
Abstract
Background
For patients with ductal carcinoma in situ (DCIS) undergoing breast conservation surgery (BCS), guidelines advise a margin width of at least 2 mm, with studies demonstrating decreased recurrence risk compared to narrower margins. However, limited data exist establishing if this margin is appropriate in mastectomies, and specifically for nipple-sparing mastectomy (NSM). Consequently, we evaluated the margins of DCIS patients undergoing NSM and resulting oncologic outcomes.
Methods
A single-institution retrospective review was performed in patients with DCIS or DCIS with microinvasion (DCIS + MI) undergoing NSM from April 2010 to December 2021. Patient and tumor characteristics, margin status, treatment, and outcomes information were collected. The association between margins and local-regional (LRR) and distant recurrence (DR) were examined.
Results
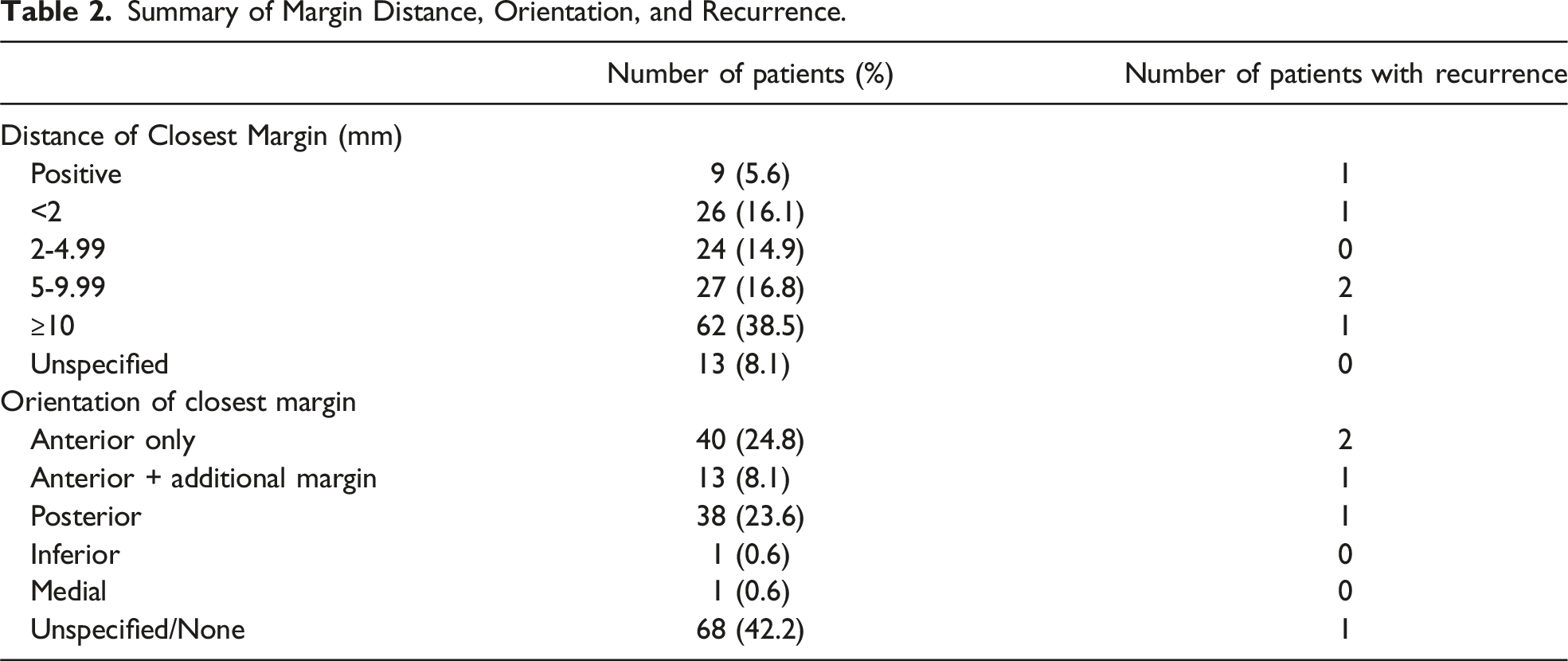
161 patients were included, comprising 284 NSM (164 therapeutic, 120 prophylactic). 153 patients had DCIS and 8 had DCIS + MI. Most patients had hormone sensitive, 123 (76.4%), and nuclear grade 2, 72 (44.7%), disease. In total, 35 (21.7%) patients had positive or <2 mm margins. Of these, 21 (60%) involved the anterior margin. At a median follow-up of 45 months (range 0-151), 2.5% (n = 4) had a LRR and .6% (n = 1) had a DR. Of patients with a recurrence, only 2 had positive or <2 mm margins, 1 had received endocrine therapy, and none received adjuvant radiation.
Discussion
No specific margin status was found to correlate with recurrence for patients with DCIS or DCIS + MI undergoing NSM, with an altogether low recurrence risk. Overall, this suggests that recommended DCIS margins in BCS doesn’t necessarily apply in NSM, where margins of <2 mm may be acceptable.
Keywords
Key Takeaways
• Margins of <2 mm may be acceptable for patients with DCIS undergoing NSM. • No specific margin status was associated with recurrence risk in patients with DCIS or DCIS + MI undergoing NSM. • Nipple-sparing mastectomy can be safely performed with low rates of recurrence in high-volume, community hospitals.
Introduction
Adequate margins for ductal carcinoma in situ (DCIS) or DCIS with microinvasion (DCIS + MI) in patients undergoing breast conservation surgery are generally considered to be at least 2 mm and is recommended by multiple national societies, including the National Comprehensive Cancer Network, Society of Surgical Oncology, American Society of Radiation Oncology, and the American Society of Clinical Oncology.1,2 This stems from a meta-analysis of observational studies demonstrating that margins of at least 2 mm are associated with a decreased risk of local tumor recurrence compared to more narrow margins, with an odds ratio of .51 for 2 mm vs > 0 mm or 1 mm. 2 Conversely, there is no consensus or specific acceptable margin width described for patients with DCIS or DCIS + MI undergoing mastectomy.
A meta-analysis examining breast cancer margin status and recurrence risk following skin-sparing mastectomy (SSM) and simple mastectomy (SM) including over 30,000 patients demonstrated a 2 to 3-fold increased risk of local recurrence (LR) for close or positive margins compared to negative margins. 3 However, this was not specific to patients with DCIS or DCIS + MI and did not include patients undergoing nipple-sparing mastectomy (NSM). A more recent study specifically examining DCIS margins for any type of mastectomy found no association between margin width and recurrence rate. However, of the 292 mastectomies included, only 15 (5.1%) underwent nipple-sparing mastectomy (NSM). 4
With increased breast cancer screening
Methods
Institutional Review Board approval was acquired. A retrospective chart review was performed for women undergoing NSM for a breast cancer diagnosis within our hospital system from April 2010 to December 2021. Patients were included if they had a diagnosis of DCIS or DCIS + MI and underwent upfront surgery and excluded if they did not have a diagnosis of DCIS and had invasive disease >1 mm. Patient and tumor characteristics were collected, including age, BMI, menopausal status, detailed margin status, extent of DCIS, nuclear grade, and tumor markers. Subsequent management including adjuvant therapies received and outcomes data were also evaluated. Primary outcomes included the association between margin status and local-regional recurrence (LRR) as well as distant recurrence (DR). Secondary outcomes included association of specific tumor characteristics such as estrogen receptor (ER) status or nuclear grade with recurrence risk.
Positive margins were defined as any tumor on ink and close margins as <2 mm from the inked margin. Tumor was defined as either DCIS or DCIS + MI. The length of follow-up was determined by the last physician to document a breast exam or most recent breast imaging. LRR was defined as recurrent breast cancer within the mastectomy skin, chest wall, or regional nodal basins and DR as distant metastatic breast cancer. Descriptive data was summarized by frequency and percentages. Univariate analysis and subgroup analysis were used to evaluate the association of margin status, tumor, and adjuvant therapy characteristics and recurrence. Chi-square analyses were performed at a significance level of .05 using Microsoft Excel (2021).
Results
Patient, Malignancy, and Treatment Characteristics in Patients Undergoing NSM for DCIS or DCIS + MI.
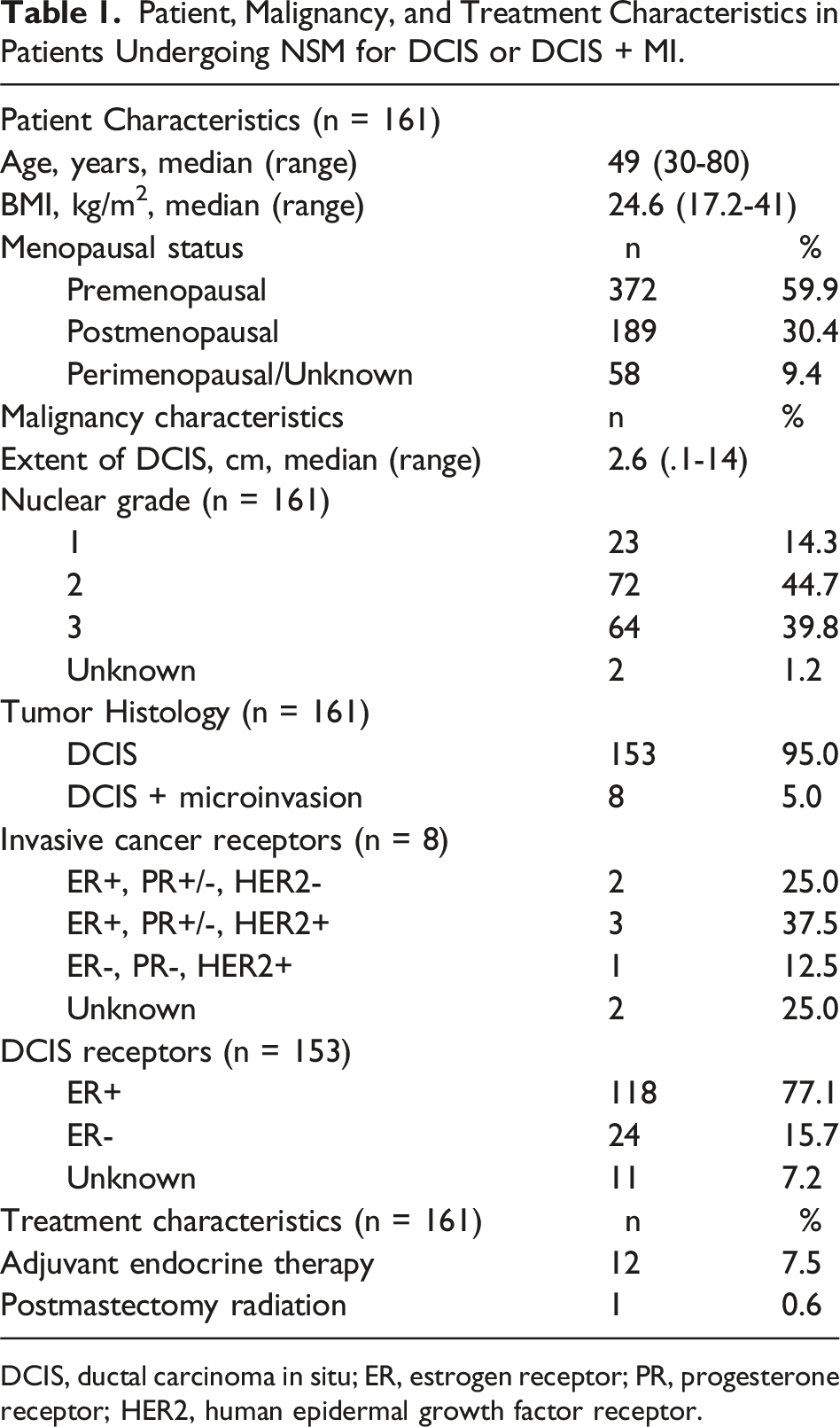
DCIS, ductal carcinoma in situ; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor.
Summary of Margin Distance, Orientation, and Recurrence.
Of the 161 patients, 5 (3.1%) experienced recurrent disease. This included 4 (2.5%) with LRR, comprising 3 with invasive, ER + disease, and 1 with DCIS, ER+. One patient (.6%) experienced a DR to the lung which was also ER+. One recurrence involved the NAC and had a negative nipple margin at the time of initial surgery. None of these patients received adjuvant radiation, and only 1 received adjuvant endocrine therapy. The median time to recurrence was 43 months (range 25-88) with a median follow-up of 68 months (range 56-88). The overall follow-up for the entire cohort was 45 months (range 0-151).
Clinicopathologic Characteristics of Patients With Recurrent Disease.
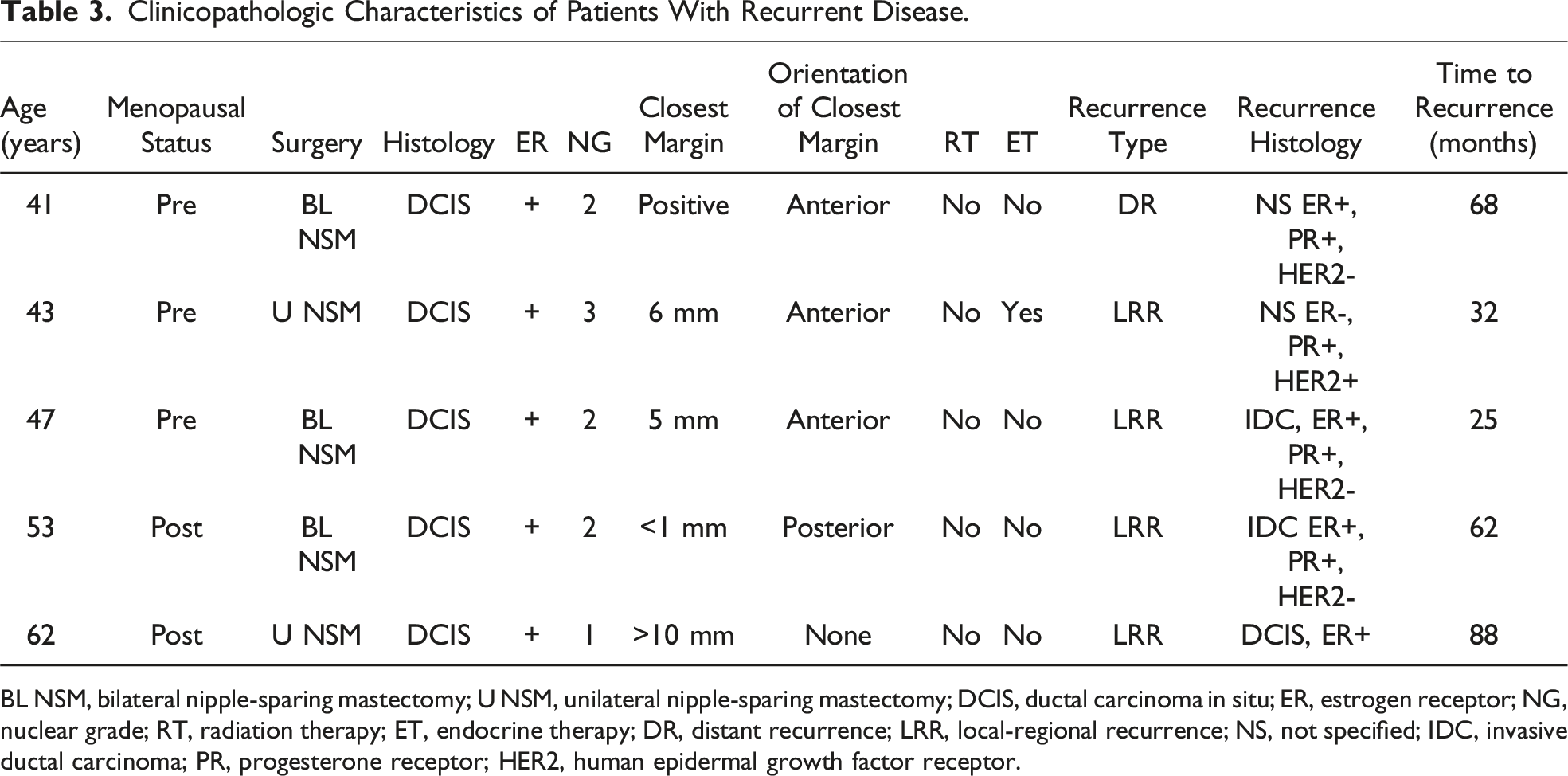
BL NSM, bilateral nipple-sparing mastectomy; U NSM, unilateral nipple-sparing mastectomy; DCIS, ductal carcinoma in situ; ER, estrogen receptor; NG, nuclear grade; RT, radiation therapy; ET, endocrine therapy; DR, distant recurrence; LRR, local-regional recurrence; NS, not specified; IDC, invasive ductal carcinoma; PR, progesterone receptor; HER2, human epidermal growth factor receptor.
Discussion
While there is a generally recognized and accepted margin width for DCIS or DCIS + MI in patients undergoing breast conservation surgery, there is no consensus regarding acceptable margins in patients undergoing mastectomy. As the incidence of DCIS increases along with the utilization of NSM in the treatment for breast cancer, determining an adequate margin width in this setting is needed. This retrospective review evaluating NSM margin width and recurrence risk in patients with DCIS and DCIS + MI suggests that <2 mm margins may be acceptable from an oncologic standpoint.
In a meta-analysis including over 30,000 patients which examined invasive breast cancer margins and recurrence risk following SSM and SM, this demonstrated a 2 to 3-fold increased risk of LR and also suggested an increased risk for DR for close or positive margins compared to negative margins. 3 Conversely, our study demonstrated no association between margin width and recurrence risk. However, the meta-analysis was not specific to patients with DCIS or DCIS + MI and did not include patients undergoing nipple-sparing mastectomy (NSM). The difference in findings may be in part related to the distinction between invasive breast carcinoma and DCIS when anatomic margins are accounted for. With mastectomy, the goal is to preserve the overlying skin envelope while minimizing residual glandular tissue by dissecting in the mastectomy plane. Consequently, close or positive margins in the setting of noninvasive disease may represent anatomic margins, unlike invasive cancer where there is potential for invasion into the subcutaneous tissue. 9 The anterior margin was most frequently identified as the closest margin in our study, and the anatomic margin may explain the lack of a significant association between margin orientation and recurrence risk.
In a more recent analysis, specifically examining DCIS margins for any type of mastectomy, margin width was not found to be associated with local or distant recurrence risk, with overall rates of 2.4% and 1%, respectively, in comparison to 15.4% having close or positive margins. However, only 15 of 282 patients underwent NSM. 4 Comparably, we demonstrated a LRR risk of 2.5% and DR risk of .6%, when accounting for a cohort with 21.7% having positive or <2 mm margins, and no recurrences at the NAC. This again demonstrates that margin status may not play a significant role in LRR in DCIS or DCIS + MI patients undergoing NSM, and further supporting its oncologic safety.
The oncologic safety of NSM has also previously been questioned due to greater concern for residual breast tissue at the mastectomy flap and occult involvement of the NAC, and reasonably close or positive margins may play a more significant role in these patients. 10 Multiple studies have since found NSM to be oncologically safe and in one such report, wherein 23% of the patients underwent NSM for DCIS, LRR was 3.7% and DR was 2.7%. Nipple margins were reported in this study, but otherwise margin status was not specifically examined. 11 Similarly, our study demonstrates an overall low rate of recurrence at 3.1%.
Other studies indicate that while LRR may be increased with close or positive margins for pure DCIS (5.3% vs 1.6% with a wider margin), post-mastectomy radiation does not significantly reduce this risk. 12 We similarly found that radiation in this setting was likely not associated with LRR, although, only one patient in our study received adjuvant radiation. Regarding the prognostic implication of ER status with recurrence risk, we found that ER status was not associated with LRR or DR. However, the literature varies on defining this association. In a recent analysis examining recurrences after NSM with pure DCIS, on univariate analysis, 10-year LRR was 19.1% in ER- DCIS vs 2.9% in ER+ DCIS (P = .002), but on multivariate analysis this was not significant. 13 In another recent analysis, while not significant, ER status tended to be related to recurrence risk. 4 Meanwhile, another study examining the prognosis of tumor markers in DCIS did not find ER status to be significantly linked to recurrence. 14
With the rising incidence of DCIS and utilization of NSM, a consensus regarding adequate margins and subsequent management in this setting is needed. While wider margins are recommended in patients undergoing BCS, this retrospective review of patients with DCIS and DCIS + MI undergoing NSM, including subsequent management and outcomes, suggests that margins of <2 mm may be acceptable and are not significantly associated with recurrence risk. Limitations of the study include its retrospective nature and limited overall follow-up. Additional limitations include a modest sample size with few recurrences from which to draw strong conclusions. Similarly, there were also few patients receiving adjuvant radiation or endocrine therapy. However, to our knowledge, this is the largest study examining detailed margin status and recurrence risk in DCIS patients undergoing NSM specifically. Consequently, future directions for examining the association and management of margins in patients undergoing NSM for DCIS could include larger, prospective studies and more comprehensive examination of the role of adjuvant radiation and endocrine therapies, especially in patients with close or positive DCIS margins.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.