
Abstract
Key Takeaways
In patients undergoing laparoscopic cholecystectomy, postoperative COVID-19 infection is associated with increased risk for 30-day morbidity, reoperation, readmission, pneumonia, and DVT. Elevated complication rates in patients undergoing laparoscopic cholecystectomy diagnosed with postoperative COVID-19 support further investigation to optimize care for these patients.
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic has strained health care systems, causing disruptions and delays for patients in need of time-sensitive and crucial surgical procedures.1-4 Several studies demonstrated that surgery in COVID-19-positive patients was associated with higher mortality, increased thromboembolic events, and severe respiratory complications.4-6 These studies have contributed to guidelines that recommend preoperative COVID-19 screening and cancellation of elective cases in COVID-positive patients to minimize the risk of unwarranted adverse respiratory complications and spread of infection.3,7,8
No current guidelines exist for surgical patients regarding specific precautions to take after surgery to prevent or surveil for a COVID-19 infection beyond general CDC Guidelines for preventing COVID-19 spread. 9 Additionally, limited information is available to surgeons regarding the management of surgical patients recovering from an operation and concomitantly infected with COVID-19. Studying the impact of postoperative infection on surgical outcomes is therefore important to anticipate complications that may arise and guide management.
Most prior studies have looked more broadly at the impact of SARS-CoV-2 infection on surgical outcomes for a broad array of general surgery cases, even including vascular and orthopedic surgery cases.3,10,11 Few studies stratify outcomes based on specific surgeries performed or focus the investigation on a specific surgical procedure. Given the prevalence of gallbladder and gallstone disease in the U.S., this study focuses on patients undergoing laparoscopic cholecystectomy, one of the most common abdominal surgical procedures performed. 17 There is limited data on COVID-19 infections in patients undergoing laparoscopic cholecystectomy, a common elective and inpatient surgery, and the associated adverse outcomes after surgery.2,12 There is even less data on the impact of postoperative COVID-19 infection on outcomes in patients undergoing laparoscopic cholecystectomy. The aim of this study was to evaluate the outcomes associated with postoperative COVID-19 diagnosis in adult patients undergoing laparoscopic cholecystectomy.
Methods
This was a retrospective, case-control study utilizing the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) 2021 database. The NSQIP database is a peer-reviewed, multicenter clinical database containing de-identified data including patient demographics, preoperative comorbidities, and postoperative outcomes within 30 days after surgery. This study was approved by the Lundquist Institute as a non-human-subject study.
The NSQIP 2021 database, which included 685 participating hospitals, was queried for adult patients (age >18) with symptomatic cholelithiasis (K80x), acute cholecystitis (K81x), or gallstone pancreatitis (K85.1x) using ICD-10 codes. We then identified patients in this group undergoing a single procedure of laparoscopic cholecystectomy with (47562) or without intraoperative cholangiogram (47563) using current procedural terminology (CPT) codes. Based on postoperative COVID-19 infection status, patients were placed into two cohorts: those with postoperative COVID-19 diagnosis and those without postoperative COVID-19 diagnosis. Postoperative COVID-19 infection in this study is defined as lab-confirmed or suspected COVID-19 infection within 30 days following surgery in patients who were negative for COVID-19 pre-operatively. Patients with preoperative COVID-19 infection were excluded from this study (Figure 1). Flow of Included Patients and Coarsened Matching (CEM). Figure 1 Legend. COVID-19, Coronavirus Disease 2019; CPT, Current Procedural Terminology; ICD-10, International Classification of Diseases, Tenth Revision; IOC, intraoperative cholangiography; and NSQIP, National Surgical Quality Improvement Program.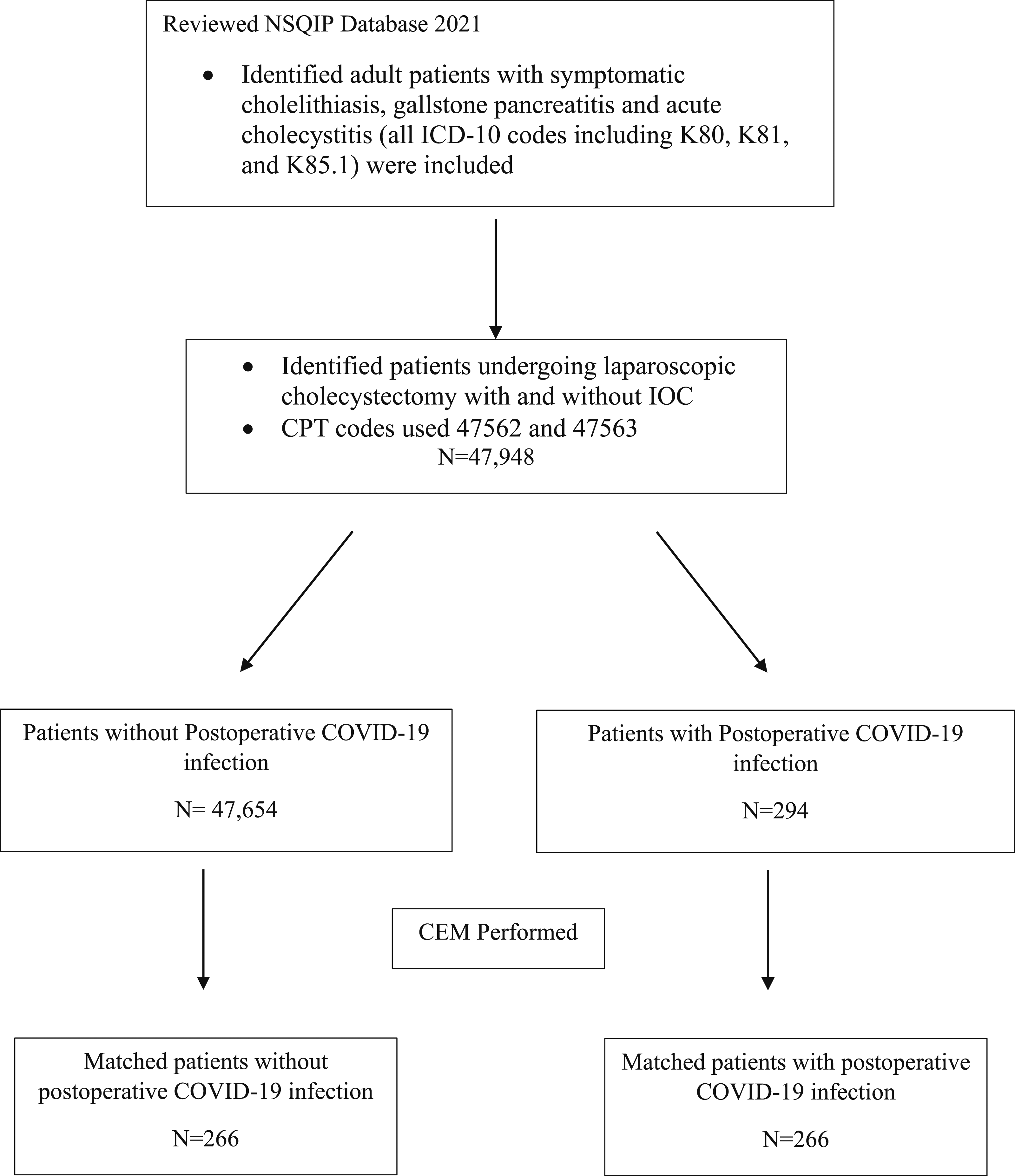
Demographic characteristics including age, sex, race, ethnicity, and body mass index (BMI) were collected. Medical comorbidities including diabetes, smoking, chronic obstructive pulmonary disease (COPD), history of ascites, congestive heart failure (CHF), hypertension (HTN), dialysis dependence, metastatic cancer, steroid use, as well as additional factors including preoperative ventilator support, elective vs urgent status of surgery, preoperative transfusion requirements, preoperative sepsis, and American Society of Anesthesiologists Classification (ASA class) were analyzed in both patient groups. Low ASA class in this study was defined as Class I and II.
The primary outcome measures of the study were 30-day mortality and 30-day morbidity, which is a composite variable of the presence of any NSQIP-defined 30-day postoperative complication. Secondary outcome measures included any surgical site infection (SSI), reoperation, readmission, length of stay, postoperative pneumonia, reintubation, pulmonary embolism (PE), ventilator need >48 hours, renal failure, urinary tract infection (UTI), stroke, cardiac arrest, myocardial infarction (MI), deep venous thrombosis (DVT), postoperative sepsis, postoperative septic shock, and transfusion requirement postoperatively.
The primary and secondary outcomes were compared between patients who underwent laparoscopic cholecystectomy who developed postoperative COVID-19 and those without postoperative COVID-19 in the aggregate cohort. Using differences in preoperative characteristics between the two cohorts that were statistically significant at a P < .05, the match criteria was determined. Coarsened Exact Matching with K:K methodology was used to match patients who underwent laparoscopic cholecystectomy with postoperative COVID-19 with those without postoperative COVID-19 based on age, BMI, smoking, COPD, CHF, preoperative sepsis, and ASA class. There were no differences in demographics and comorbidities in between cohorts in the matched group after Coarsened Exact Matching. The primary and secondary outcomes were compared between the two groups in both cohorts.
SPSS V28 (IBM Corp, Armonk, New York) was used to perform statistical analysis for this study. A 2-sided P < .05 was considered statistically significant. Continuous data was compared using the Student’s t test, categorical data was compared using Pearson χ2 and Fisher’s exact tests, and matched categorical data was analyzed using the Cochran-Mantel-Haenszel test.
Results
Demographics and Perioperative Characteristics of Aggregate and Matched (−) Post Op COVID and (+) Post Op COVID Cohorts.
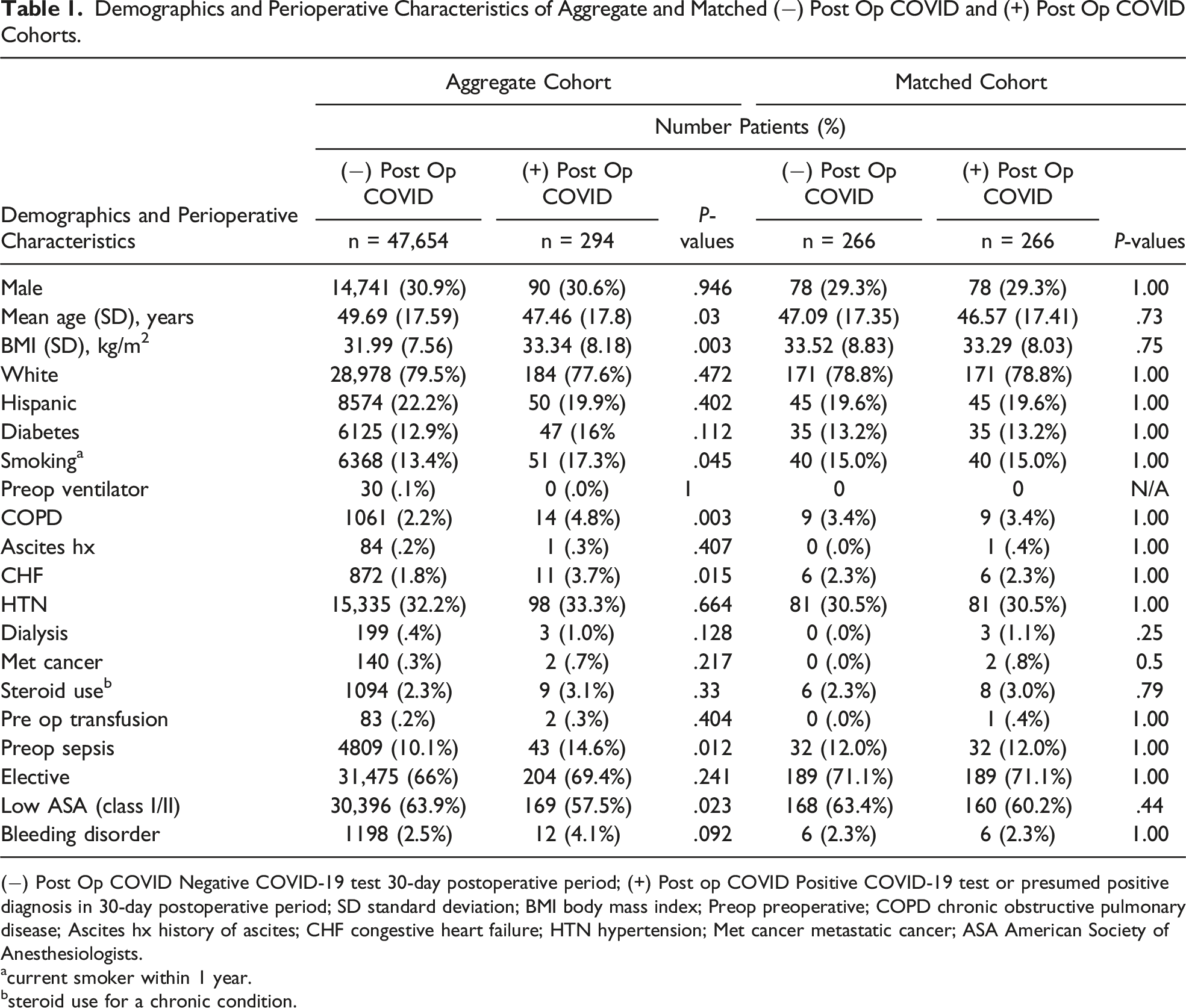
(−) Post Op COVID Negative COVID-19 test 30-day postoperative period; (+) Post op COVID Positive COVID-19 test or presumed positive diagnosis in 30-day postoperative period; SD standard deviation; BMI body mass index; Preop preoperative; COPD chronic obstructive pulmonary disease; Ascites hx history of ascites; CHF congestive heart failure; HTN hypertension; Met cancer metastatic cancer; ASA American Society of Anesthesiologists.
acurrent smoker within 1 year.
bsteroid use for a chronic condition.
30-Day Postoperative Outcomes for Patients With and Without Postoperative COVID-19 Undergoing Laparoscopic Cholecystectomy in Aggregate Cohort.
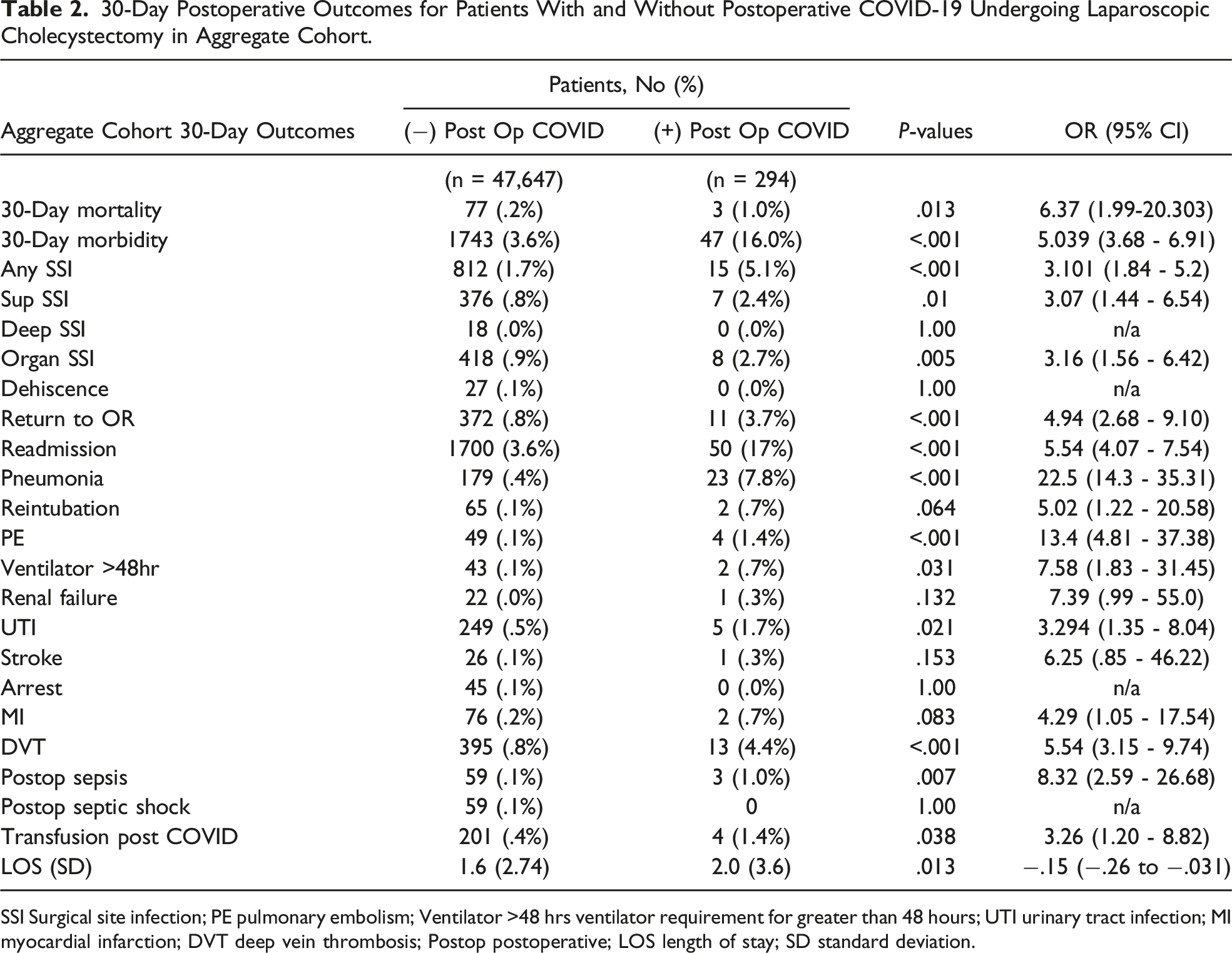
SSI Surgical site infection; PE pulmonary embolism; Ventilator >48 hrs ventilator requirement for greater than 48 hours; UTI urinary tract infection; MI myocardial infarction; DVT deep vein thrombosis; Postop postoperative; LOS length of stay; SD standard deviation.
30-Day Postoperative Outcomes for Patients With and Without Postoperative COVID-19 Undergoing Laparoscopic Cholecystectomy in Matched Cohort.
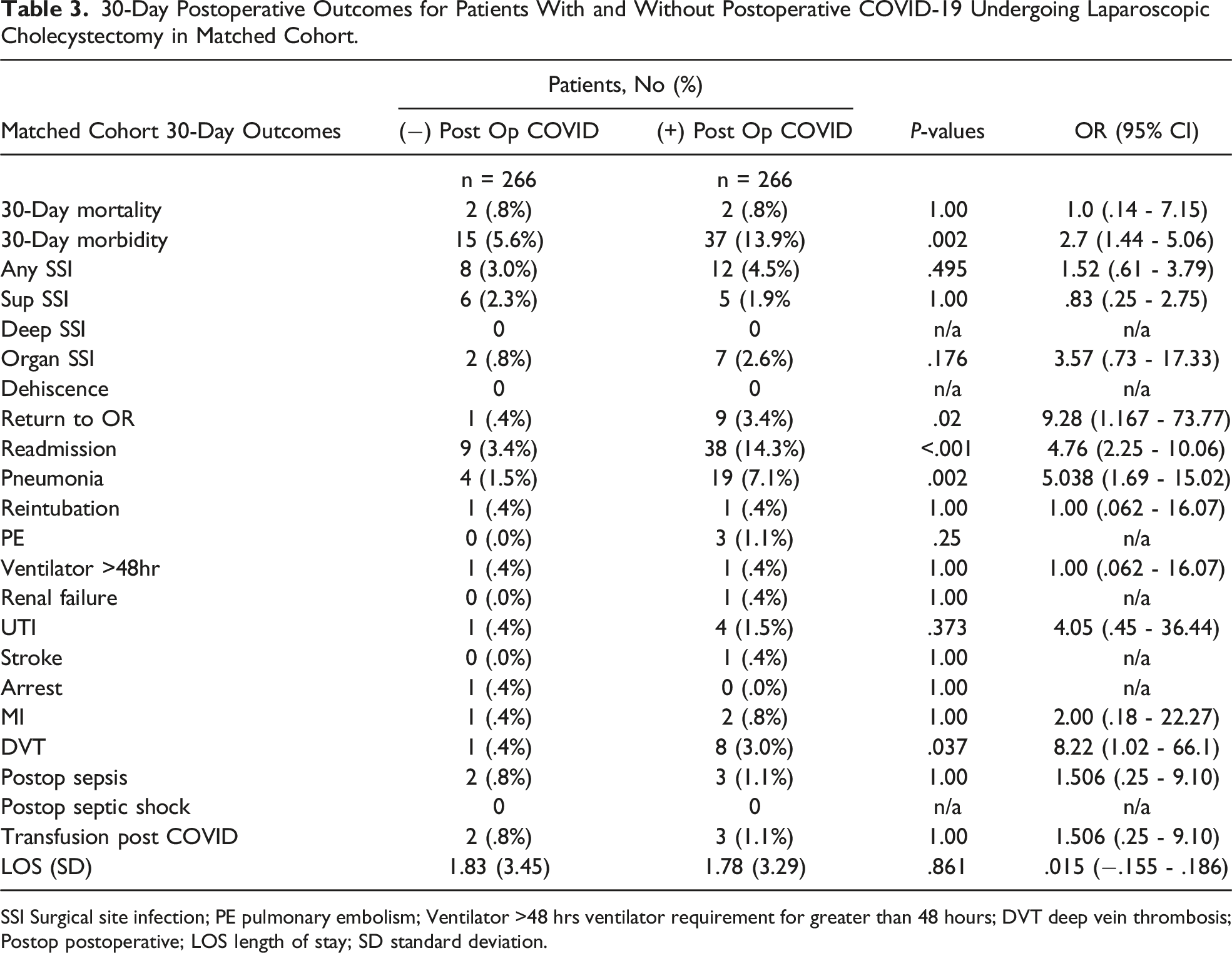
SSI Surgical site infection; PE pulmonary embolism; Ventilator >48 hrs ventilator requirement for greater than 48 hours; DVT deep vein thrombosis; Postop postoperative; LOS length of stay; SD standard deviation.
Discussion
In this retrospective, national database study, patients undergoing laparoscopic cholecystectomy with a postoperative COVID-19 infection had an increased likelihood of experiencing many 30-day postoperative complications. After matching, patients who underwent laparoscopic cholecystectomy with a postoperative COVID-19 diagnosis had an increased likelihood of 30-day morbidity, reoperation, readmission, pneumonia, and DVT. Research early in the pandemic focused predominantly on the impact of preoperative COVID-19 on surgical outcomes in order to develop guidelines for physicians taking care of patients and determining the need for delaying or canceling cases.4,5,6 This study, however, demonstrates notable findings of the impact of postoperative COVID-19 infection on surgical outcomes in a commonly performed surgical procedure and can guide further investigation and risk assessment of surgical patients diagnosed with postoperative COVID-19.
Our findings are consistent with studies to date on the surgical risks associated with perioperative COVID-19 infection.10,12,13 Prasad et al (2021), in a large prospective multicenter study of Veteran Affairs hospital system, found a similar rate of postoperative COVID-19 infection of .5% in their study population, which included patients undergoing elective orthopedic, gastrointestinal, cardiothoracic, ophthalmologic, neurosurgical, and urologic surgeries in 2020. Their study also found that patients with postoperative COVID-19 infections had higher rates of mortality, readmission, reoperation, pneumonia, DVT, and longer LOS in addition to a number of other complications, though their study included a composite of surgical procedures with variable risk, unlike our study, which focused on a single surgical procedure. 10
Postoperative pneumonia in surgical patients contributes to increased morbidity, mortality, and length of stay for surgical patients. 14 For patients undergoing laparoscopic cholecystectomy, approximately 2% of patients were noted to develop postoperative pneumonia in a large retrospective, population-based cohort study by Teng et al (2021). 14 In our study, we found nearly 7-fold (1.5% to 7.1%) increase in the risk of postoperative pneumonia in COVID-19-positive patients in the matched cohort undergoing laparoscopic cholecystectomy. Prasad et al similarly found that 23% of patients with postoperative COVID-19 developed pulmonary complications, which included pneumonia, acute respiratory distress syndrome, and ventilation compared to 2.3% of COVID-19-negative patients. 10 In another study looking at perioperative COVID-19 infection and surgical outcomes in elective, urgent and emergent cases, Peters et al found that postoperative pneumonia occurred in approximately 1% of patients without COVID-19, 2% of patients with pre-operative COVID-19 diagnosis and 13.5% of patients with postoperative COVID-19. 12 Postoperative COVID-19 infection has been consistently shown, in the few studies that have examined its effects, to significantly increase the risk of postoperative pneumonia. It warrants further investigation into how to best combat the development of pneumonia in COVID-19-positive patients recovering from surgery, as there is currently little evidence that factors such as incentive spirometer or pulmonary toilet make a significant difference in rates of postoperative pneumonia for surgical patients.
In our study, we found a significant increase in the rate of DVT in patients with postoperative COVID-19 undergoing laparoscopic cholecystectomy in both our aggregate and matched cohorts. COVID-19 has been shown to increase the risk of thromboembolic events, which again leads to higher rates of mortality, morbidity, and hospital LOS. 15 Patients undergoing surgery are already at higher risk of developing venous thromboembolic events (VTE) due to prolonged immobilization and systemic inflammation. 4 A study done by COVIDSurg Collaborative found that patients undergoing surgery with perioperative or recent COVID-19 diagnosis had a nearly 50% increased risk of postoperative venous thromboembolism and mortality secondary to venous thromboembolism was significantly higher in patients with perioperative COVID-19 infection. 4 There is currently little data to support the use of prophylactic antithrombotic treatment in patients with COVID-19 diagnosis in the outpatient setting, however, patients should be counseled on their increased risks of VTE and the signs and symptoms if they develop COVID-19 in the postoperative period. 16 Further studies looking into the prevention of VTE in surgical patients with COVID-19 should be considered.
There are limitations to this study, which include its retrospective design, which can limit our ability to account for confounding factors that may have influenced both COVID-19 diagnosis and poor outcomes. While there are many notable benefits to using the NSQIP database including large patient numbers, which provides power to studies utilizing its data, there are also limitations. The first limitation of the NSQIP database for our study is the accuracy of diagnosis of COVID-19. The NSQIP database criteria for postoperative COVID-19 infection used was a patient with a positive test or presumed positive diagnosis within 30 days of surgery who was negative preoperatively. They do not offer specifications on what symptoms attributed a “presumed” diagnosis or the number or type of tests that were used (PCR vs nucleic acid amplification tests) for “laboratory confirmed” diagnosis. Additionally, neither the exact date from surgery nor suspected vs laboratory confirmed diagnosis were able to be differentiated in this group, which allows for the possibility of a COVID-19 diagnosis in our sample to represent a false negative preoperative COVID-19 diagnosis or potentially a similar presenting upper respiratory infection. Another area of future study is the impact of vaccination on preoperative and postoperative COVID-19 infection as it relates to surgical outcomes. Currently, the NSQIP database does not include vaccination status, it is therefore not possible to determine if vaccinated patients with COVID-19 infection are protected from more serious surgical outcomes.
Another factor we cannot control for in this study is the potential impact that surgeon decision making may have had on the management of gallbladder pathology during our 2021 study period. As we discussed earlier, the COVID-19 pandemic impacted patient selection for surgery and surgeon decision making, given limitations on resources and concerns about increased adverse outcomes when operating on COVID positive patients. During our study period the threshold for operating on patients with acute cholecystitis, gallstone pancreatitis and symptomatic cholelithiasis may have changed from pre-pandemic times. It is possible that NSQIP outcomes reflected in this study may have been altered if patients undergoing laparoscopic cholecystectomy were generally sicker, and in need of more urgent surgery.
There are reports that during the pandemic there was an increase in conservative management for acute cholecystitis, supporting the hypothesis that primarily sicker patients were undergoing surgery. Ruhi-Willams et al (2023), a retrospective, large national database study looking at the impact of the COVID-19 pandemic on the management of acute cholecystitis found compared to pre-pandemic, there was a statistically significant rise in use of cholecystostomy tubes (18% vs 21.5%) and medical management (29.4% vs 31.8%) during the pandemic. 18 There is evidence that the pandemic changed decision-making on who underwent surgery with the limited resources; however, it is not possible to say in our study how that may have impacted results as data on conservative management and cholecystostomy tube use was not collected by NSQIP, and therefore not included in this study. It is possible that our results demonstrating increased 30-day morbidity, reoperation, readmission, pneumonia, and DVT may be partially due to patients undergoing surgery during the pandemic being generally sicker.
Finally, a clear limitation of all studies looking at impact of COVID-19 infection on surgical outcomes is delineating the impact COVID-19 has alone on outcomes given known cardiac, respiratory, and hematologic complications associated with COVID-19 and distinguishing synergistic effects of the surgical process and COVID-19 on surgical complications and outcomes. In our study, we have demonstrated a statistically significant impact of postoperative COVID-19 on surgical outcomes. It is not certain, however, if these outcomes would be different for these patients if they were not undergoing surgery. Clinical significance of this may be overstated, as adverse outcomes may be due primarily to COVID-19 infection.
Conclusion
The findings of our study, which demonstrates that patients undergoing laparoscopic cholecystectomy with postoperative COVID-19 infection have worse postoperative outcomes, suggest that these patients may warrant increased attention to mitigate their risks for adverse outcomes. Like surgical patients with a preoperative COVID-19 infection, guidelines for the care of patients diagnosed with COVID-19 after common surgical procedures such as laparoscopic cholecystectomy, may help improve their outcomes. Additionally, clinicians could consider simple targeted efforts to reduce the likelihood of complications such as counseling patients to take extra care in the immediate postoperative period to limit the risk of contracting COVID-19 and instructing patients to notify their provider if they develop COVID-19 in the postoperative period for closer monitoring.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.