
Abstract
Background
The role of minimally invasive surgery (MIS) in the acute management of diverticulitis remains controversial. Using a national cohort, we examined the relationship between operative approaches with acute clinical and financial outcomes.
Methods
Adults undergoing emergent colectomy for diverticulitis were tabulated from the 2015-2020 American College of Surgeons National Surgical Quality Improvement Program. Regression models were developed to analyze the association between open and MIS approaches with major adverse events (MAE), as well as secondary endpoints. A subgroup analysis was conducted to compare outcomes between open and MIS requiring conversion to open (CTO).
Results
Of 9194 patients, 1580 (17.3%) underwent MIS colectomy. The proportion of MIS resection increased from 15.1% in 2015 to 19.1% in 2020 (nptrend<.001). Compared to Open, MIS patients were younger, equally likely to be female, had a lower proportion of patients with ASA class ≥3, and a higher BMI. Preoperatively, MIS patients were less frequently diagnosed with sepsis. Following adjustment with open as reference, MIS approach had reduced odds of MAE (AOR .56), ostomy creation (AOR .12), shorter postoperative length of stay (LOS; β −1.63), and a lower likelihood of nonhome discharge (AOR .45, all P < .001). Additionally, CTO was linked to decreased likelihood of MAE (AOR .78, P = .01), ostomy creation (AOR .02, P < .001), comparable LOS (β −.46, P = .41), and reduced odds of nonhome discharge (AOR .58, P < .001), relative to open.
Discussion
Compared to planned open colectomy, MIS resection was associated with improved clinical and financial outcomes, even in cases of CTO. Our findings suggest that whenever possible, MIS should be attempted first in emergent colectomy for diverticulitis. Nevertheless, future prospective studies are likely needed to further elucidate specific patient and clinical factors.
Key Takeaways
• Compared to planned open emergent colectomy for diverticulitis, minimally invasive (MIS) resection, even when converted to open, was linked to lower odds of major adverse events, ostomy creation, and reduced resource utilization. • Our results suggest that whenever feasible, MIS should be considered as the first operative approach attempted in the acute management of diverticulitis.
Introduction
Diverticulitis results in over 450,000 emergency department visits and 200,000 admissions annually, representing a significant burden on the United States health care system. 1 Among admitted patients, up to 20% require operative interventions. 2 Minimally invasive surgery (MIS) has been the preferred operative approach for elective colectomy due to its association with reduced complications, pain, and postoperative length of stay (LOS). 3 Yet, its role in the acute management of diverticulitis remains controversial. 3
Current guidelines from the European Association for Endoscopic Surgery (EAES) and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) only provide a weak recommendation for laparoscopic resection in emergent cases of diverticulitis in light of limited evidence. 4 Critics of the minimally invasive approach for emergent colectomy often cite safety and technical concerns. Specifically, MIS may pose an elevated risk of bowel injury given the distorted, inflamed surgical field. 3 Severe abdominal inflammation with hardened tissue may also make laparoscopic dissection impossible. Additionally, there is a higher perceived likelihood of abdominal bacteremia caused by pneumoperitoneum. 2 Although these concerns have not been corroborated by substantial evidence, they continue to limit the widespread adoption of MIS in the acute setting. 2 Conversely, certain retrospective studies5–8 and meta-analyses9,10 have presented results favoring MIS utilization in emergent colectomy. Compared to open colectomy, MIS resection was associated with lower odds of complications and shorter LOS.5–10 These studies, however, are limited to single institutions 5 or otherwise small cohorts.6,7,9,10 Moreover, few works have examined whether following unplanned conversion to open, planned MIS operations still confer improved outcomes relative to planned open procedures.5,8–10 Consequently, the role of minimally invasive surgery in the acute setting of diverticulitis remains under investigation.
Using a large national cohort, our study examined the relationship between operative approaches for emergent colectomy and select clinical and financial outcomes. We hypothesized that the MIS approach, even in cases of conversion to open, would be associated with lower odds of mortality and complication, as well as shorter LOS, relative to planned open resection.
Methods
This was a retrospective study using the 2015 to 2020 American College of Surgeons National Surgical Quality Improvement Program (NSQIP), Colectomy Targeted Participating User Files. National Surgical Quality Improvement Program and its participants are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. Due to the de-identified nature of the database, this study was deemed exempt from full review by the Institutional Review Board at the University of California, Los Angeles.
All adults (≥18 years) undergoing emergent, nonelective colectomy for diverticulitis were tabulated using relevant Current Procedural Terminology (CPT) codes (Supplemental Table 1). Patients with missing key data for age, sex, elective status, emergency status, American Society of Anesthesiologists (ASA) classification, or functional status were excluded (.8%; Figure 1). National Surgical Quality Improvement Program predefined variables were utilized to ascertain the operative approach and patient characteristics.
11
Patients undergoing planned open operations constituted the Open cohort, while those receiving laparoscopic or robotic resection comprised the MIS cohort. Ostomy creation and the extent of colonic resection (total vs partial) were identified using CPT codes (Supplemental Table 1). Study flowchart. Of the 50,463 adult hospitalizations for colectomy in the setting of diverticulitis identified in the 2015 to 2020 National Surgical Quality Improvement Program (NSQIP), 9194 patients were included in this study. Of these, 1580 (17.3%) received minimally invasive (MIS) resection.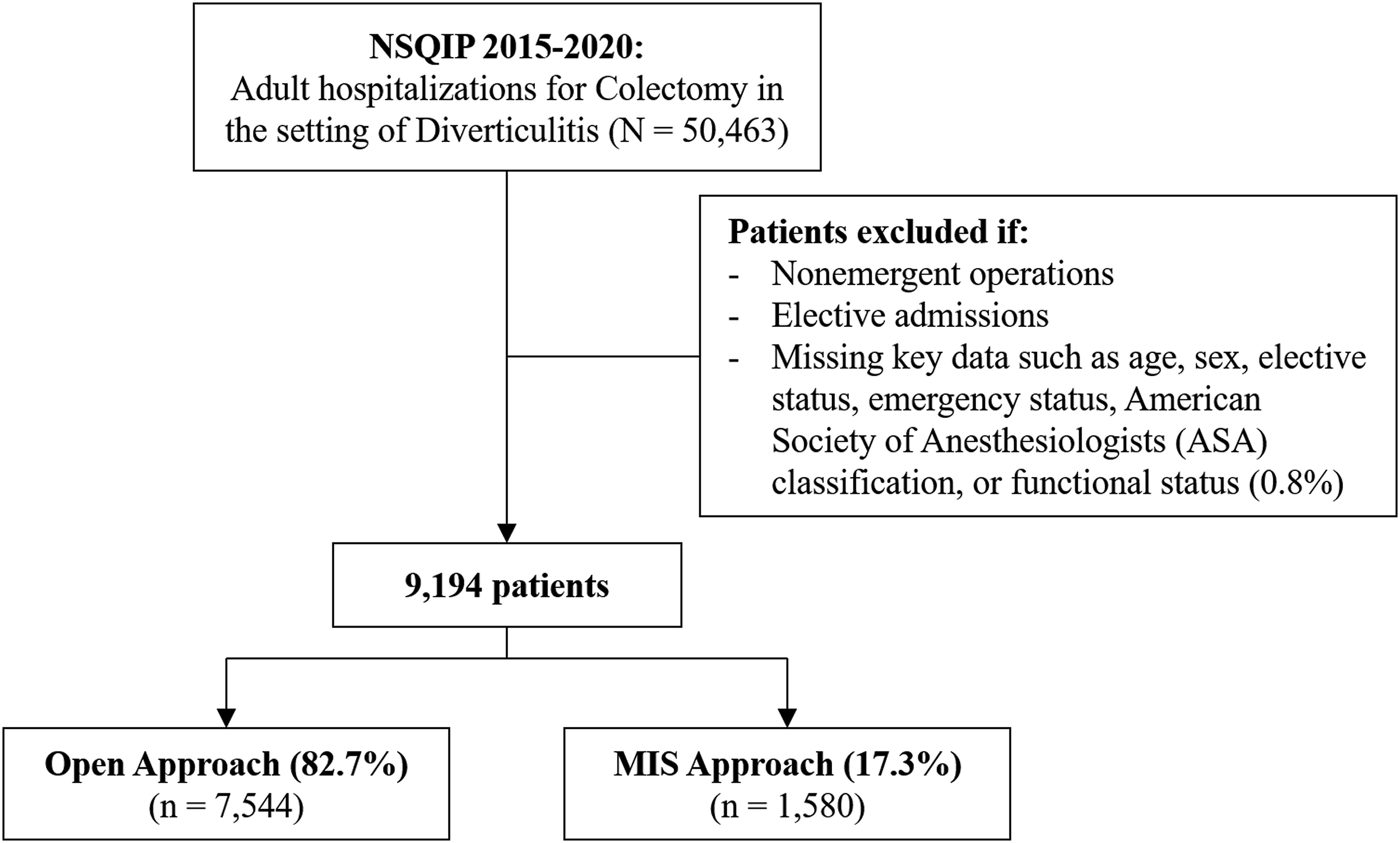
The primary outcome was major adverse events (MAE), defined as a composite of 30-day mortality and perioperative complications. Secondary endpoints included 30-day mortality, perioperative complications, operative time, ostomy creation, LOS, nonhome discharge, and 30-day readmission. Complications of interest consisted of cardiac complications (cardiac arrest and myocardial infarction), pneumonia, superficial and deep wound infections, organ space infection, urinary tract infection, wound dehiscence, sepsis, septic shock, renal complications (acute renal insufficiency and failure), reoperation, prolonged ventilation (>48 hours), reintubation, stroke, thromboembolic events (pulmonary embolism and deep vein thrombosis), transfusion, anastomotic leak, and postoperative ileus.
Categorical variables are reported as percentages (%), while continuous variables are presented as medians with interquartile range (IQR). The Pearson’s χ2 and the Mann-Whitney U tests were utilized to analyze the significance of intergroup differences, as appropriate. The significance of temporal trends was assessed using Cuzick’s nonparametric test (nptrend). 12 Entropy balancing was used to account for differences in characteristics between Open and MIS. This method adjusts the distribution of covariates between cohorts by assigning each patient a specific weighting value. Since it does not rely on matching propensity scores, entropy balancing retains the entire sample for analysis. 13 Covariate selection for the entropy balancing model was guided by elastic net regularization, a technique which uses the penalized least-squares methodology to reduce overfitting. 14 Following entropy balancing, logistic and linear regression models were fitted to examine the relationship between operative approaches and the outcomes of interest. A subgroup analysis was also performed to compare outcomes between Open and MIS operations requiring unplanned conversion to open (CTO). Regression outputs are reported as adjusted odds ratios (AORs) or as beta coefficients (β) with 95% confidence intervals (CIs), as appropriate. α was set at .05 for statistical significance. All statistical analyses were performed using Stata 16.0 (StataCorp, College Station, TX).
Results
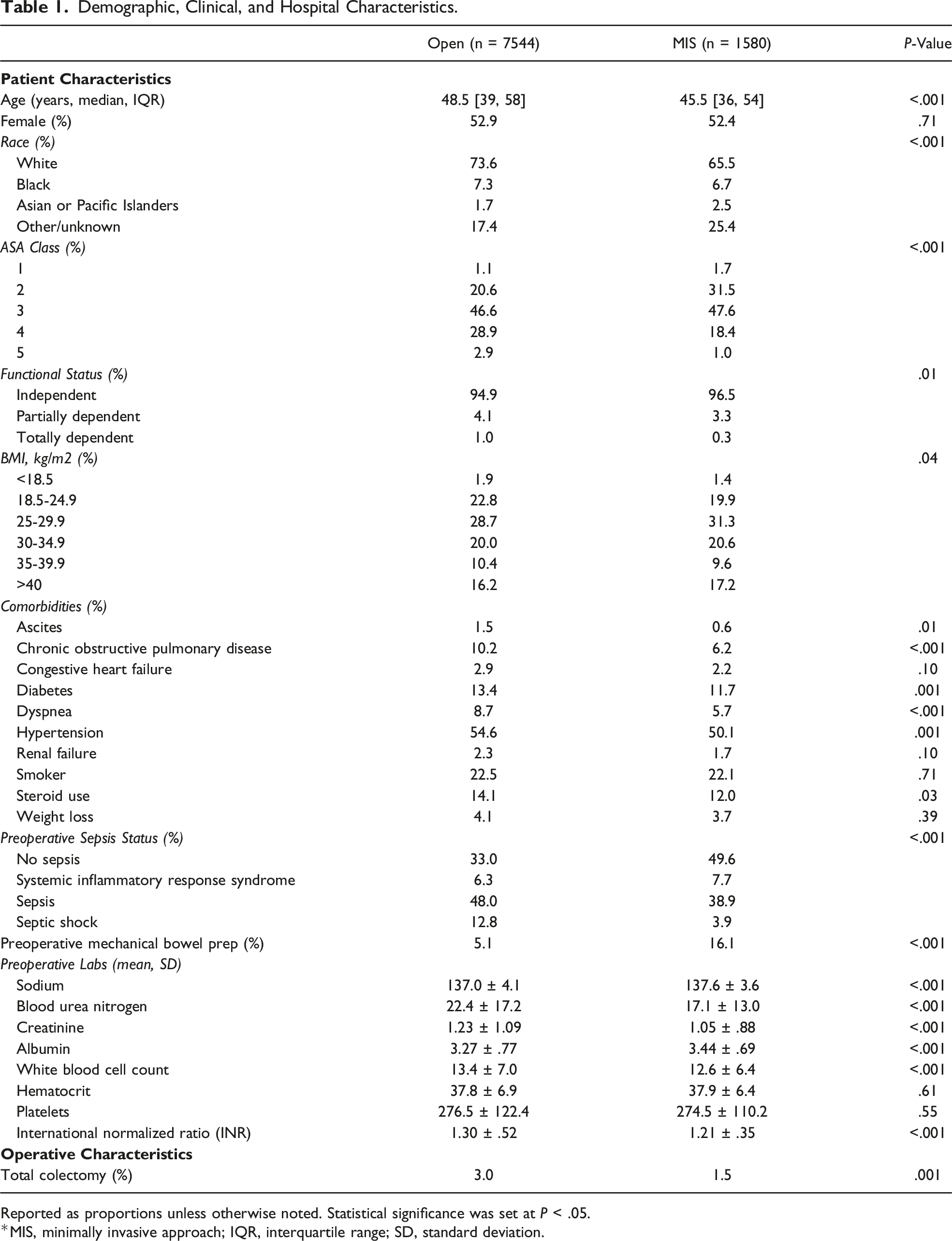
Of 9194 patients, 1580 (17.3%) constituted the MIS cohort. The proportion of minimally invasive, emergent colectomies for diverticulitis increased from 15.1% in 2015 to 19.1% in 2020 (nptrend<.001; Figure 2). Patient and operative characteristics are shown in Table 1. Compared to Open, MIS patients were younger (45.5 [36, 54] vs 48.5 [39, 58] years, P < .001), equally likely to be female (52.9 vs 52.4%, P = .71), had a lower severity of systemic illness (ASA class ≥3, 67.0 vs 78.4%, P < .001), and a higher BMI (BMI ≥25, 78.7 vs 75.3%, P = .04). Preoperatively, MIS patients were less frequently diagnosed with sepsis (50.5 vs 67.1%) and more often received mechanical bowel prep (16.1 vs 5.1%, all P < .001). Minimally invasive approaches were less likely to result in total colectomy (1.5 vs 3.0%, P = .001). Annual trends in the volumes of open and minimally invasive (MIS) colectomy, 2016-2020. The proportion of MIS procedures significantly increased over the study period, nptrend <.001. Demographic, Clinical, and Hospital Characteristics. Reported as proportions unless otherwise noted. Statistical significance was set at P < .05. *MIS, minimally invasive approach; IQR, interquartile range; SD, standard deviation.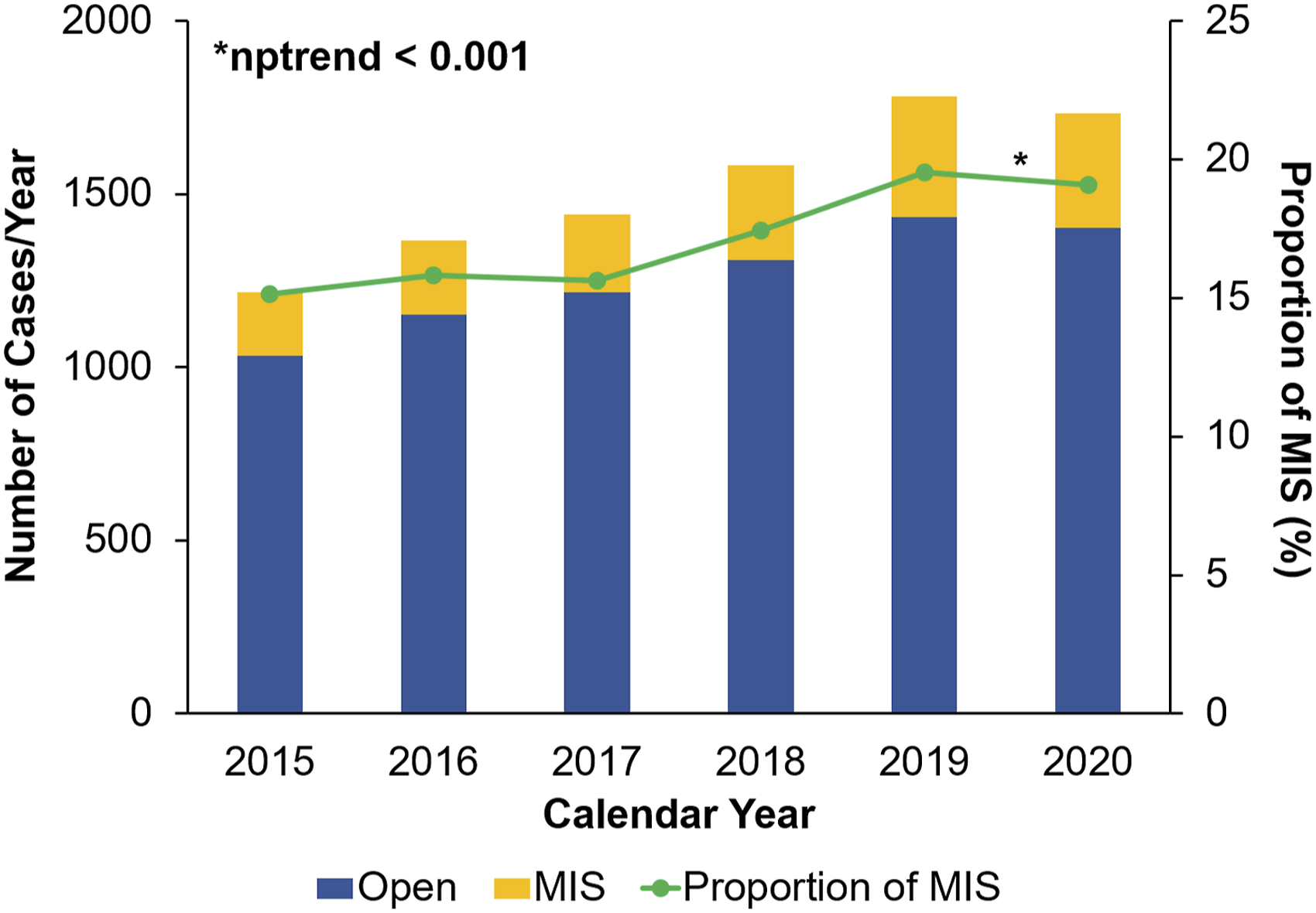
Unadjusted Outcomes of Patients Undergoing Planned Open Versus Minimally Invasive (MIS) Colectomy for Emergent Diverticulitis.
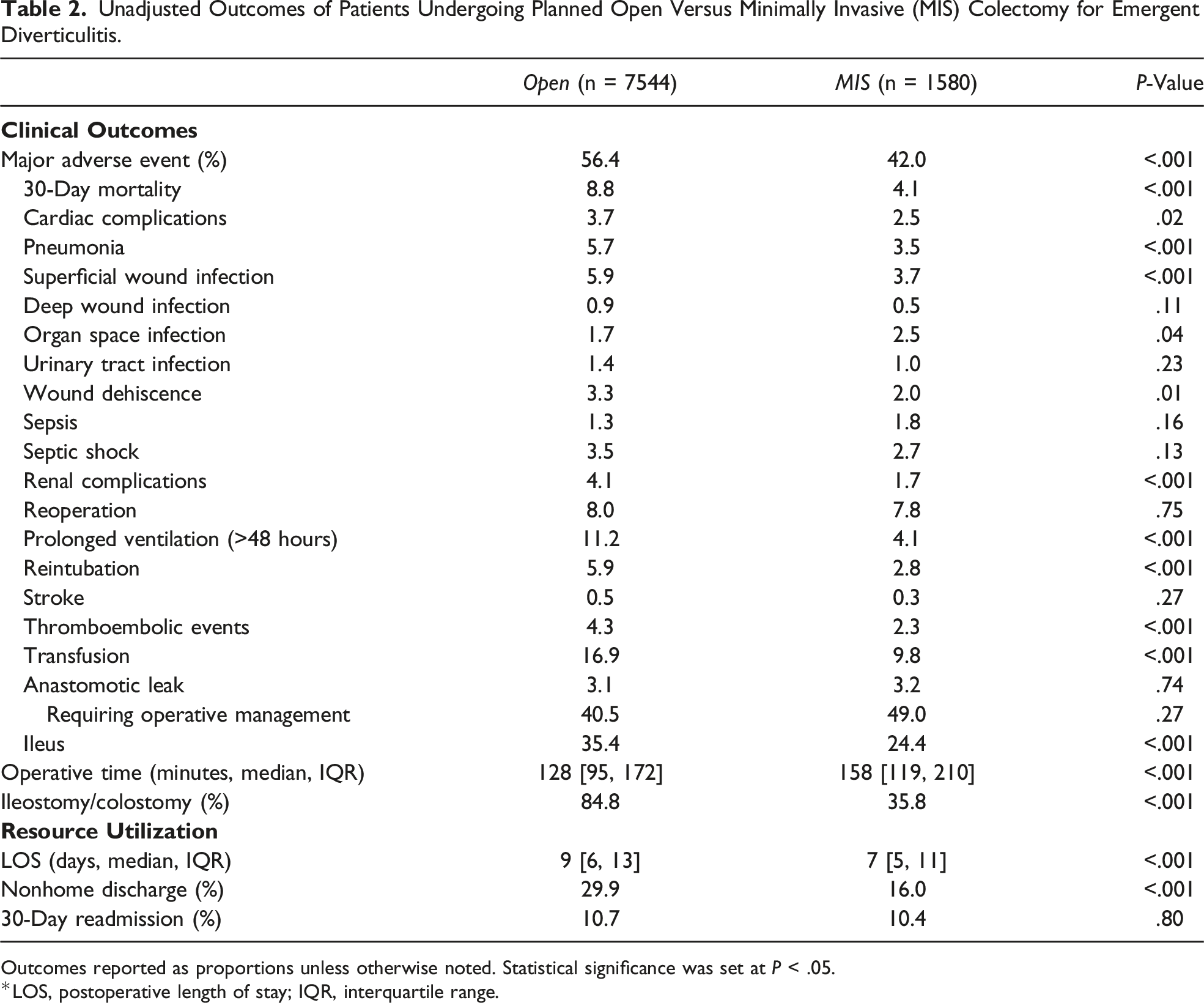
Outcomes reported as proportions unless otherwise noted. Statistical significance was set at P < .05.
*LOS, postoperative length of stay; IQR, interquartile range.
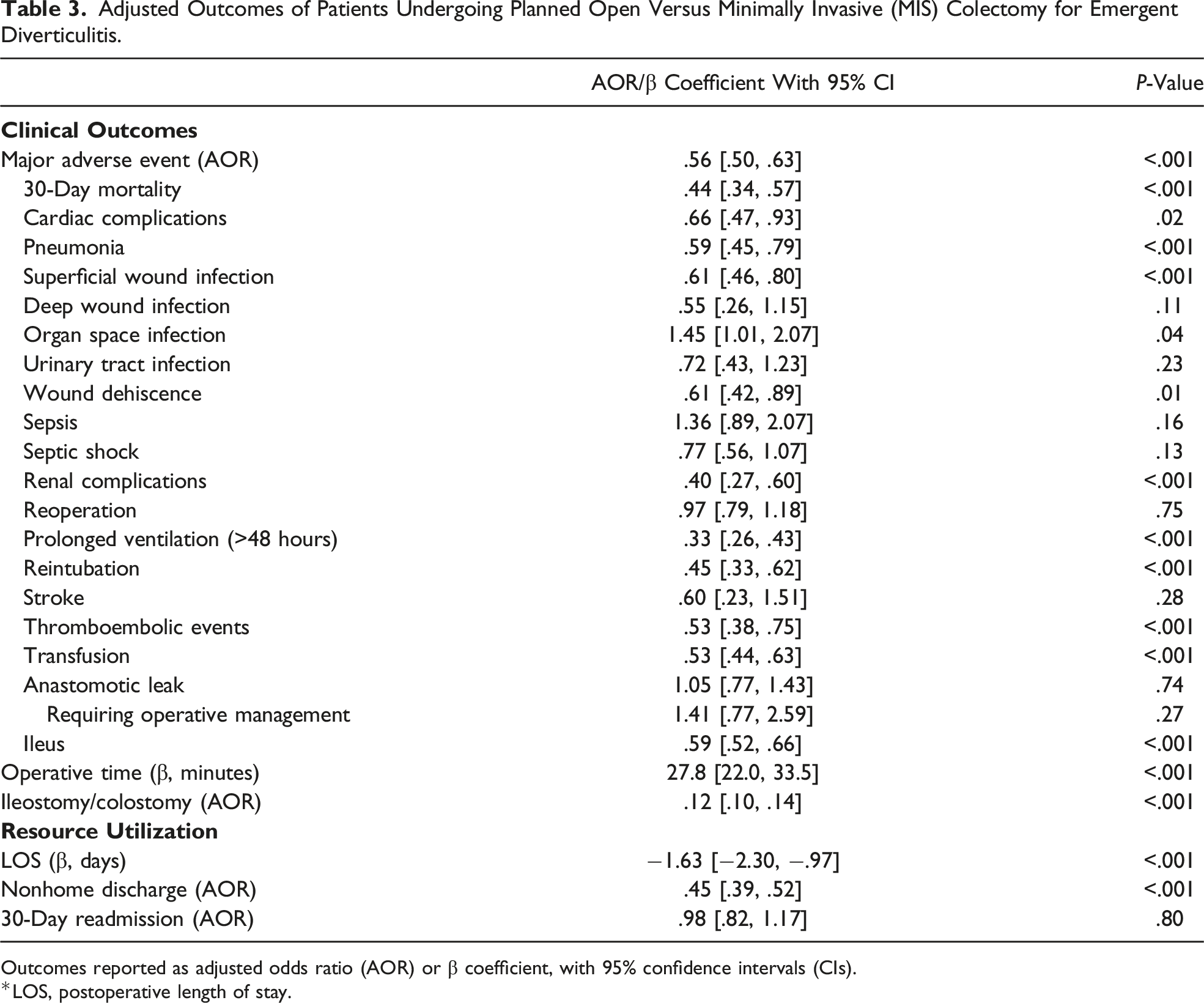
A logistic model was fitted for MAE and yielded an adequate discrimination (C-statistic = .73). Regression outputs comparing outcomes between open and MIS approaches are shown in Figure 3 and Table 3. Following risk adjustment with planned open colectomy as the reference, MIS was associated with decreased odds of MAE (AOR .56, 95% CI [.50, .63]; Table 3). In particular, it was linked to reduced likelihood of 30-day mortality, cardiac complications, pneumonia, superficial wound infection, wound dehiscence, renal complications, prolonged ventilation, reintubation, thromboembolic events, transfusion, and ileus (Figure 3). Compared to open, MIS had higher odds of organ space infection (AOR 1.45, 95% CI [1.01, 2.07]) and longer operations (β 27.8 minutes, 95% CI [22.0, 33.5]; Table 3). However, MIS was associated with lower odds of ostomy creation (AOR .12, 95% CI [.10, .14]) and shorter LOS (β −1.63 days, 95% CI [−2.30, −.97]). Furthermore, MIS yielded a lower likelihood of nonhome discharge and similar odds of 30-day readmission (Table 3). Association of minimally invasive emergent colectomy (MIS) with select outcomes of interest. Compared to planned open resection, MIS was associated with lower odds of major adverse events, ostomy creation, and nonhome discharge. ∗Indicates statistical significance, P < .05. Error bars represent 95% CIs. Adjusted Outcomes of Patients Undergoing Planned Open Versus Minimally Invasive (MIS) Colectomy for Emergent Diverticulitis. Outcomes reported as adjusted odds ratio (AOR) or β coefficient, with 95% confidence intervals (CIs). *LOS, postoperative length of stay.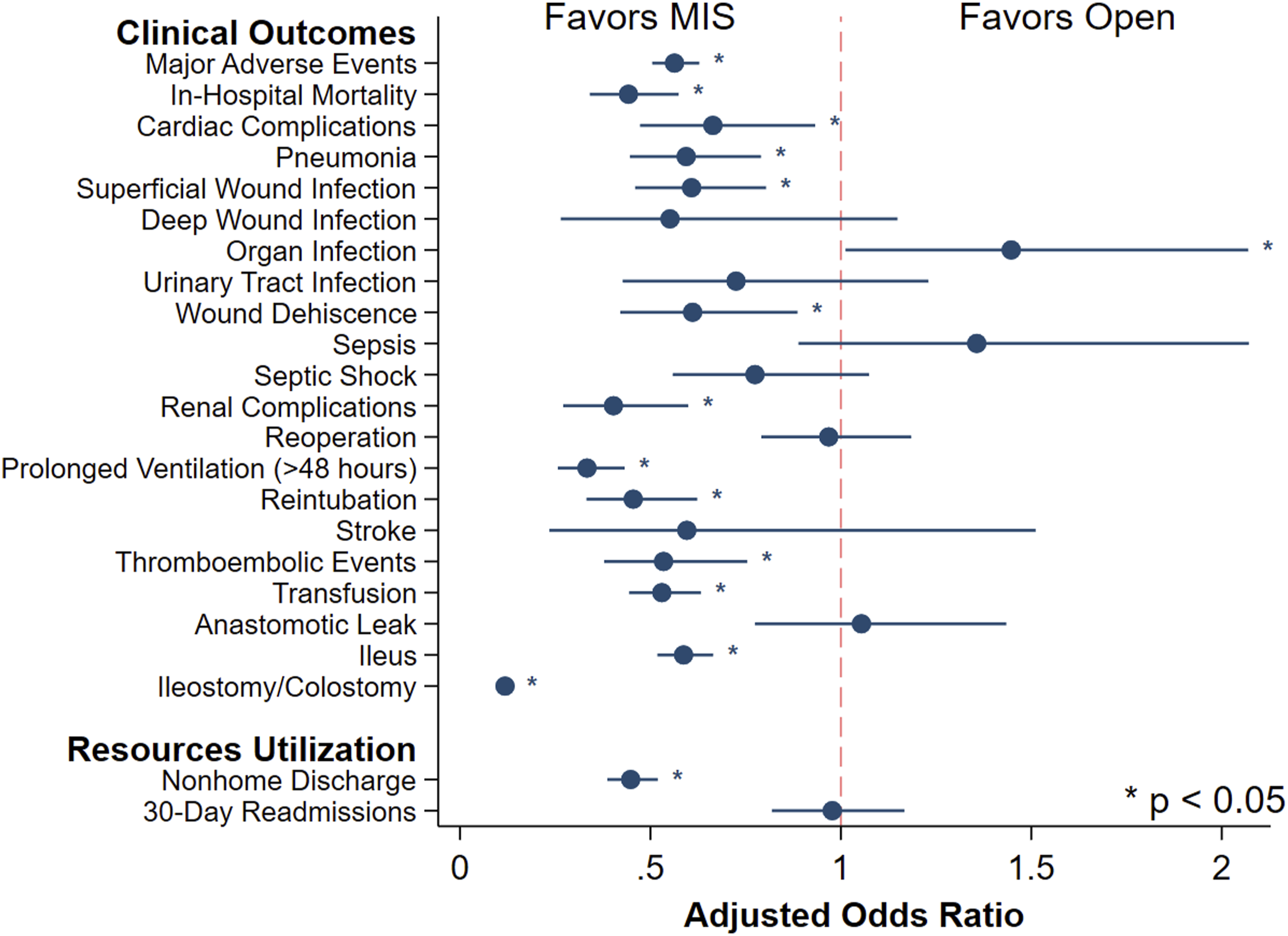
Subgroup Analysis: Open vs CTO
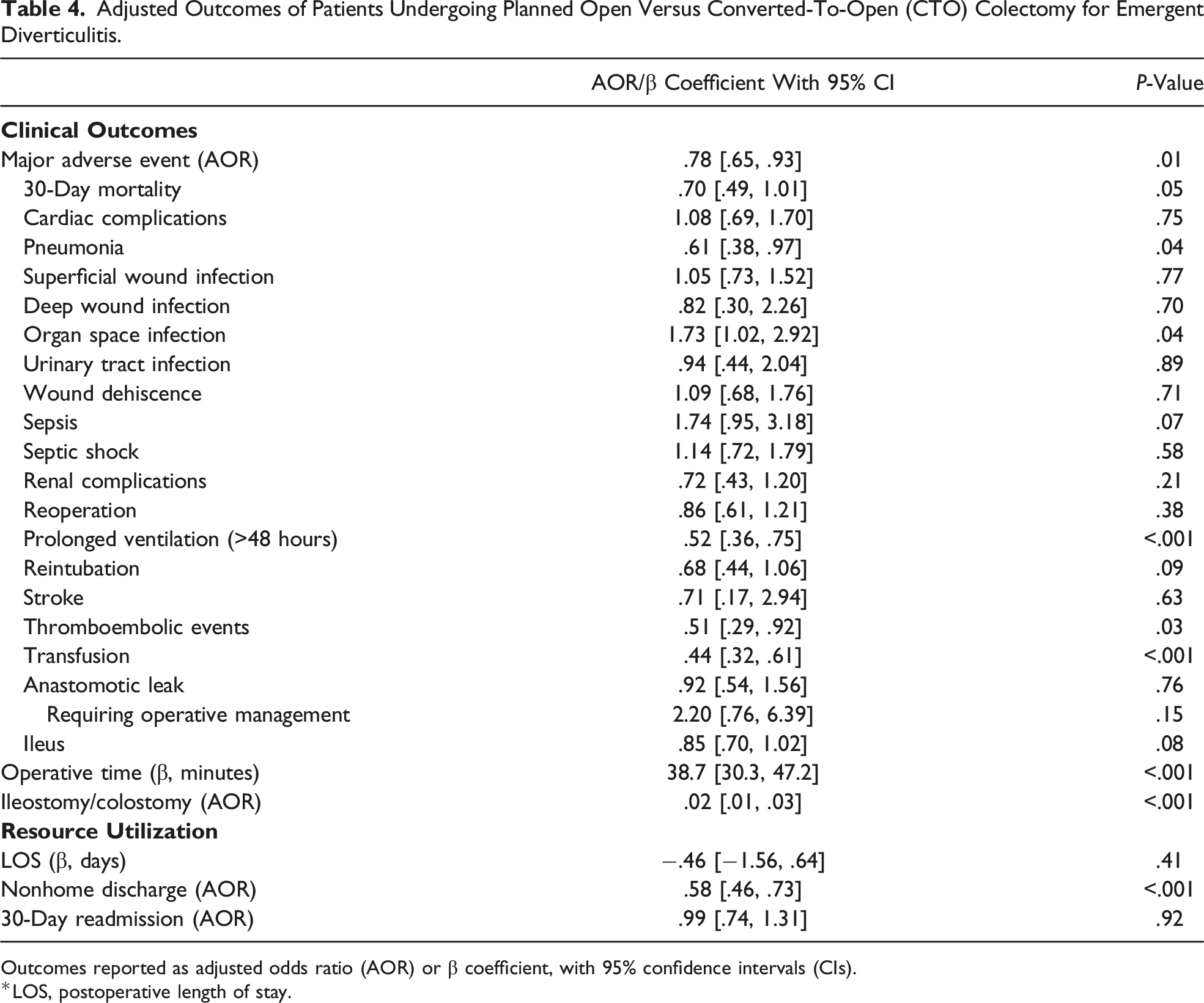
Adjusted Outcomes of Patients Undergoing Planned Open Versus Converted-To-Open (CTO) Colectomy for Emergent Diverticulitis.
Outcomes reported as adjusted odds ratio (AOR) or β coefficient, with 95% confidence intervals (CIs).
*LOS, postoperative length of stay.
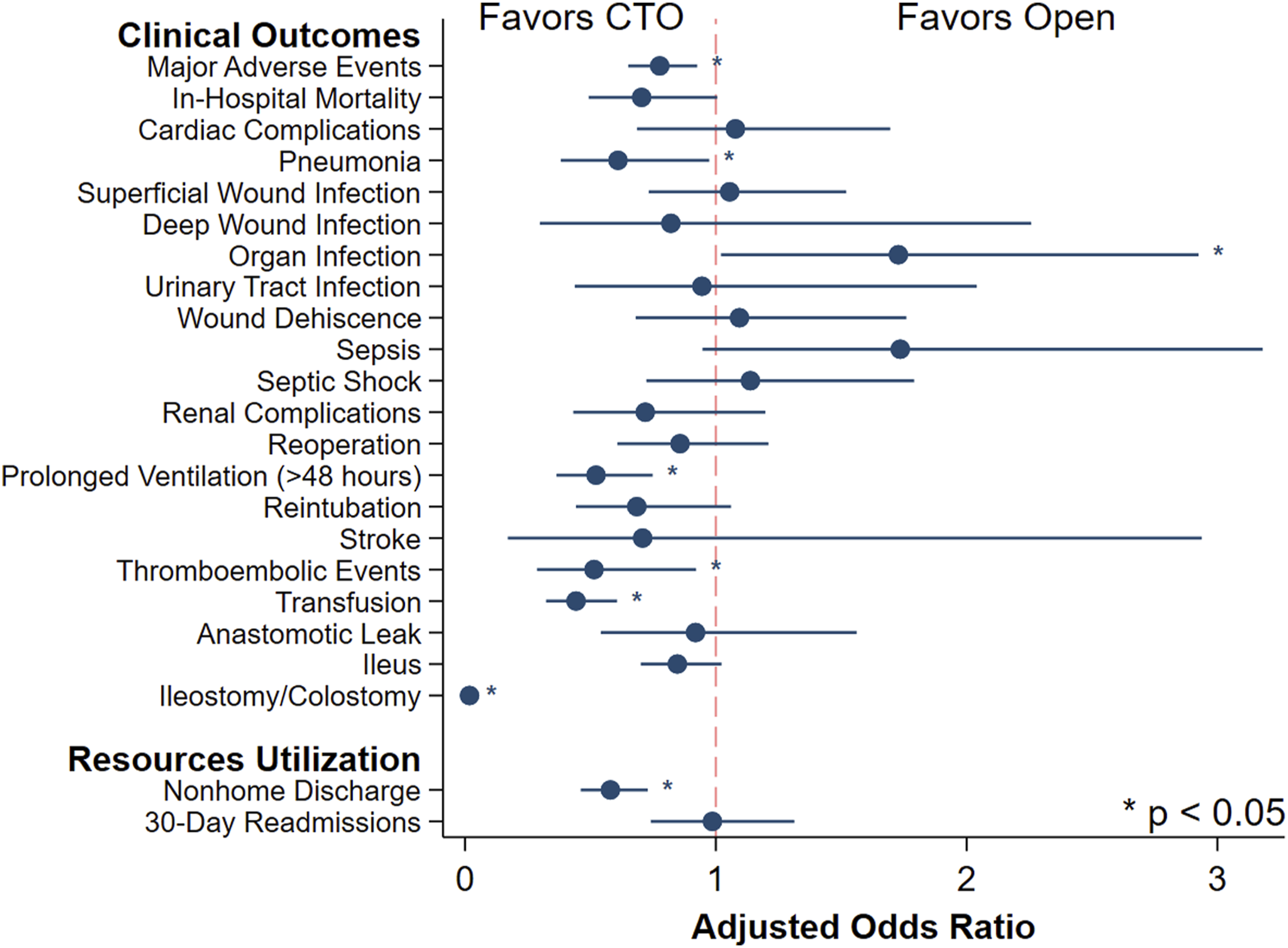
Association of converted-to-open emergent colectomy (CTO) with select outcomes of interest. Compared to planned open resection, CTO was associated with lower odds of major adverse events, ostomy creation, and nonhome discharge. ∗Indicates statistical significance, P < .05. Error bars represent 95% CIs.
Discussion
While MIS has become the preferred approach in elective colectomy for diverticulitis, its role in the acute setting remains controversial. 3 Using a large national database, we examined contemporary trends in MIS utilization in emergent colectomy for diverticulitis. We further assessed the relationship between planned open and MIS operative approaches with acute clinical outcomes. We found the proportion of emergent colectomy that were MIS to have increased throughout the study period, accounting for approximately 20% of the cases in 2020. Following risk adjustment, both MIS and CTO were associated with lower odds of MAE, ostomy creation, and reduced resource utilization, compared to planned open. However, they were linked to longer operations and a higher likelihood of organ space infection. With potential implications for clinical decision-making, our findings warrant further discussion.
Minimally invasive surgery approaches have been increasingly utilized for emergent colectomy for acute diverticulitis. 7 Possible contributors to this trend include the demonstrated benefits of MIS in elective resection and the increase in familiarity of surgeons with the approach. The Sigma trial showed that for elective colectomy, laparoscopy was linked to reduced major complication rates, pain, and LOS, relative to open. 2 Retrospective studies5–8 and meta-analyses9,10 have similarly noted MIS to be associated with improved outcomes for emergent colectomy. While future prospective studies are needed to examine this relationship, their designs will need to acknowledge the ethical concerns regarding the ability of patients to properly consent in acute settings. 15 Additionally, the rise in MIS utilization for emergent colectomy may be attributed to the growing experience of surgeons with this technique. As surgeons perform more MIS elective resections, they may be more willing to adapt the skills learned from these cases to emergent operations. 16 Nevertheless, steep learning curves and concerns over the safety of MIS procedures continue to limit the adoption of the approach in acute settings.2,3,16,17 The learning curve for MIS colectomy in diverticulitis is estimated at 70-100 cases. 17 However, the use of hand-assisted laparoscopic surgeries may aid in the transition from open to MIS approach.16,17 The minimally invasive approach is also believed to be linked to increased risks of bowel injury due to distorted anatomy 3 and abdominal bacteremia caused by pneumoperitoneum. 2 Nonetheless, there is no substantial evidence to support these hypothetical relationships. 2 Our study also helps suggest that no such association exists by demonstrating comparable odds of sepsis and septic shock between open and MIS. Given the increasing utilization of MIS in emergent colectomy, ongoing examination of clinical and financial outcomes associated with these operations remains necessary.
Our observation that MIS was associated with lower short-term mortality is a novel finding. Previous studies found no relationship between surgical approaches and perioperative deaths.5–10 Nevertheless, they were limited by their institutional designs, 5 small cohorts,6,7,9,10 or having a remarkably low mortality. 8 The observed association between MIS and lower odds of 30-day mortality in our study can be possibly attributed to the less complicated postoperative course these patients experienced. In fact, the link between the minimally invasive approach and reduced risks of complications and shorter LOS is well-established.5–10 Factors contributing to this relationship include the abilities of MIS to exert a lower level of surgical stress 7 and better preserve the integrity of the abdominal wall. 18
Additionally, we found that compared to planned open approach, CTO was associated with decreased odds of complications. This is a novel finding in the context of emergent colectomy for diverticulitis. Using 2012-2017 NSQIP, Moghadamyeghaneh, Lee, and their respective colleagues noted CTO to be associated with similar odds of morbidity, relative to planned open.6,7 Yet, their analyses were limited to CTO cohorts with fewer than 180 patients, approximately a third of our CTO cohort. Possible contributors to the association of CTO with improved clinical outcomes in our study include patient selection and progress accomplished prior to conversion, such as mobilization of the bowel. 19 It is difficult to analyze this relationship further without additional information, such as reasons and timing of conversions. Thus, future examination of factors associated with conversion-to-open and outcomes following these procedures remains relevant. Nevertheless, our results help support the safety profile of MIS and its role as the first operative approach attempted for emergent colectomy.
Interestingly, we noted that compared to planned open, MIS and CTO were linked to higher odds of organ space infection. One possible explanation for this observation is the inadequate washout of purulent material in interloop spaces. These spaces could be poorly visualized during emergent cases due to the underlying dilated, inflamed bowel. This is contrary to a previous hypothesis that MIS offers improved quality of peritoneal lavage in emergent colectomy for perforated diverticulitis, relative to open. 18 Our results suggest that a more thorough approach to washout is warranted when the minimally invasive approach is utilized.
Finally, it is important to recognize the association of MIS with remarkably lower odds of requiring an ileostomy or colostomy, with planned open as the reference. This finding is consistent with a previous study by Rea et al. 18 The reduction in the likelihood of ostomy creation persisted even if the case was converted to an open procedure, which, to our knowledge, is a novel finding. Ileostomy and colostomy have significant financial and clinical burdens on patients. Their monthly supplies cost, on average, between $100 and $300. 20 Additionally, up to 80% of patients with ostomies experience stoma-related complications, such as peristomal skin breakdown. 20 It is possible that the link between MIS and reduced odds of ostomy creation reflected the strong preferences of the operating surgeons to avoid the aforementioned burdens. The association also suggests that since their patients are more likely to be ostomy-free, MIS may offer improved quality of life, compared to the open approach. This relationship should be examined in future works.
This study has several limitations inherent to its retrospective nature and utilization of an administrative database. First, NSQIP does not include certain critical clinical information, such as the modified Hinchey classification, history of acute attacks of diverticulitis, location of resections, reasons and timing of conversions to open, and several individual factors that may influence clinical decision-making and procedural outcomes. For example, surgeons are less likely to initiate an MIS operation on an unstable patient with significant comorbidities, leading to a potential selection bias within our study population. Additionally, NSQIP does not document the operative volumes for each surgeon or whether the surgeon obtained subspecialty training in colorectal and/or minimally invasive surgery. Thus, we could not study the impact of additional experience and specialization on outcomes following these operations. Finally, we cannot determine any causal relationships due to the observational nature of our study design. Despite these limitations, we employed robust statistical methodology and a large patient sample to examine contemporary trends and outcomes in open vs MIS emergent colectomy for diverticulitis.
In conclusion, our study demonstrated increasing MIS adoption in emergent colectomy for diverticulitis. Compared to planned open resection, MIS, even if converted to open, was linked to longer operations but lower odds of major adverse events, ostomy creation, and reduced resource utilization. These findings suggest that, whenever possible, minimally invasive surgery should be considered as the first operative approach attempted in emergent colectomy for diverticulitis. Nevertheless, future prospective studies that can incorporate more granular patient and clinical factors should be pursued to optimize surgical decision-making.
Supplemental Material
Supplemental Material - Open Versus Minimally Invasive Emergent Colectomy for Diverticulitis
Supplemental Material for Open Versus Minimally Invasive Emergent Colectomy for Diverticulitis by Nguyen K. Le MS1, Nam Yong Cho BS, Saad Mallick MD, Nikhil Chervu MD MS, Shineui Kim BA, Sara Sakowitz MS MPH, Peyman Benharash MD MS, and Hanjoo Lee MD in The American Surgeon™.
Footnotes
Author Notes
This manuscript was presented at the 2024 Annual Conference of the Southern California Chapter, American College of Surgeons, Santa Barbara, CA, January 19-21, 2024.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.