
Abstract
Abdominal pain continues to be a common chief complaint in the emergency setting. While this presentation can be non-specific, there are certain findings that warrant immediate surgical intervention. Portal venous gas on imaging in the setting of peritonitis and sepsis is one such finding. Thyrotoxicosis on the other hand is an uncommon diagnosis that is associated with non-specific symptoms resulting in delayed diagnosis, a clinical scenario that can lead to significant morbidity and mortality. Here, we present a rare case of a patient who presented with signs and symptoms of peritonitis and portal venous gas on CT scan that was taken emergently to the operating room. No intraabdominal pathology was identified. The patient was later diagnosed with thyrotoxicosis, the presumed cause of the acute abdomen presentation.
Hyperthyroidism normally presents with tachycardia, heat intolerance, hypertension, hyperphagia, unintentional weight loss, and in some cases exophthalmos. 1 Commonly, patients with undiagnosed worsening hyperthyroidism present with arrhythmias, heart failure, and in rare cases, thyrotoxicosis. 1 Thyrotoxicosis has an estimated incidence of .2 cases per 100,000 population, 2 and it is rarely diagnosed in the emergent setting. 3 Mortality can be as high as 25 percent; therefore, timely diagnosis is crucial to improving patient outcomes. 3 Severe abdominal pain is rarely reported in the literature as a chief complaint for patients with hyperthyroidism. A few cases of thyrotoxicosis have been reported with patients presenting with ketoacidosis, acute abdomen, and multi-organ failure 3 ; however, thyrotoxicosis is not well described in the setting of portal venous air. We present the management of thyrotoxicosis masquerading as an acute abdomen.
Our patient is a 32-year-old man with a past medical history of hyperthyroidism who presented to the emergency department (ED) with a 2-day history of severe abdominal pain, nausea, bilious emesis, and non-bloody watery diarrhea. On initial assessment, he was hypotensive and tachycardic. Initial lab workup revealed a leukocytosis of 11.5 K/mcL, a lactic acidosis of 7.7 mmol/L, and acute kidney injury (AKI) with a creatinine of 2 mg/dL. He was fluid resuscitated and started on norepinephrine to maintain a mean arterial pressure greater than 65 mmHg. An abdomen and pelvis computed tomography (CT) with intravenous contrast revealed hepatic portal venous gas (HPVG), pneumatosis involving the ascending colon with circumferential wall thickening at the hepatic flexure extending to the mid transverse colon (Figures 1 and 2). Given the concern for peritonitis and ischemic bowel, the decision was made to take the patient to the operating room (OR) for an emergent exploratory laparotomy. Intraoperatively, all areas of the abdomen were normal appearing without any evidence of ischemia or injury. In the recovery unit, the patient remained hypotensive and tachycardic despite fluid resuscitation and stress dose steroids. He was transferred to the surgical intensive care unit for further management. Sagittal view of CT abdomen/pelvis with IV contrast demonstrating hepatic portal venous gas. Transverse view of CT abdomen/pelvis with IV contrast showing circumferential thickening of the large bowel at the hepatic flexure.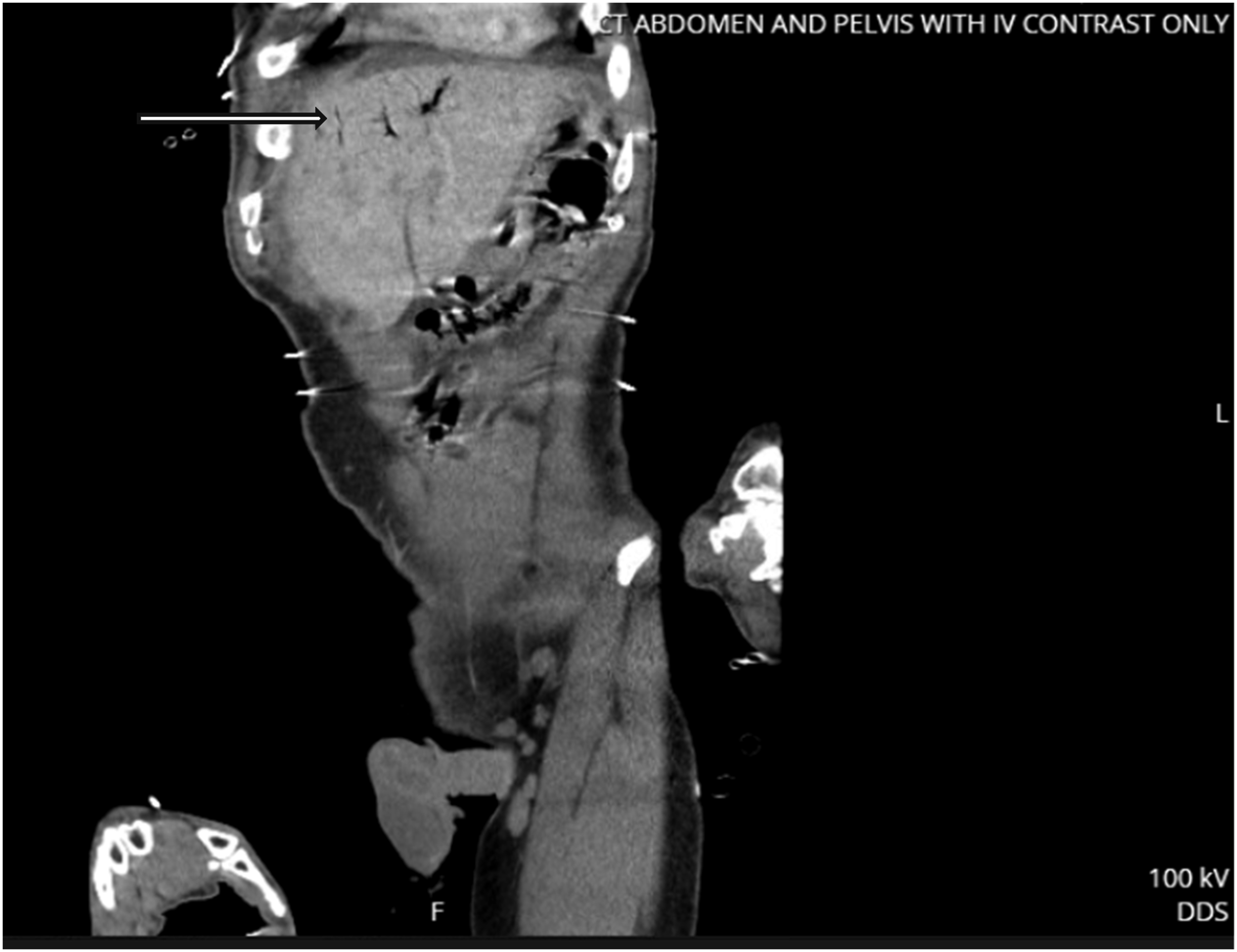

A thyroid panel revealed a TSH of <.01 uIU/mL, triiodothyronine of 282.8 ng/dL, and a free thyroxine of 5.77 ng/dL, confirming a diagnosis of thyrotoxicosis. He was started on propylthiouracil, and his vital signs improved, and his AKI resolved by postoperative day (POD) 1. He continued to improve and was discharged home on POD 5 on methimazole and propranolol. He was seen 4 months postoperatively by the acute care surgery/trauma clinic and was free of complications from a surgical standpoint.
While abdominal pain is a common chief complaint in the ED, abdominal pain associated with hyperthyroidism is not a common finding. Here, we present a patient with thyrotoxicosis who presented to the ED with complaints of severe abdominal pain with associated nausea, bilious emesis, and non-bloody diarrhea, with portal venous gas and evidence of bowel ischemia on imaging, a leukocytosis, and lactic acidosis. Our patient was taken emergently to the OR; however, no acute intraabdominal pathology was identified. The patient was later diagnosed with thyrotoxicosis and appropriate treatment was initiated. This case report aims to bring awareness that while the treatment algorithm for an acute abdomen will remain appropriate in patients with signs and symptoms of life-threatening intraabdominal pathology, thyrotoxicosis should remain on the differential if no contributing pathology is found intraoperatively.
In 2021, Al-Mashdali et al 1 reported a case of a patient who presented with a 3-week history of severe abdominal pain with associated nausea and vomiting. This patient was subsequently diagnosed with non-diabetic ketoacidosis secondary to thyrotoxicosis. The authors surmised that the effects of thyroid hormone on increasing beta-adrenergic receptors lead to increased lipolysis and an increased catabolic state which contributed to the ketoacidosis. Our patient had a lactic acidosis that was mostly due to the increased oxygen demand that is associated with an increased catabolic state. Signs and symptoms associated with thyrotoxicosis can be non-specific and may lead to delayed diagnosis. Similarly, Banerjee et al 2 in 2019 reported a case of a 45-year-old woman that presented with a 12-hour history of severe abdominal pain with associated nausea and vomiting. She was hypotensive and tachycardic and was initially treated for hypovolemia. She did not progress as expected and was subsequently diagnosed with thyrotoxicosis. Our patient was initially hypotensive and tachycardiac as well; however unlike some of the reported cases in the literature, our patient had findings concerning for an acute abdomen by both physical exam and radiographic imaging. Patients presenting with thyrotoxicosis can mimic those presenting with sepsis, heat stroke, gastrointestinal infection, or ischemic heart disease. Both these cases show that the non-specific presentation can lead to delayed diagnosis of thyrotoxicosis.
Though our patient was ultimately found to not have any intraabdominal pathology, the presence of HPVG and pneumatosis is a strong indication for immediate surgical intervention. Hepatic portal venous gas is rare but when present is associated with a number of life-threatening pathologies, some of which include intestinal ischemia and necrosis, hollow viscous perforation, and intraabdominal abscess. 4 The diagnosis of thyrotoxicosis in our patient was delayed, but given his presentation, ischemic bowel had to be ruled out first. When the patient presents with septic shock from an acute intraabdominal pathology, standard of care remains: Operative exploration to identify the source. However, once this has been ruled out, other less common sources should be explored, especially when the patient carries a history of hyperthyroidism. To the best of our knowledge, the presence of HPVG in a patient with thyrotoxicosis has not been previously reported in the literature and while it remains important to keep hyperthyroidism on the differential for patients presenting with severe abdominal pain, emergent exploration remains the mainstay for patients with evidence of an acute abdomen.
Thyrotoxicosis is rare but is associated with high mortality. Presenting symptoms are varied and often mimic other more common pathologies. Clinicians should remember that without identifiable causes of the signs and symptoms of an acute abdomen, hyperthyroidism should be on the working differential especially when the patient has a history of hyperthyroidism. Early diagnosis and treatment can greatly improve patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.