
Abstract
Introduction
The Lower Anogenital Squamous Terminology (LAST) Project recommended unified classification for HPV–associated squamous lesions of the lower anogenital tract, using a 2-tiered nomenclature in 2013. Adherence to the new nomenclature worldwide is unknown. This study aims to assess the trend of the use of the two-tiered High Squamous Intraepithelial Lesion and Low Squamous Intraepithelial Lesion (HSIL/LSIL) as opposed to the traditional three-tiered Anal Intraepithelial Neoplasia (AIN I/II/III) classification as suggested by the LAST Project.
Methods
A literature search on full-text English language studies of premalignant anal lesion was performed on PubMed from 2002-2022. The studies were categorized by continent, and the prevalence of HSIL/LSIL classification vs AIN I/II/III was calculated.
Results
546 studies and 251 studies were identified using the AIN I/II/II and the HSIL/LSIL classification respectively. Global trend suggested a statistically significant downward trend in the use of the two-tiered nomenclature system in publications globally. Regional trend including North America, Europe, and other (Asia and Latin America) showed variance in adoption of the two-tiered nomenclature system.
Conclusion
Despite multidisciplinary collaborative effort, adherence to the recommendations to use the two-tiered system for HPV-associated premalignant anal lesions continues to be suboptimal. Further efforts are needed to identify the cause of poor adherence to be able to create strategies that reinforces unification of terminology and integration of LAST the recommendations.
Key Takeaway
• HPV is one of the most common sexually transmitted disease and has been associated to caner. Premalignant lesions can precede anal cancer. Throughout the years various terminologies have emerged to describe these premalignant lesions. • In 2012 the LAST Project was initiated to establish a histopathological nomenclature system that aligns with the current knowledge of HPV, optimizes biomarker utilization, and facilitates clear communication across various medical specialties. • The findings of our research indicate that the adherence to the recommendations to use the two-tiered system for HPV-associated premalignant anal lesions remains poor.
Introduction
Human Papillomavirus (HPV) is one of the most common sexually transmitted diseases in the world. 1 The lifetime risk of anogenital HPV is around 80%–90% in people with at least one opposite-sex partner. 2 There are about 150 genotypes for HPV, 40 of which can infect the anogenital organs, with a significant subset specifically affecting the anal region. 3 Types 15-20 are considered high-risk due to their association with invasive squamous cell carcinoma, and the remaining low-risk types are associated with warts. Ninety percent of anal cancer is caused by high-risk HPV, but only a small percentage of the infected population develops anal cancer. 3
While the long-term natural history is insufficiently established, premalignant lesions can precede anal cancer in the setting of HPV infection. 4 Various terminologies have emerged over the years to describe these premalignant lesions. Terms such as surface carcinoma, intraepithelial carcinoma and carcinoma in situ. 5 In 1969, Richart proposed that cellular atypia, dysplasia, and cervical neoplasia are all phases of a continuous disease spectrum. 6 He introduced the histological categories of cervical intraepithelial neoplasia (CIN) 1, 2 and 3 to grade the degree of dysplasia. 6 Subsequently in the 1980s as the understanding of HPV pathophysiology and oncogenesis improved a two-tiered system was established.7,8 The new low- and high-grade squamous intraepithelial lesions (HSIL/LSIL) classification was more biologically relevant and was noted to have more consistent pathological interrater reproducibility than the previous 3-tiered system.9,10
However, the existence of multiple terms to reference the same process led to challenges in patient care. 11 For instance, unclear medical approach in the setting of –IN2 and unnecessary hysterectomy when facing a carcinoma in situ pathology report. 11 In an effort to address these challenges, the LAST project was stablished in 2013. This collaborative effort involved the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. 12 The team of experts were organized into five working groups (WG) comprised of surgical pathologists, gynecologic pathologists, dermatopathologists and medical and surgical specialists including dermatologists, infectious disease specialists, gynecologists, gynecologic oncologists, urologists and colorectal surgeons. The primary goal was to establish a histopathological nomenclature system that aligns with the current knowledge of HPV, optimizes biomarker utilization, and facilitates clear communication across various medical specialties. As a consensus, the working groups recommended a two-tiered HSIL/LSIL nomenclature for noninvasive HPV-associated squamous proliferation of the LAT. Additionally, they advocated for the use of biomarkers such as p16 to provide clarification in situations where a classification of a lesion into HSIL or LSIL is not readily evident. 11
Over a decade has passed since the publication of the LAST project. However, the global adoption of this two-tiered terminology remains unknown. The aim of this study is to assess global trends and regional variances in the usage of the two-tiered classification system. We hypothesize that the adherence rate of the two-tiered system has increased since the release of the LAST project recommendations.
Methods
This study constitutes a literature review and does not involve any original human subject research; therefore, Institutional Review Board (IRB) approval is not applicable to this study.
Data Collection and Analysis
A literature review was conducted in the PubMed database between 2002 and 2022. The search strategy was limited to English language articles and was conducted using predefined terms, including a combination of relevant keywords such as “Anal intraepithelial neoplasia (AIN), squamous intraepithelial lesion (SIL), High-grade squamous intraepithelial lesion (HSIL), low squamous intraepithelial lesion (LSIL). To refine our search strategy, the following terms were excluded: “vulvar, cervical, vaginal, cervix, scrotal, penile, pap smear and loop excision.”
Statistical Analysis
Records yielded from the search were sorted by publication year and categorized by continent to analyze geographical trends in adopting HSIL/LSIL as a new classification system. The annual percentage change in the number of publications was calculated, and trend analysis was performed using the Jonckheere-Terpstra trend test. The directionality of the trend was assessed to examine changes over time, particularly focusing on the period before and after the introduction of the LAST recommendations in 2013. StataSE 17.0 (StataCorp, College Station, TX) was used for all analyses.
Results
A total of 797 studies was identified (Figure 1). Of these, 546 used the three-tiered nomenclature, while 251 used the HSIL/LSIL classification. The adoption rates of the new classification varied significantly by regions and over time. Literature review diagram.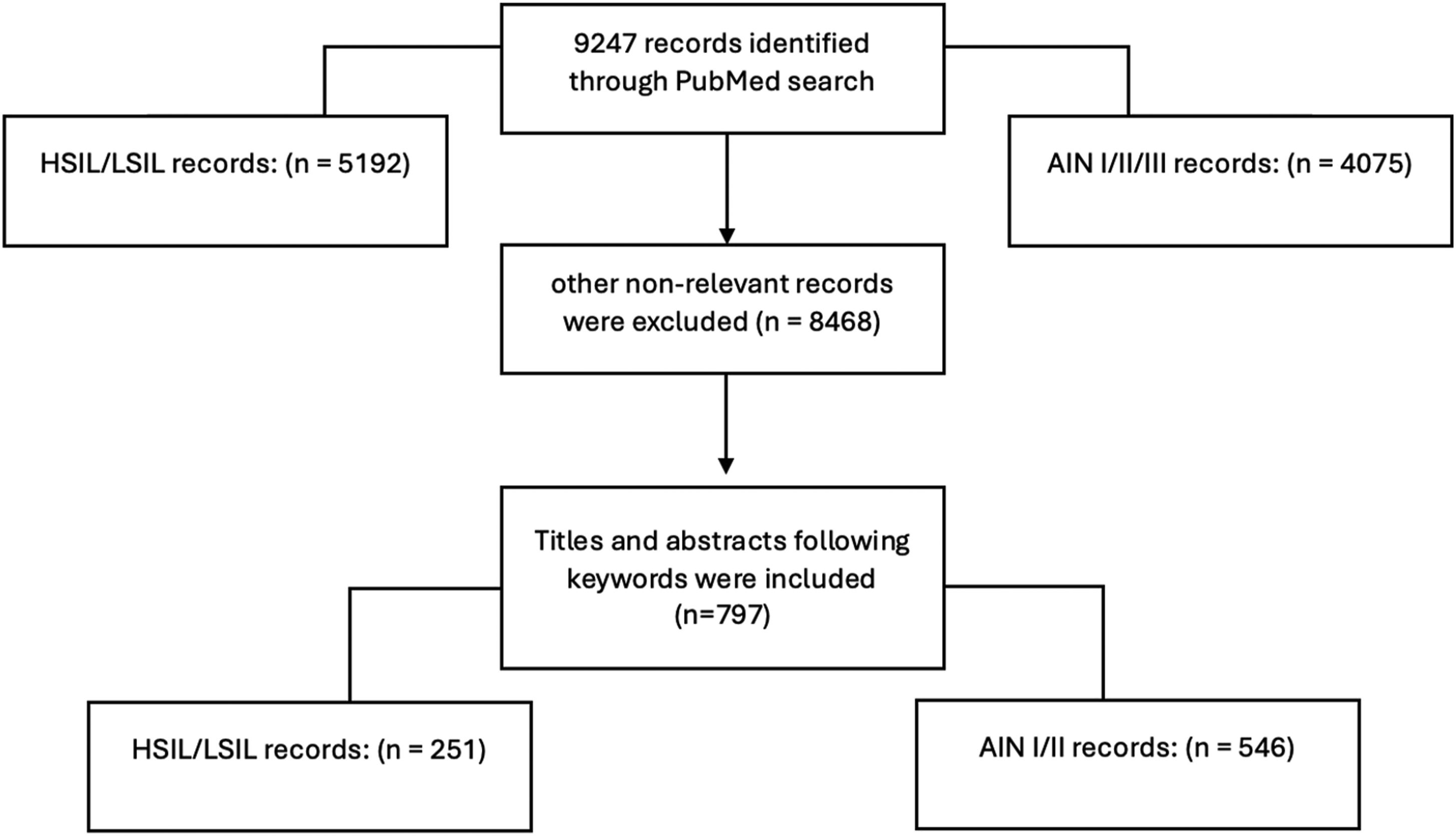
Global Trend Analysis
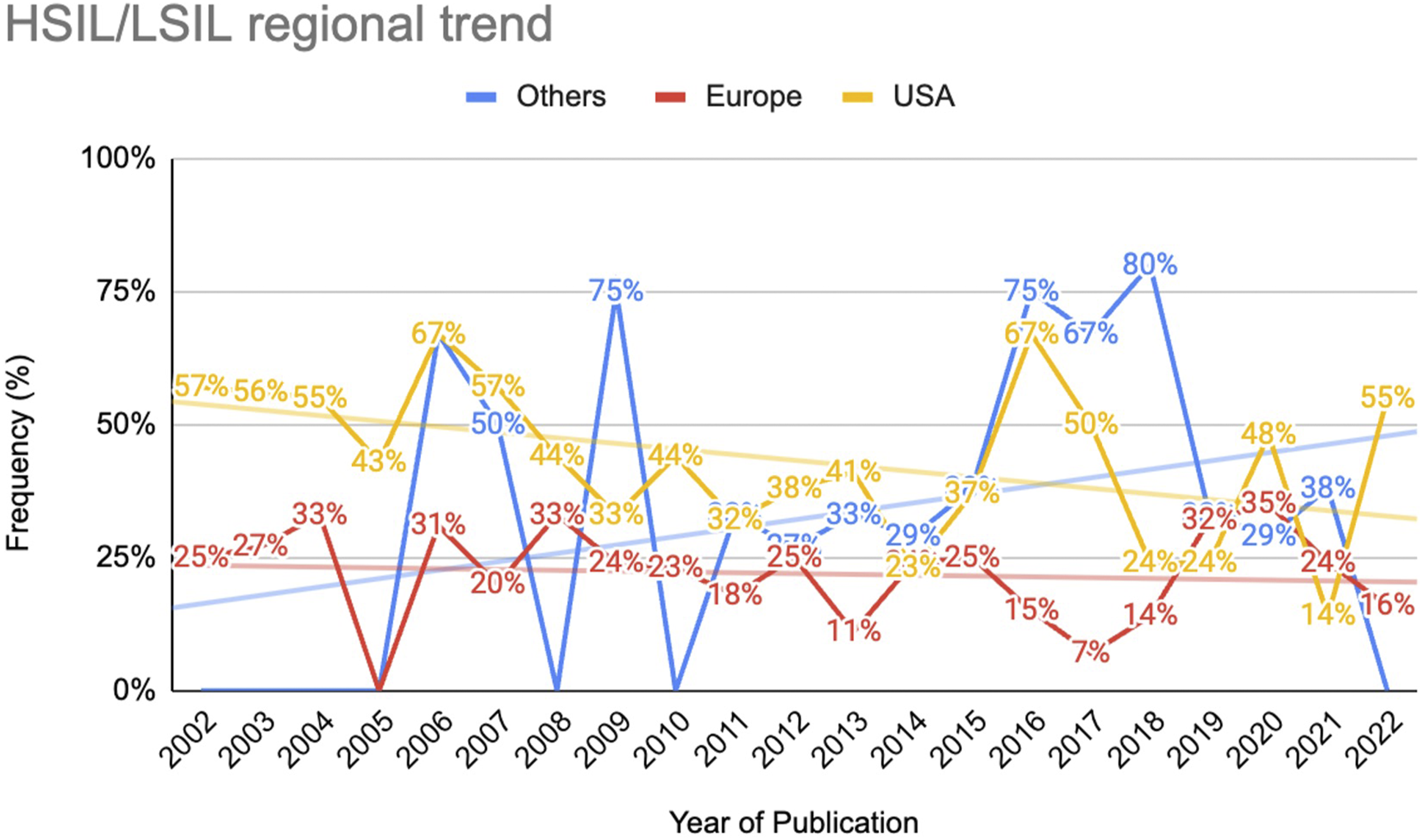
In the period between 2002 and 2012, the proportion of publications using HSIL/LSIL accounted for 35% (108 out of 311) of the total number of publications worldwide. Between 2013 and 2022, the proportion of HSIL/LSIL usage among the total publications was 29% (143 out of 486) (Figure 2). Trend analysis for HSIL/LSIL publication worldwide yielded a statistic of −82 and a Z-value of −2.47 (P = .01), suggesting a statistically significant downward trend in HSIL/LSIL publications globally. (Figure 3). Two-tiered nomenclature usage by year of publication globally. Two-tiered nomenclature usage by year of publication across different regions. Blue: Others; red: Europe; yellow: USA.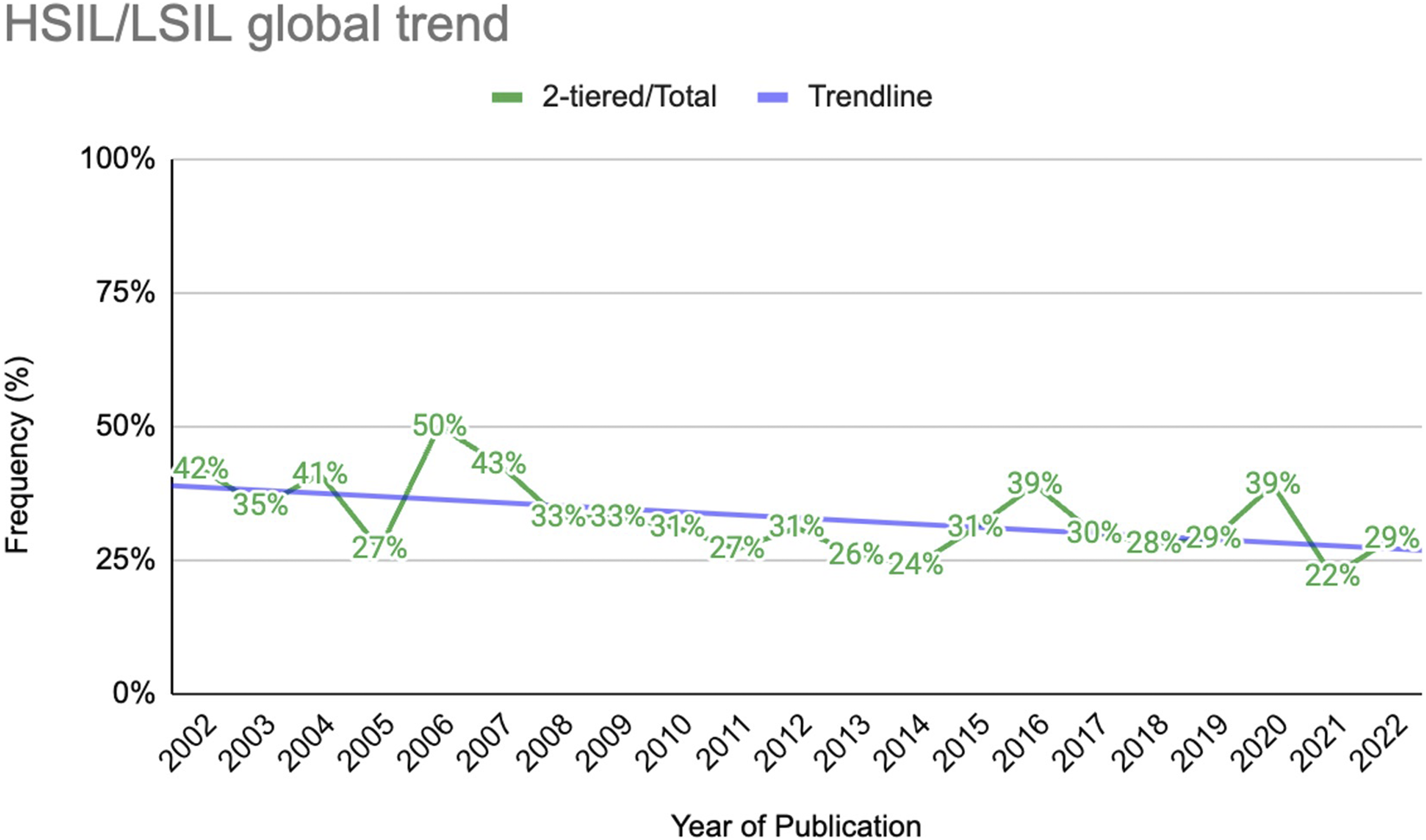
Regional Trend Analysis
In North America, 46% of the publications used the two-tiered nomenclature between 2002 and 2012. This rate decreased to 37% in the period between 2013 and 2022. The trend analysis test indicated a significant trend (statistic = −71; Z = −2.14; P = 0.03).
Publications in Europe exhibited a similar downward trend. Between 2002 and 2012, the publication frequency was 24% for the two-tiered nomenclature. Post-2013, the frequency of publications changed to 21%. Trend analysis for HSIL/LSIL publications indicated a non-significant downward trend (statistic = −26; Z = −.78, P = 0.43).
Given the small number of publications identified from Asia and Latin America in the periods of interest, the decision was made to group them together. Prior to 2013, the proportion of publications using the two-tiered nomenclature was 28%. Post-2013, the frequency in the use of the two-tiered nomenclature among the total publications increased to 40%. Trend analysis demonstrated no significant trend (statistic = 56; Z = 1.73; P = 0.08).
Discussion
The findings of our research indicate regional variance in adoption of the two-tiered nomenclature system, reflecting historical inconsistencies in pathology reports for HPV-associated lesions that contributed to uncertainty in clinical decision-making. 9 The outdated three-tiered system, introduced in the late 1960s, did not accommodate evolving insights into HPV’s oncogenic processes and anal cancer development. 6 For instance, it was observed that while some individuals with HPV infection retained oncogenic expression, others showed viral clearing from the host immune response. Meanwhile, others progressed into a latent or asymptomatic state. This knowledge indicated that the existing model of a lesion progressing towards higher degrees of –IN over time was too simplistic. 13 Furthermore, the challenge of pathological subjectivity in classifying between -IN2 and –IN3 categories led to poor reproducibility among pathologists. 14 The recognition of these issues prompted the shift to the two-tiered system for its biological relevance and improved interrater reliability.
The two-tiered system, which differentiates between HSIL and LSIL aids providers in clinical management decisions. 11 HSILs are considered premalignant lesions with a higher risk of progression to invasive carcinoma. The LAST project unified classification, supplemented by biomarkers, especially when p16 staining and HPV oncogene analysis were used for equivocal cases, 11 addresses the limitations of the previous nomenclature and improves diagnostic consistency.
Screening for HSILs is recommend through high-resolution anoscopy (HRA) as an effective option, particularly for high-risk individuals. This approach helps preventing anal cancer progression, although it may not reduce its incidence. Prior studies, including the ANALOGY trial 15 and research by Pineda and Welton, have suggested HRA’s effectiveness in detecting and managing HSILs, thereby playing a significant role in guiding treatment and surveillance decisions. 16
Despite the anticipated benefits, our research over the past two decades reveals a downward trend in the adoption of the two-tiered nomenclature, especially in North America. There was a 9% decrease in the frequency of publications using the two-tiered nomenclature, with trend analysis indicating a statistically significant downward trend over the years. The absence of significant trends in Europe, Asia and Latin America points to a global resistance to change, possibly due to entrenched diagnostic practices, lack of awareness, or cultural differences in medical practice. 11 Our literature review did not identify explicit recommendations against the adoption of the two-tiered nomenclature. This absence suggests that the issue may not be an explicit objection to the nomenclature itself but rather a combination of the factors mentioned above, which calls for educational and policy interventions.
The WG5 initiative aimed at widespread implementation of the LAST project recommendations, targeting a broad audience that includes health care professionals, regulatory agencies, public health organizations, educational entities, and coding organizations. Active dissemination efforts are in place, but challenges remain.
There were several limitations to this study. The search strategy was restricted to sorting titles using the predefined search terms. As a result, our study lacks a comprehensive exploration of the complete manuscript and the use of two-tiered nomenclature within them. Our strategy also excluded titles that combined the two-tiered system with AIN terminology, potentially overlooking manuscripts that used both systems interchangeably. Additionally, the study was limited to English-language publications, which may have impacted our ability to capture the full spectrum of the nomenclature use in the global scientific community. This limitation may result in a notably lower number of publications from Asia and Latin America, where English is not the predominant language, thereby affecting our analysis of the global distribution and discussion of the topic. Therefore, it is unclear if the trend of publications directly reflects the real-world usage of the two-tiered nomenclature.
In conclusion, our findings reflect suboptimal global adherence to the two-tiered system, despite multidisciplinary collaborative effort. Moving forward, further research is needed to identify the cause of poor adherence of these recommendations in order to implement strategies for unifying the terminology and integrating the recommendations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.