
Abstract
Introduction
For decades, a growing body of work has documented pervasive racial disparities in health care outcomes across the US.1–3 Indeed, Black race has been linked with significantly increased all-cause morbidity following numerous low- and high-risk surgical procedures, relative to non-Hispanic Whites.4,5 While the underlying mechanisms continue to be elucidated, prior work has attributed these inequities to greater disease severity at presentation, 2 increased likelihood of emergent surgery, and care at lower quality6,7 or lower volume hospitals. 8 Yet, a landmark report from the Institute of Medicine 9 and others 6 have suggested racial disparities in outcomes remain, even after adjusting for such patient and hospital factors.
Irrespective of cause, a myriad of efforts has been implemented at the regional and national levels to address race-based inequities in surgical outcomes, including the 2015 Patient Protection and Affordable Care Act (ACA), with discrepant results. While Mehtsun et al 10 noted a narrowing gap in postoperative mortality between Black and White Medicare patients, the study period occurred before implementation of ACA and Medicaid expansion. Others have more recently evaluated individual operations or limited cohorts, and reported continued racial inequities in outcomes.11,12 Ultimately, mitigating race-based inequities in outcomes remains a national imperative. A comprehensive understanding of how such disparities have evolved since the ACA is lacking but could guide future interventions and policy initiatives.
In this work, we evaluated the contemporary association of race with morbidity following major elective operations. We secondarily assessed the evolution of morbidity rates over the last five years. Lastly, we considered whether care at high-volume centers would mitigate any noted disparities in outcomes. We hypothesized that Black race would remain associated with inferior outcomes, without significant improvement over the study period. We further hypothesized that care at high-volume hospitals would reduce, but not eliminate, inequities in surgical outcomes.
Methods
Data Source and Study Cohort
All adult (≥18 years) hospitalization records entailing elective CABG, AAA repair, colectomy, and hip replacement were tabulated from the 2016-2020 National Inpatient Sample (NIS) using previously-validated International Classification of Diseases, Tenth Revision codes. These procedures were specifically selected as they are commonly performed across institutions in the US., and encapsulate a broad, nationally-representative cohort that would permit analysis of overall trends. 10 The NIS is the largest all-payer database reporting hospital discharge data and accounts for >97% of the U.S. population. 13
Variable Definitions and Study Outcomes
Patients were stratified by White or Black race, as reported in the NIS. Records entailing other race/ethnicity (13.6%) or missing key data were excluded (<1%, Figure 1). CONSORT Diagram of Survey-Weighted Estimates Of an estimated 2,838,485 records tabulated from the 2016-2020 National Inpatient Sample and included for analysis, 244,405 (8.6%) were of Black race. All estimates represent survey-weighted methodology.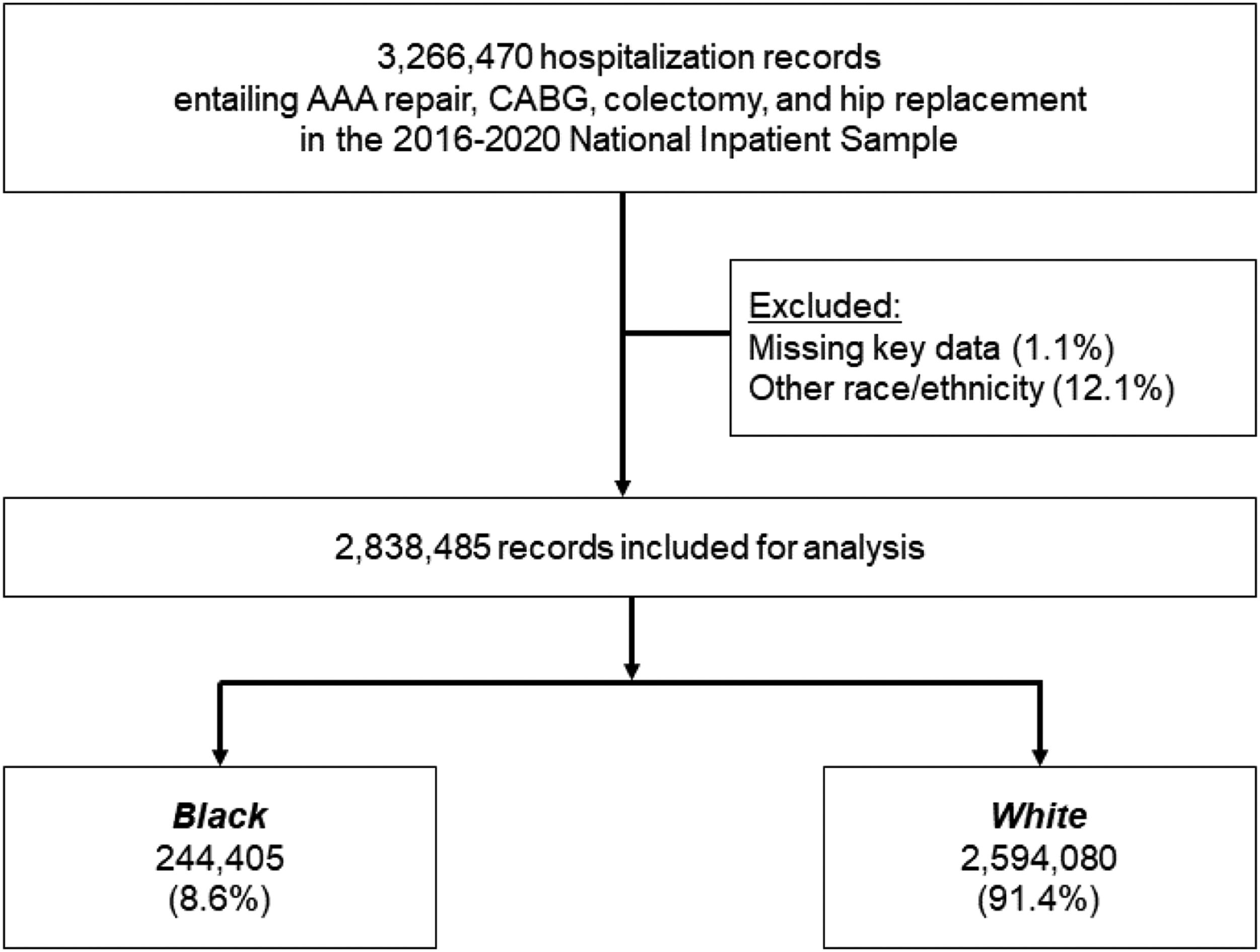
The Health care Cost and Utilization Project data dictionary was used to detail patient and hospital characteristics. 13 The van Walraven modification of the Elixhauser comorbidity index was applied to quantify the patient burden of chronic illness. 14 Relevant comorbidities and perioperative complications were ascertained using previously published ICD-10 codes. 15
Center-specific annual caseloads were computed for each operation. Institutions in the top quartile of annual volume were designated as high-volume hospitals (HVH) for the specific operative category. Specifically, centers were considered HVH for AAA repair if annual volume >10, for CABG if annual volume >279, for colectomy if annual volume >105, and for hip replacement if annual volume >200 cases.
The primary outcome of this study was in-hospital mortality. We secondarily evaluated the incidence of perioperative complications, duration of hospitalization, and discharge to extended care facilities.
Statistical Analysis
Variables are reported as medians with interquartile range (IQR) if continuous, or as group proportions (%), otherwise. The significance of intergroup differences was ascertained using the Mann-Whitney U, adjusted Wald, or Pearson’s chi-square test, as appropriate.
We subsequently fit multivariable regression models to consider the independent association of race with key study outcomes. Model covariates were automatically selected using elastic net regularization, which utilizes a penalized least-squares methodology to minimize model overfitting and increase out-of-sample generalizability. 16 Model covariates included patient age, sex, Elixhauser comorbidity index and relevant comorbidities, income quartile, rural/urban location, operation, hospital volume, hospital teaching status, hospital region, and year of admission. An interaction term was introduced between race and year of hospitalization. We then estimated the risk adjusted absolute point estimates for major morbidity. To consider temporal changes in adjusted risk of morbidity, we computed the delta in risk between cohorts for each year, over the study period.
The receiver operating characteristic was used to evaluate model goodness of fit. Logistic and linear model outputs are reported as adjusted odds ratios (AOR) and beta-coefficients (β), respectively, both with 95% confidence intervals (CI). Statistical significance was set at α = .05. All statistical analyses were performed using Stata 16.1 (StataCorp, College Station, TX). Due to the deidentified nature of the NIS, this study was deemed exempt from full review by the Institutional Review Board of the University of California, Los Angeles.
Results
Cohort Characteristics
Demographic, Clinical, and Hospital Characteristics.
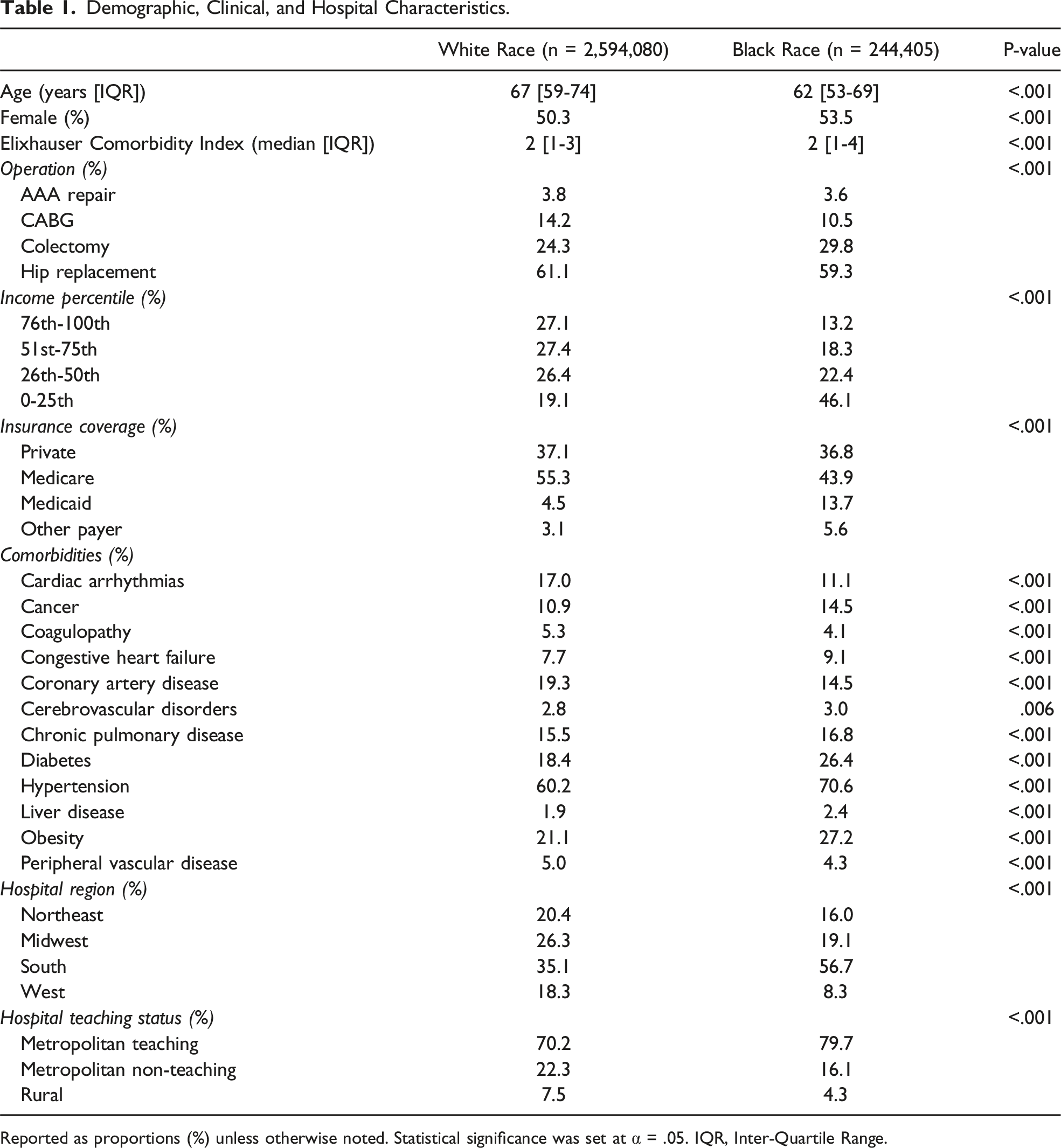
Reported as proportions (%) unless otherwise noted. Statistical significance was set at α = .05. IQR, Inter-Quartile Range.
Postoperative Outcomes
Unadjusted and Adjusted Outcomes Following Major Elective Procedures, Stratified by Race.
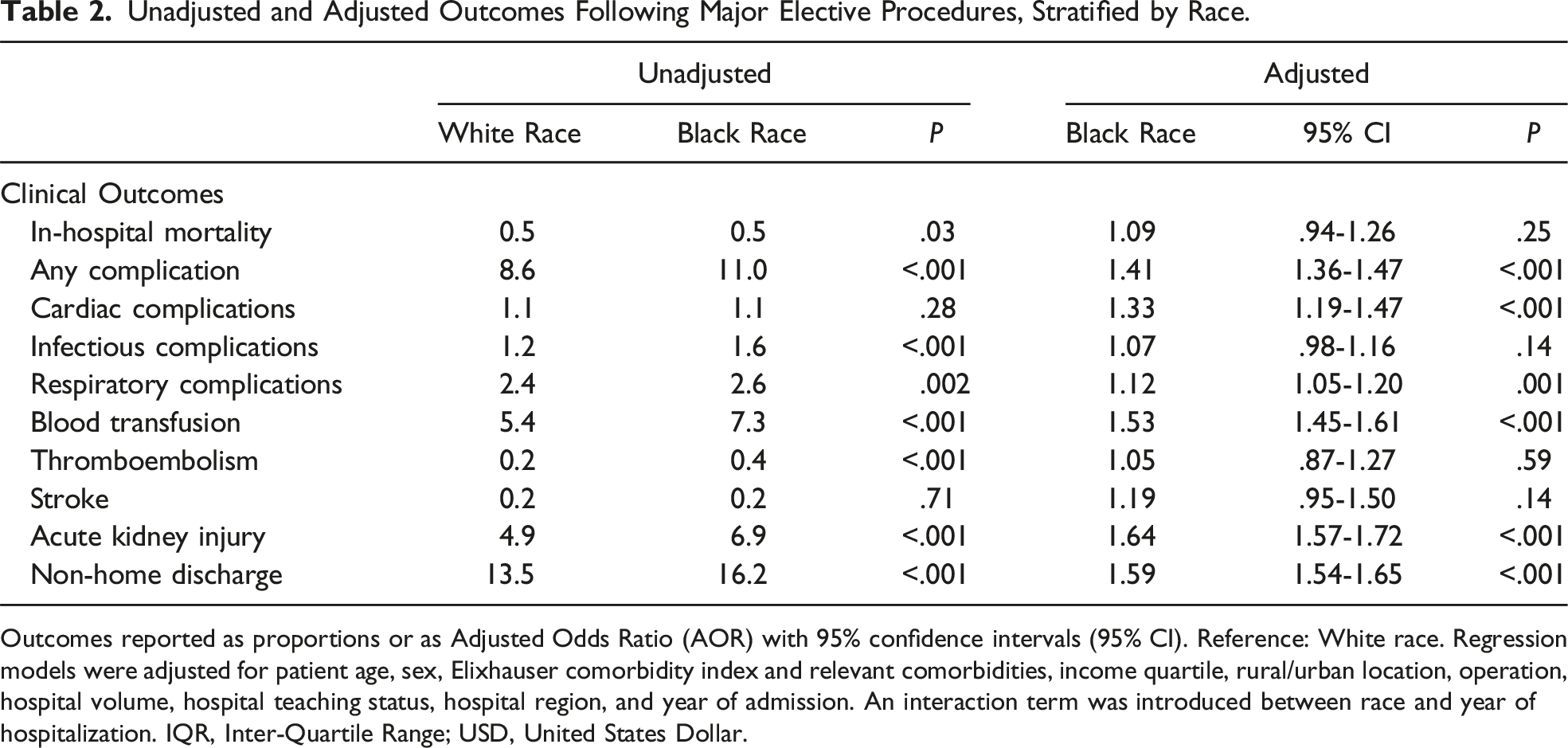
Outcomes reported as proportions or as Adjusted Odds Ratio (AOR) with 95% confidence intervals (95% CI). Reference: White race. Regression models were adjusted for patient age, sex, Elixhauser comorbidity index and relevant comorbidities, income quartile, rural/urban location, operation, hospital volume, hospital teaching status, hospital region, and year of admission. An interaction term was introduced between race and year of hospitalization. IQR, Inter-Quartile Range; USD, United States Dollar.
This persisted across each operation considered for analysis, such that the cohort of patients of Black race faced increased relative risk of complications following AAA repair (34.2 vs 27.2%), CABG (21.3 vs 16.4%), colectomy (17.3 vs 13.1%), and hip replacement (4.4 vs 3.2%) (Figure 2). Adjusted Risk of Complications, Stratified by Race. Following adjustment, patients of Black race demonstrated greater adjusted risk of major perioperative complications following elective AAA repair (34.2 vs 27.2%, P < .001), CABG (21.3 vs 16.4%, P < .001), colectomy (17.3 vs 13.1%, P < .001), and hip replacement (4.4 vs 3.2%, P < .001). * indicates statistical significance, P < .001. CABG, Coronary artery bypass grafting; AAA, abdominal aortic aneurysm.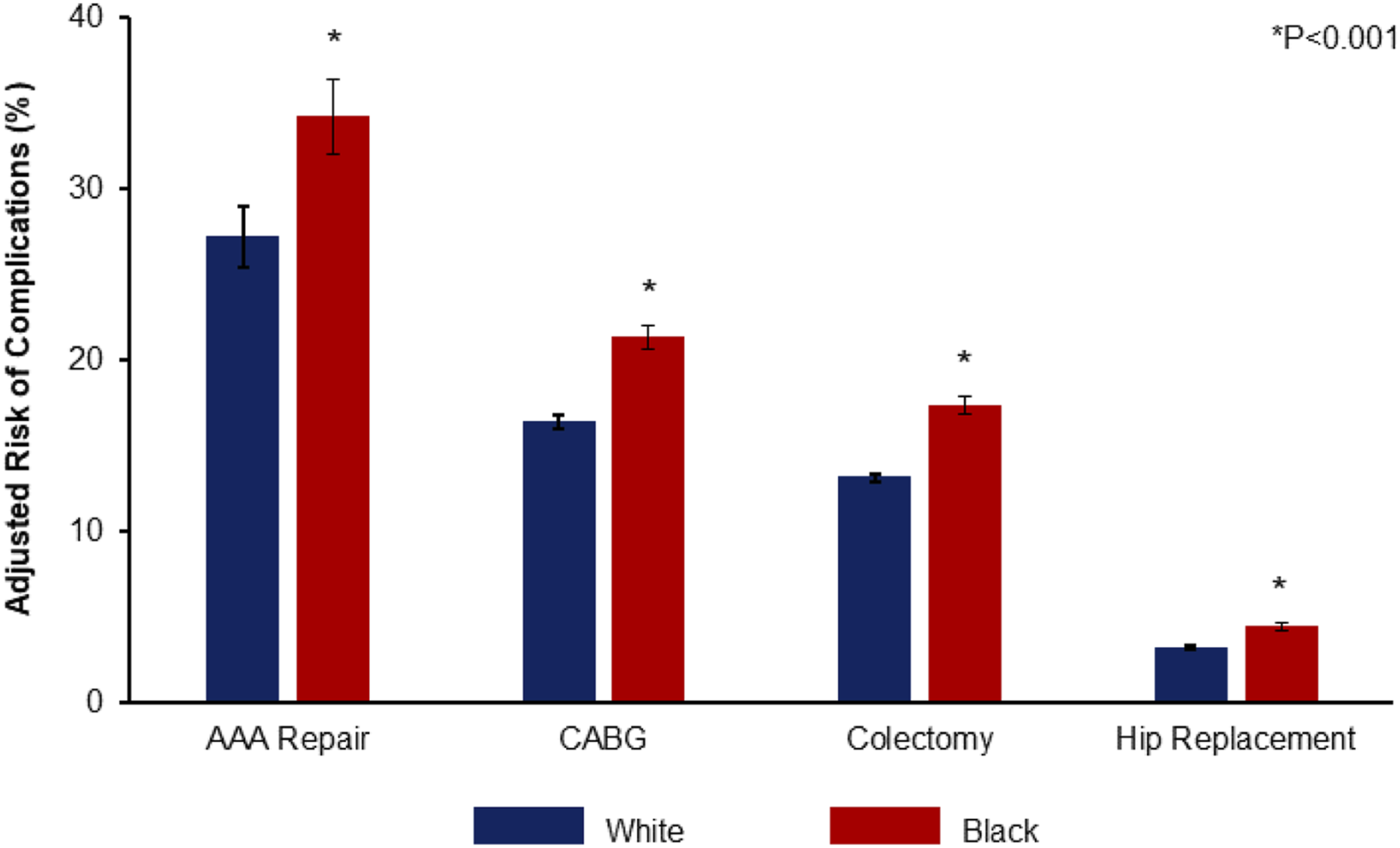
Temporal Trends
Evaluating elective operations from 2016 through 2020, risk-adjusted rates of major perioperative complications decreased for both those of White race (9.2% in 2016 to 8.4% in 2020, P < .001) and Black race (11.8% in 2016 to 10.8% in 2020, P < .001). However, no significant difference in the delta in adjusted risk of complications between patients of White and Black race was observed (2016 vs 2020: −Δ0.3%, CI −1.2 to .7%) (Figure 3). Temporal Trends in Adjusted Risk of Perioperative Complications. Following risk adjustment, Black race remained associated with greater likelihood of complications following elective operations, relative to White race. No significant change in the difference in adjusted risk of postoperative complications between patients of White and Black race was observed over the study period.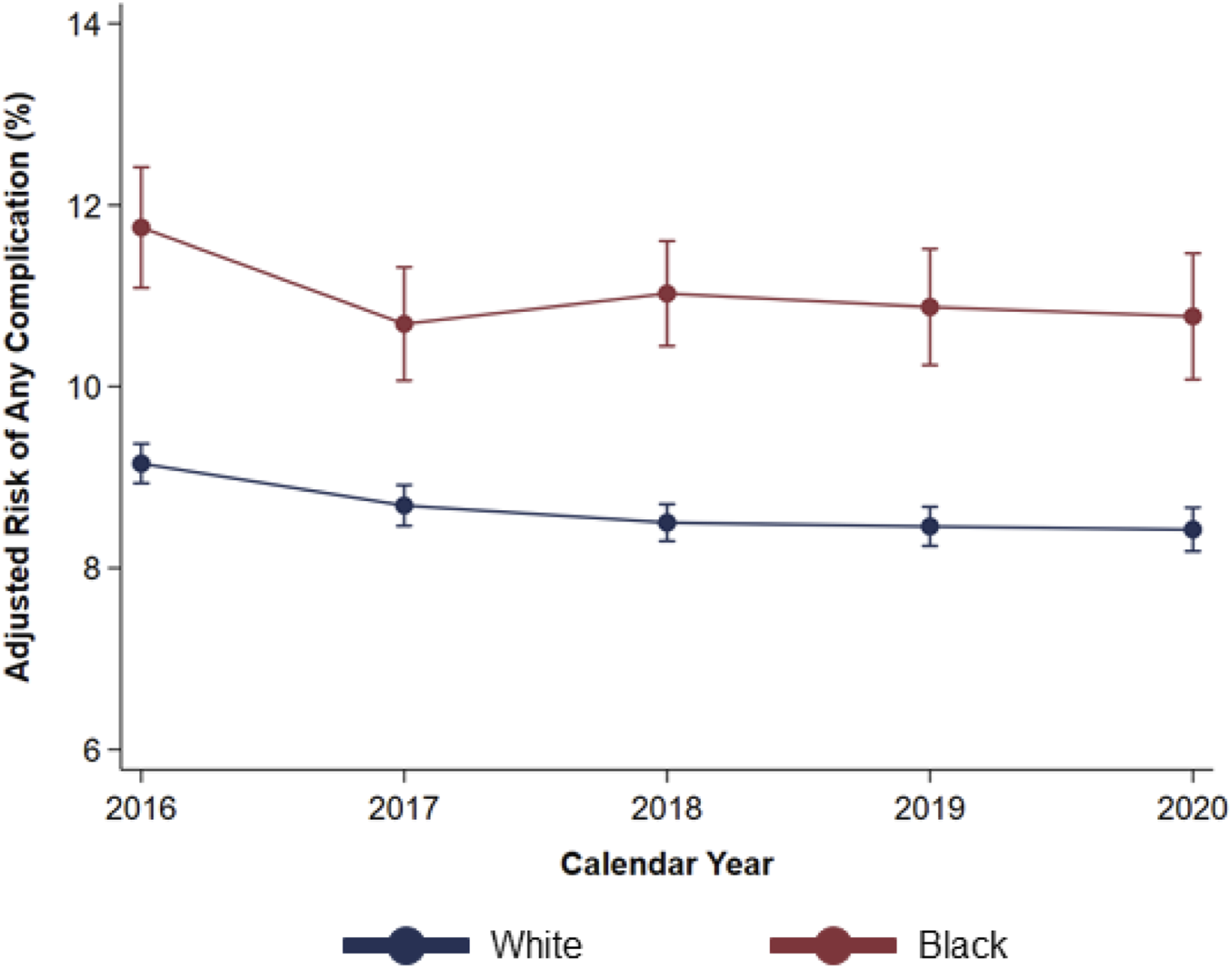
Impact of Elective Care at High Volume Hospitals
Among all patients, 1,883,691 (66.4%) were treated at HVH, of whom 158,060 (8.4%) were of Black race. On average, patients of Black race were younger, more frequently female, and more often treated in the South. The cohort of Black patients more frequently underwent AAA repair and colectomy, but less often CABG and hip replacement (Supplemental Table S1).
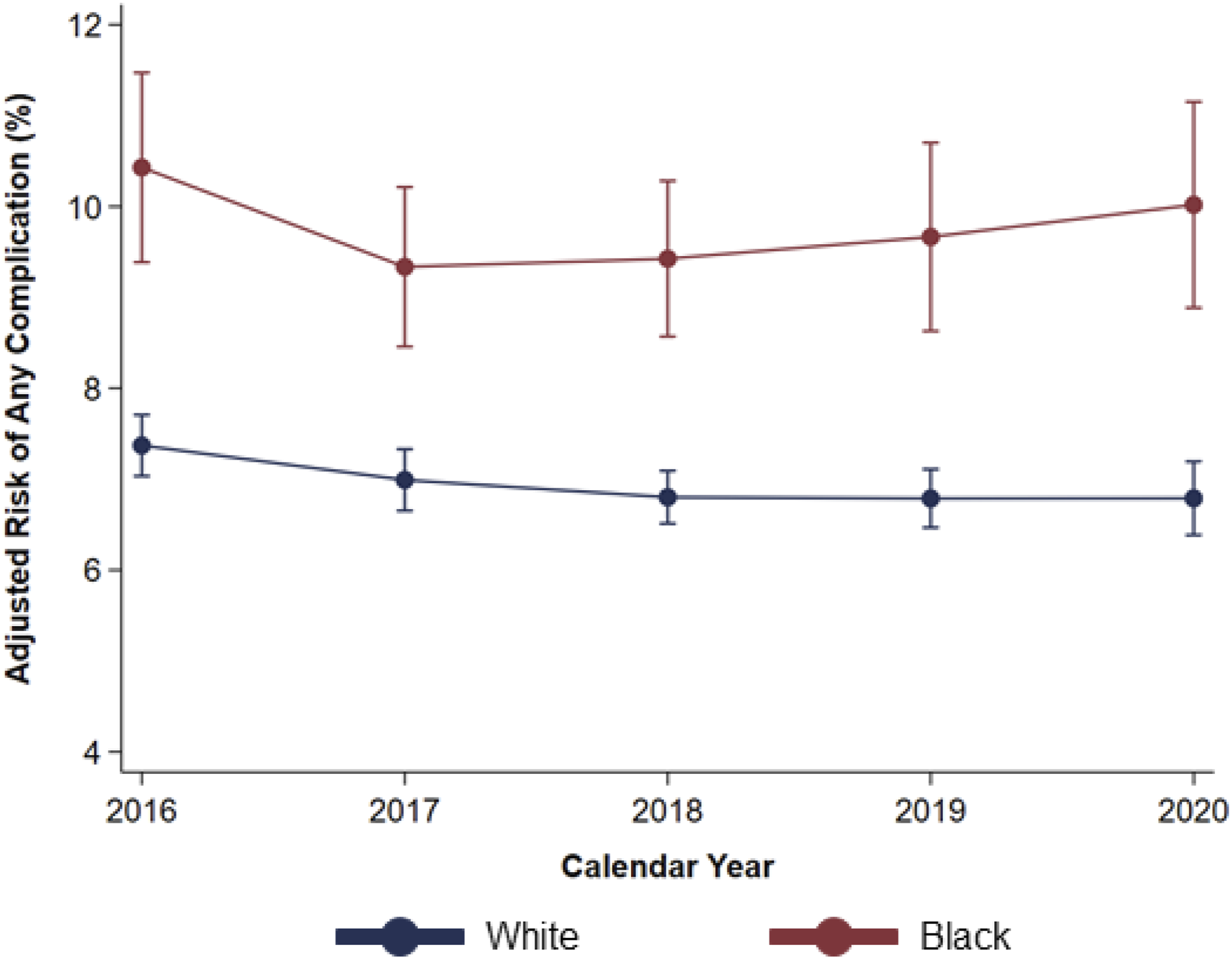
Following risk adjustment, and with White race as reference, Black race remained linked with similar in-hospital mortality, but greater likelihood of any major perioperative complication. Namely, Black race was associated with increased odds of stroke and acute kidney injury, as well as need for blood transfusion and non-home discharge (Supplemental Table S2). Upon stratification by operation type, patients of Black race remained associated with greater adjusted risk of perioperative complications following CABG, colectomy, and hip replacement, but not AAA repair (Figure 4). Further, the difference in risk of complications between patients of White and Black race did not meaningfully change over the study period (2016 vs 2020: Δ0.3%, CI -2.7 to 3.2%) (Figure 5). Risk-Adjusted Complication Rates at High-Volume Hospitals, Stratified by Operation Following adjustment, and considering only those electively admitted at HVH, patients of Black race continued to face increased risk of major perioperative complications following CABG (17.8 vs 13.6%), colectomy (16.0 vs 12.1%), and hip replacement (3.4 vs 2.5%), but similar likelihood following AAA repair (35.2 vs 28.3%). * indicates statistical significance, P < .001. HVH, High-Volume Hospital, CABG, Coronary artery bypass grafting; AAA, abdominal aortic aneurysm. Temporal Trends in Adjusted Risk of Perioperative Complications at High-Volume Hospitals. After risk adjustment, and only considering patients treated at high-volume hospitals, Black race remained associated with greater likelihood of complications following elective operations, relative to White race. No significant change in the difference in adjusted risk of complications following such procedures between patients of White and Black race was observed over the study period.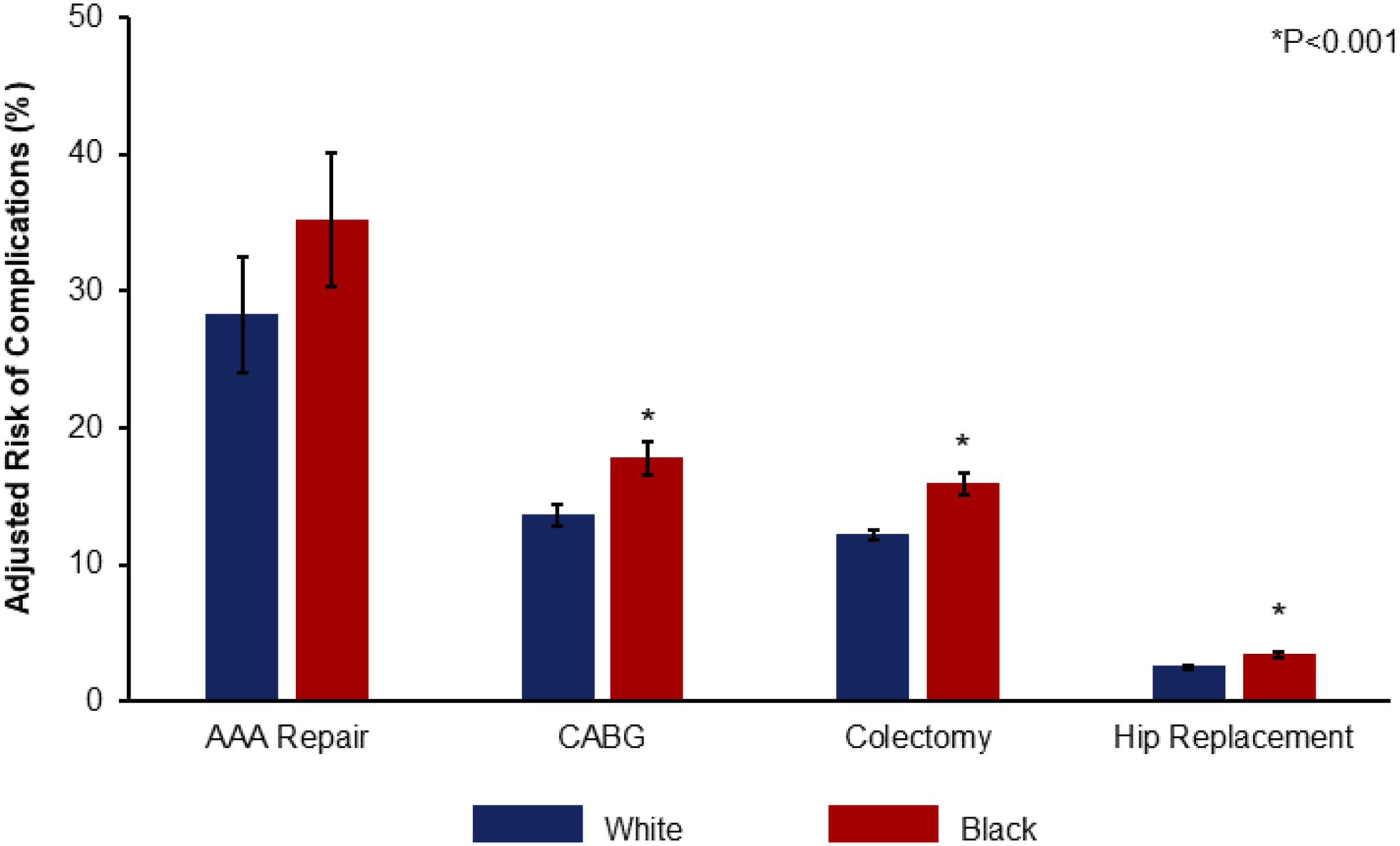
Discussion
In the present national analysis, we analyzed race-based disparities in morbidity following major elective operations, and made several important observations. Patients of Black race demonstrated significantly greater odds of postoperative complications. Notably, overall risk-adjusted rates decreased over time, but the disparity between Black and White patients persisted, such that patients of Black race continued to face greater morbidity risk over the study period. While care at high-volume centers was linked with lower morbidity, race-based differences in complications remained. With implications towards national policy and practice, these findings merit further discussion.
We noted significant racial disparities in morbidity rates following elective AAA repair, CABG, colectomy, and hip replacement. Indeed, patients of Black race faced greater likelihood of cardiac, respiratory, and renal sequelae following such procedures. These associations held true after controlling for comorbidity burden, as well as income and insurance coverage. Altogether, our findings add to a body of work stretching back two decades reporting racial disparities in surgical outcomes.1,3–6,9 Expanding on this literature, we identified continued outcomes inequities in the contemporary period.
Prior literature has attributed differences in postoperative complication rates to care at low-volume or low-quality institutions.7,8 Yet, we found the delta in risk between patients of Black and White race to remain similar regardless of center volume. Our findings, therefore, suggest expanding access to high-volume centers alone will not entirely mitigate race-based inequities. Interestingly, these findings contradict a study by Parson et al, 17 who reported similar outcomes between White and Black patients receiving cancer care at American College of Surgeons National Surgical Quality Improvement Program-participating hospitals. However, we postulate that the selected sample of patients undergoing cancer resection at such institutions may significantly differ from the national cohort of patients captured in this work. Furthermore, while expanding access to high-volume centers remains important, our study also calls for an examination of systemic and social contributors to outcomes inequities. In particular, efforts are needed to uncover and address implicit bias across physicians and hospitals, 18 improve the quality of patient-physician communication, 19 and ensure equitable care delivery, both during and after hospitalization. In both tangible and intangible ways, these factors may shape the quality of care patients receive, and may significantly influence their perioperative outcomes.
Across elective operations, irrespective of care at high-volume centers, race-based disparities in outcomes persisted over time. Importantly, a myriad of policies and programs aimed at addressing inequities in health outcomes have been implemented over the last decade, including the 2014 ACA. While such programs were linked with dramatic expansions of health insurance coverage and overall access to health care, literature has reported insignificant impact on hospitalization outcomes. 20 In our study, we found overall morbidity rates declined over time, yet the delta between Black and White patients has remained. Taken together, our findings suggest these programs may have improved care overall, but have been ineffective in addressing racial inequities. Of note, an earlier work by Mehtsun et al 10 reported decreasing racial inequities in postoperative mortality from 2010 to 2014. Our study found comparable mortality, but not morbidity rates between patients of Black and White race. A greater emphasis on postoperative morbidity as a quality metric in future policies and performance incentive programs may contribute to mitigating racial disparities.
The present work has several important limitations. As an administrative database, the NIS relies on ICD coding, which can vary based on local practices. Granular physiologic, laboratory, or radiographic data was unavailable for analysis. Degree of clinical severity or extent of disease burden was not accessible. However, the NIS has been used and validated extensively to analyze surgical outcomes. Lastly, due to the retrospective nature of this work, causal conclusions cannot be made. Despite these limitations, however, we applied robust analytical methods and evaluated a large, nationally-representative cohort, to consider the contemporary state of racial disparities in outcomes following major surgical operations.
In conclusion, we identified persistent disparities in postoperative morbidity among patients of Black and White race undergoing major elective surgery. This gap persisted across the five-year study period, without significant change. Additionally, while care at high-volume centers reduced overall rates of morbidity, racial disparities in outcomes remained. Future work is needed to elucidate the root cause of these inequities. Ultimately, national programs and policies are needed to more effectively mitigate the racial disparities gap beyond the efforts of the ACA.
Supplemental Material
Supplemental Material - Persistent Racial Disparities in Morbidity Following Major Elective Operations
Supplemental Material for Persistent Racial Disparities in Morbidity Following Major Elective Operations by Sara Sakowitz, Syed Shahyan Bakhtiyar, Saad Mallick, Giselle Porter, Konmal Ali, Amulya Vadlakonda, Joanna Curry, and Peyman Benharash in The American Surgeon™.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.