patient has a new, sustained arrhythmia, hemodynamic instability, or syncope. However, these guidelines do not differentiate between minor ECG abnormalities and more severe ECG changes that necessitate admission (ie, ST segment elevations or discrete new onset arrhythmias such as ventricular or supraventricular tachycardia or atrial fibrillation/flutter). Consequently, all patients with ECG changes have historically been admitted for 24-hour telemetry monitoring.
Recently, a single-center study proposed that ISF patients could be safely managed with abbreviated monitoring and without hospital admission, as none of the patients experienced BCI or required ISF-related procedures, and <1% had significant cardiac complications. 1 Building upon these findings, the current study sought to corroborate these results in a multicenter setting and reassess the necessity for prolonged telemetry monitoring in patients presenting with ISF and minor ECG abnormalities. We hypothesize that ISF patients with minor ECG changes upon arrival will not exhibit structural or functional abnormalities on echocardiography (echocardiogram diagnosed BCI) or demonstrate clinical symptoms of significant BCI. If the data support our hypothesis, it suggests that a subset of ISF patients with minor ECG changes could potentially avoid unnecessary hospital admissions, thus conserving valuable resources and reducing health care expenditures.
Materials and Methods
The institutional review board approved the study period for patient data collection at each participating center, and a waiver of informed consent was granted for data collection. This retrospective (1/1/2018-8/30/2020) multicenter study involving 8 Level-I and Level-II trauma centers included adult patients ≥18 years with radiographically confirmed SF on computed tomography scan and presenting ECGs displaying minor abnormalities or those with no ECG abnormalities but elevated serum troponin. Each institution in this study routinely obtains ECG and a serum troponin level for all patients with suspected BCI. During data collection, there was a transition from collecting troponin I to high sensitivity troponin at one of the participating centers thus both were included in the study. Troponin elevation was determined based on normal reference ranges provided by the laboratory for the type of troponin collected. Minor ECG changes were defined as sinus tachycardia, asymptomatic sinus bradycardia, nonspecific arrhythmia/ST-changes, or bundle branch block for the purpose of this study. ISF was defined as having an abbreviated injury scale (AIS) score <2 for the head/neck/face/extremities/abdomen. Pregnant and incarcerated patients were excluded from the study. Patients with multiple rib fractures or hemothorax/pneumothorax were also excluded, as these patients would otherwise likely require admission. It should also be noted that blunt chest trauma patients without sternal fracture may also be at risk of BCI. However, because there is no clear definition for screening of patients with blunt chest trauma without sternal fracture, these patients were not included in the study.
Data Collection
Data was collected using REDCap, a secure online software.10,11 Patient demographics (including age, sex, ethnicity, comorbidities, and anticoagulation status) and cardiac information were collected, including initial ECG on arrival, serum troponin, echocardiogram, ISF-related complications, and ISF-related procedure data. The primary endpoint of this study was the presence of an echocardiogram confirmed BCI, defined as segmental wall motion abnormalities leading to hypotension or valvular dysfunction, as determined by the cardiologist’s interpretation of the echocardiogram. The secondary outcome was the presence of significant BCI, defined as cardiogenic shock, dysrhythmia requiring treatment, post-traumatic cardiac structural defects, unexplained hypotension requiring treatment, or cardiac-related procedures as defined by Velmahos et al 12 Abnormalities on ECG were diagnosed using machine reading interpretations as well as attending surgeon/emergency physician interpretations. Complications related to ISF were defined as hypotension (systolic blood pressure <90 mmHg), significant arrhythmia or SF/cardiac-related procedures such as sternal stabilization (eg, sternal plating or wiring), cardiac catheterization, chest tube insertion, unplanned intubation, sternotomy, or thoracotomy. Furthermore, data regarding non-cardiac complications were recorded, including urinary tract infection, acute kidney injury, acute respiratory distress syndrome, sepsis, and pneumonia.
Additional data collected included demographic data such as age, sex, race/ethnicity, and pertinent past medical history such as pre-existing arrhythmia (ie, atrial fibrillation and atrial flutter), coronary artery disease, congestive heart failure, hypertension, valvular disease, diabetes mellitus, chronic obstructive pulmonary disease, cirrhosis, end-stage renal disease, or chronic kidney disease. Injury profile data was also obtained, including mechanism of injury (MVC, auto vs pedestrian, motorcycle collision, fall, and assault), AIS grades (for the face, head/neck, chest, abdomen, and extremity), and injury severity score (ISS). Hospitalization data were also obtained, including length of stay (LOS), intensive care unit (ICU) admission, discharge location, and mortality.
Statistical Analysis
All statistical analyses were performed using International Business Machines (IBM) SPSS statistics for Windows (version 28, IBM Corp. Armonk, NY). 13 Descriptive statistics including student t-test and chi-square analysis were utilized when necessary to appropriately characterize the patient population and statistical indices included mean, median, and standard deviation.
Results
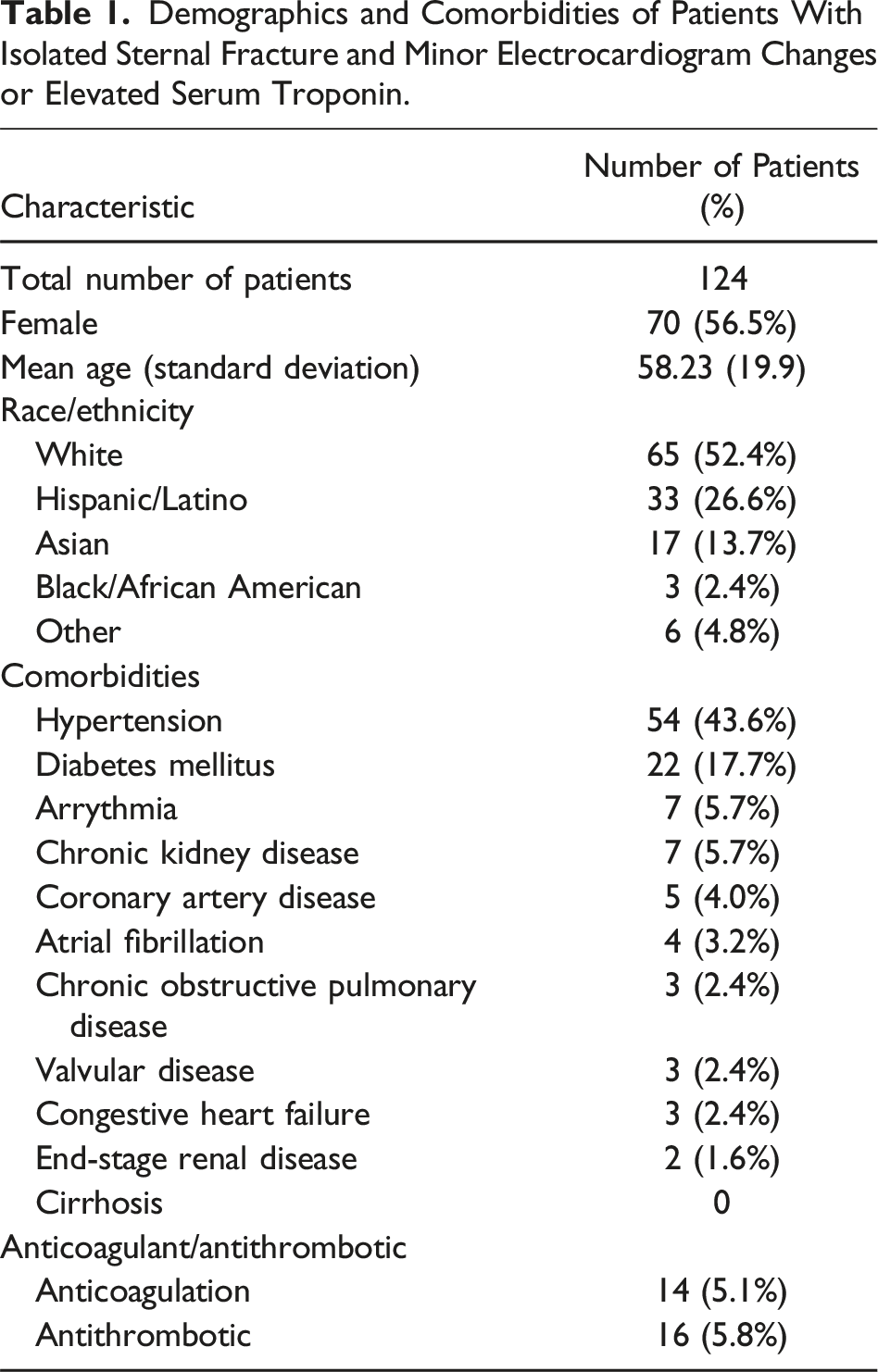
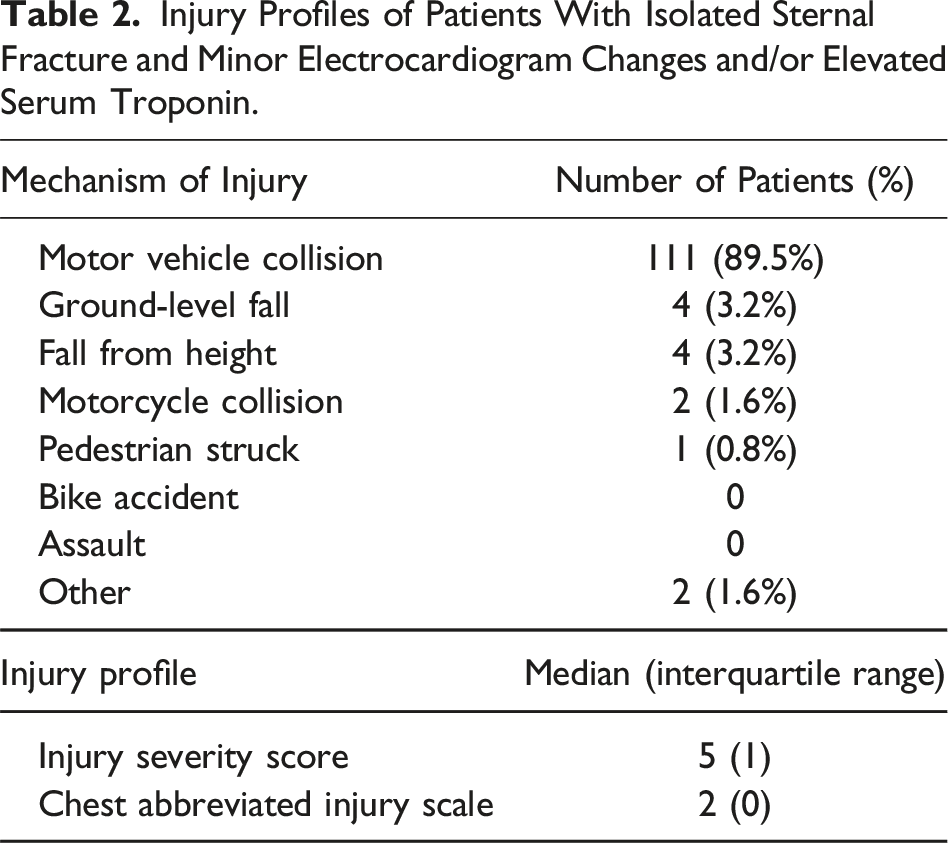
A total of 274 patients (54% female) with a mean age (SD) of 54 (20) years experienced an ISF without significant arrhythmia. Of the 274 patients, 124 (45.3%) met inclusion/exclusion criteria (Figure 1) with either minor ECG changes or elevated serum troponin and thus were included for analysis (Table 1). The most common mechanism of injury was a MVC, accounting for 89.5% of cases. The median ISS for the overall cohort was 5, and the median AIS for the chest was 2 (Table 2). Isolated sternal fracture patients flow chart. A flow diagram for inclusion/exclusion of patients with isolated sternal fracture (ISF) with electrocardiogram (ECG) abnormalities and/or serum troponin elevation, evaluating for significant blunt cardiac injury (BCI) or echocardiogram confirmed BCI. Demographics and Comorbidities of Patients With Isolated Sternal Fracture and Minor Electrocardiogram Changes or Elevated Serum Troponin. Injury Profiles of Patients With Isolated Sternal Fracture and Minor Electrocardiogram Changes and/or Elevated Serum Troponin.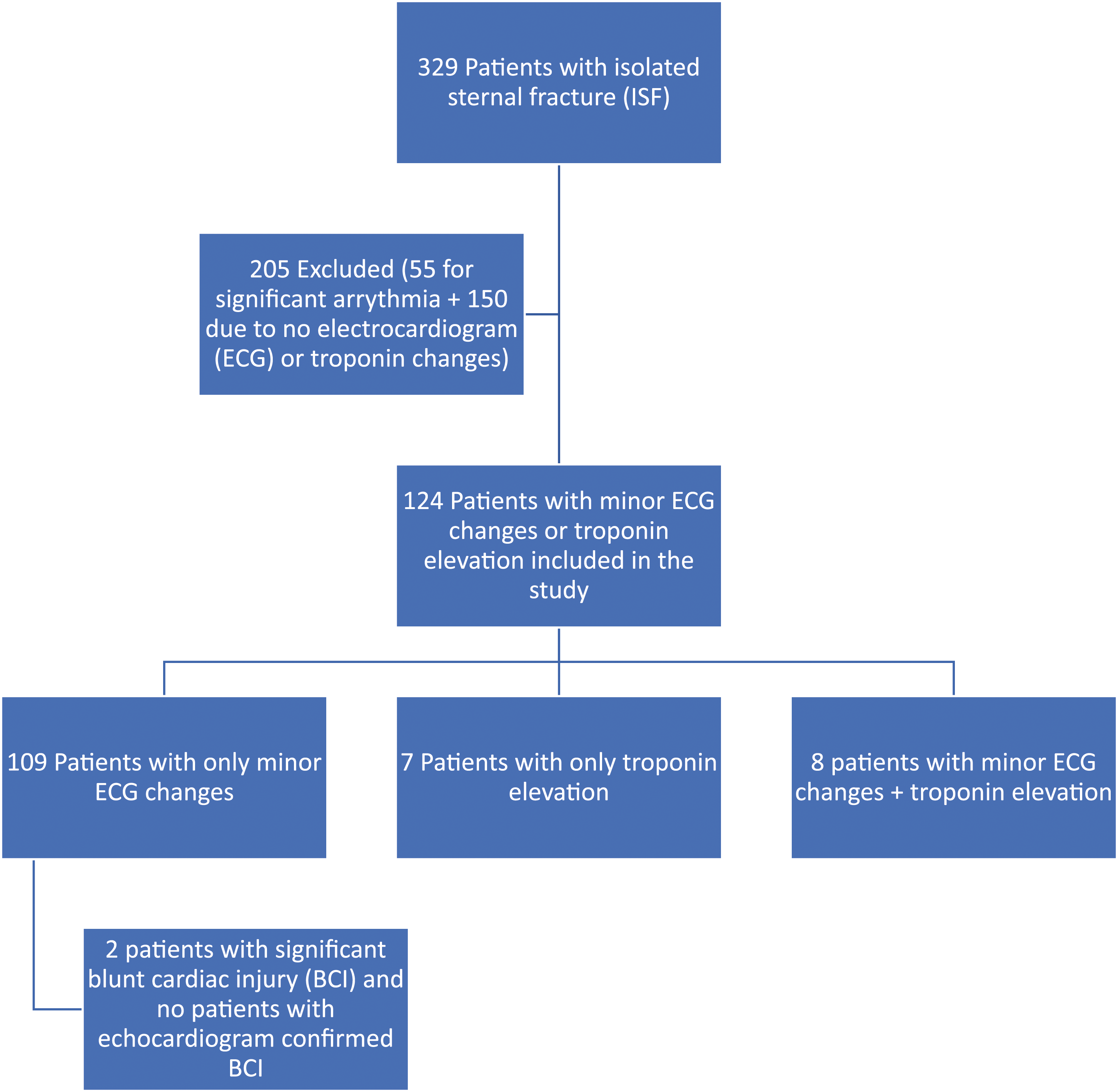
Cardiac Profiles of Patients With Isolated Sternal Fracture and Minor Electrocardiogram (ECG) Changes and/or Elevated Serum Troponin.
SD = standard deviation.
Echocardiogram Confirmed BCI and Significant BCI in ISF Patients with Minor ECG Abnormality and/or Elevated Serum Troponin
Complications and Procedures for Patients With Isolated Sternal Fracture and Minor Electrocardiogram Changes and/or Elevated Serum Troponin.
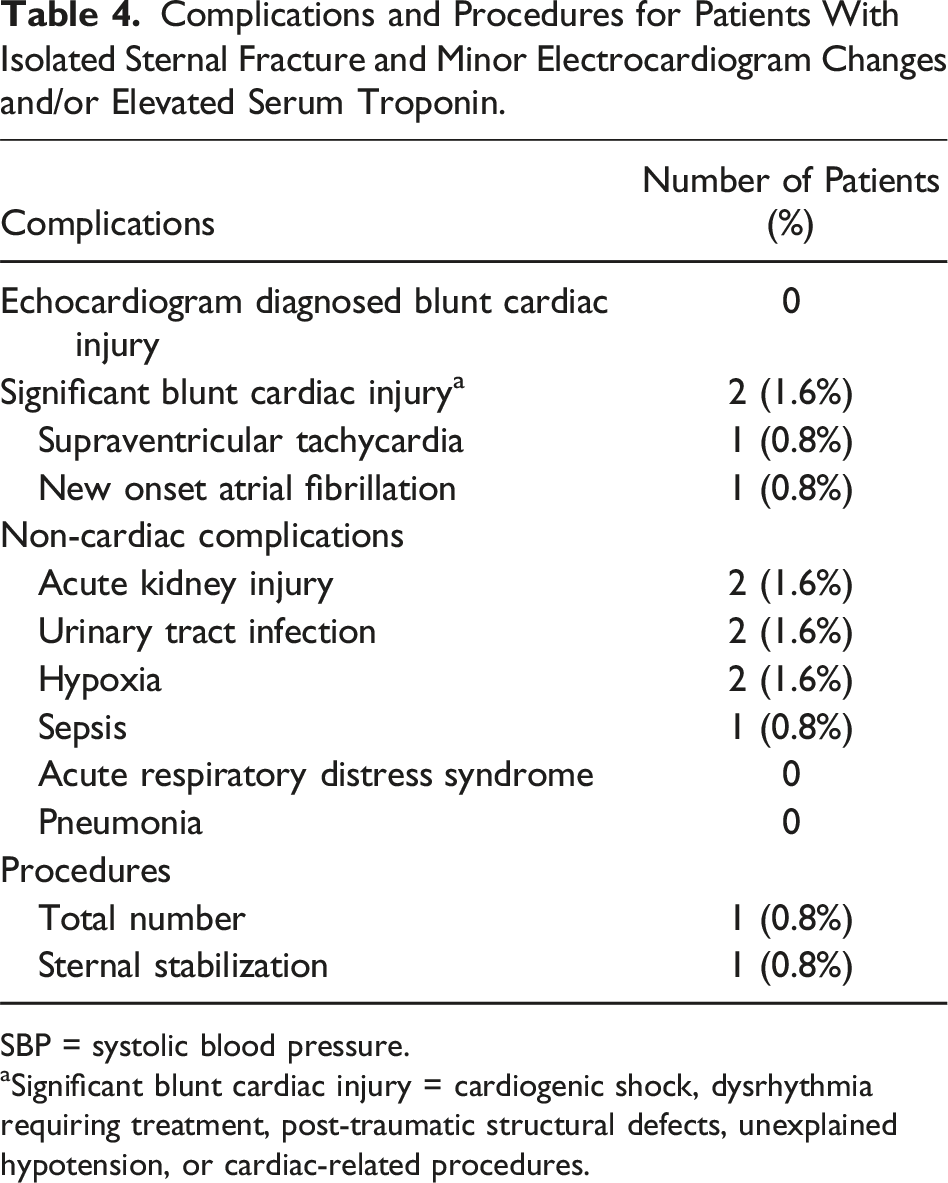
SBP = systolic blood pressure.
aSignificant blunt cardiac injury = cardiogenic shock, dysrhythmia requiring treatment, post-traumatic structural defects, unexplained hypotension, or cardiac-related procedures.
Non-cardiac Outcomes for ISF Patients
Hospital Course and Discharge Disposition for Patients With Isolated Sternal Fracture and Minor Electrocardiogram Changes and/or Troponin Elevation.
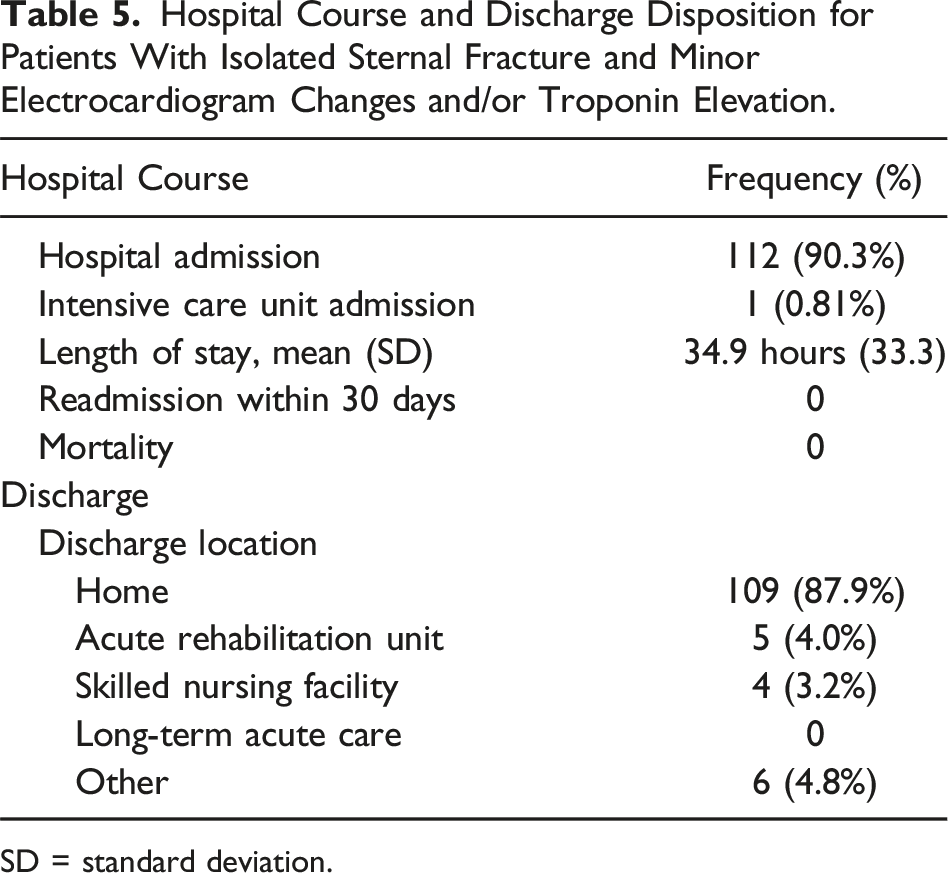
SD = standard deviation.
Discussion
Blunt cardiac injury is a potentially life-threatening complication following SF. Our study corroborates that BCI following ISF is extremely rare, as <2% of ISF patients with minor ECG abnormalities or elevated serum troponin experienced significant BCI. Moreover, no ISF patients had echocardiogram confirmed BCI, and no patients underwent a BCI-related procedure. However, more than 30% of all patients underwent an echocardiogram. Given the BCI rate of 1.6% in this cohort, the number needed to treat for ISF patients would be 62.1.
Previous studies have found that ISF alone is not a predictor of BCI.14-17 Weiner et al reviewed 50 patients with ISF and found only 6% had clinically significant cardiac contusion. 15 Furthermore, Sabada et al found only 1 of 37 (2.7%) ISF patients over a 2-year period sustained a BCI. 16 Our current study builds upon these results, showing that significant BCI rarely occurred in patients with ISF and minor ECG abnormalities. Previously, Athanassiadi et al 14 did not recommend an echocardiogram for screening, whereas Wiener et al 15 advised echocardiogram usage only for ISF patients with moderate ISS.6-15 Despite these recommendations, nearly one-third of patients in our study received an echocardiogram, highlighting the need to reinforce existing guidelines and limit the use of echocardiogram to those with potential cardiogenic syncope, new arrhythmia, or unexplained hypotension as no patients in this study suffered echocardiogram diagnosed BCI. Efforts to limit the unnecessary use of echocardiography may help reduce health care expenditures and decrease patient out-of-pocket costs.
Admission in the setting of ISF with significant arrhythmia or hypotension is certainly indicated. However, this study showed that 90% of patients with minor ECG changes or troponin elevation were admitted following ISF, while the other 10% were observed in the Emergency Department. In all patients, including those not admitted, the average LOS was nearly 35 hours. Nevertheless, nearly all patients were discharged home, and none died. The patient with a brief episode of supraventricular tachycardia was admitted to a telemetry-monitored bed and upgraded to ICU level of care due to the SVT but was discharged shortly after without intervention or further complication. It should be noted that this patient had a toxicology screen positive for tetrahydrocannabinol, opioids, and methamphetamines upon arrival, which may be potential confounders. These findings suggest that observing all ISF patients, with 24-hour telemetry monitoring, may be unnecessary and by modifying previous guidelines, there is the potential for significant cost savings. Using a single telemetry-monitored bed is conservatively estimated to cost $1400 per night.18,19 Given the relatively high incidence of ISF, this would save hundreds of thousands, if not millions, of dollars annually and free up available inpatient beds.
Limitations
This study has inherent limitations to the retrospective design, including misclassification and missing data. To corroborate the findings of the current study, a prospective, multicenter study analyzing appropriate observation periods for patients with ISF and ECG changes or troponin elevation appears warranted. It should be noted, we had intended to perform a multivariable logistic regression analysis to determine if any variables were predictors of BCI. However, this analysis could not be performed due to the limited number of patients suffering an echocardiogram confirmed BCI or significant BCI.
Additionally, this study does not include blunt chest trauma patients without sternal fracture, which potentially misses a population of patients experiencing BCI. Furthermore, this study lacks some pertinent variables, including detailed cardiac history and prior cardiac interventions (percutaneous coronary intervention or cardiac surgery). The type of sternal fracture and the presence of a retrosternal hematoma were also not studied; therefore, no relation could be made based on sternal fracture location and likelihood of cardiac complication. Moreover, we could not determine the exact appropriate period, if any, that these patients should be monitored in the Emergency Department. Finally, the authors do not believe ISF patients with new onset arrhythmia or significant ECG changes should be considered for abbreviated monitoring, as these patients were excluded from this study.
Following ISF with minor ECG changes or an elevated serum troponin without ECG changes, no patients sustained an echocardiogram diagnosed BCI, and less than 2% of patients experienced significant BCI. However, over 30% of patients underwent an echocardiogram, and over 90% were admitted for telemetry monitoring. These results suggest 24-hour telemetry monitoring in ISF patients with minor ECG changes may be unnecessary. Additionally, this study identifies the potential opportunity for improved adherence to existing guidelines regarding ordering an echocardiogram in this ISF population. Further investigations should be performed to identify an optimal monitoring timeframe for ISF patients with minor ECG changes to avoid unnecessary admissions and curtail health care expenditures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.