
Abstract
Background
There lacks rapid standardized bedside testing to screen cognitive deficits following mild traumatic brain injury (mTBI). Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test (ImPACT-QT) is an abbreviated-iPad form of computerized cognitive testing. The aim of this study is to test ImPACT-QT utility in inpatient settings. We hypothesize ImPACT-QT is feasible in the acute trauma setting.
Method
Trauma patients ages 12-70 were administered ImPACT-QT (09/2022-09/2023). Encephalopathic/medically unstable patients were excluded. Mild traumatic brain injury was defined as documented-head trauma with loss-of-consciousness <30 minutes and arrival Glasgow Coma Scale 13-15. Patients answered Likert-scale surveys. Bivariate analyses compared demographics, attention, motor speed, and memory scores between mTBI and non-TBI controls. Multivariable logistic regression assessed memory score as a predictor of mTBI diagnosis.
Results
Of 233 patients evaluated (36 years [IQR 23-50], 71% [166/233] female), 179 (76%) were mTBI patients. For all patients, mean test-time was 9.3 ± 2 minutes with 93% (73/76) finding the test “easy to understand.” Mild traumatic brain injury patients than non-TBI control had lower memory scores (25 [IQR 7-100] vs 43 [26-100], P = .001) while attention (5 [1-23] vs 11 [1-32]) and motor score (14 [3-28] vs 13 [4-32]) showed no significant differences. Multivariable-regression (adjustment: age, sex, race, education level, ISS, and time to test) demonstrated memory score predicted mTBI positive status (OR .96, CI .94-.98, P = .004).
Discussion
Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test is feasible in trauma patients. Preliminary findings suggest acute mTBIs have lower memory but not attention/motor scores vs non-TBI trauma controls.
• Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test is feasible and efficient in acute trauma patients in uncontrolled emergency room and hospital settings. • Memory scores were lower in mTBI patients than trauma controls, suggesting memory score as a potential adjunct screening tool in acute mTBI.Key Takeaways
Introduction
Mild traumatic brain injury (mTBI, “concussions”) represents the most common form of TBI, with a 100 per 100,000 annual incidence worldwide. 1 Despite its classification as “mild,” mTBI encompasses a spectrum of cognitive, physical, and affective symptoms. In particular, cognitive symptoms such as memory problems, 2 reduced attention span, and slower motor speed are significant causes of difficulty returning to work 3 and self-reported patient disability. 4
Diagnosing mTBI is challenging due to the subtlety of clinical symptoms, the ambiguity of radiographic findings, and the absence of identifiable biomarkers. 5 A challenge in the trauma setting is the acute triage of mTBI patients, as these patients may not require hospitalization but may have substantial early cognitive impairment. 6 However, the diagnosis of mTBI is likely underreported in acute settings, as many patients underreport symptoms and/or hospital systems may not capture cognitive deficits in patients who are discharged directly from the emergency department. The number of patients discharged has even more recently increased due to increased data on the safety of this practice. 7 In addition, formal cognitive evaluations are time-consuming and require highly specialized providers such as occupational therapists and/or speech therapists to administer these tests. 7 To date, there is a paucity of standardized, validated bedside exams that can be administered by nursing staff to screen for cognitive deficits in mTBI patients.
This study aimed to evaluate this gap with the administration of the Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test (ImPACT-QT), an FDA-approved iPad variant of the computerized ImPACT test 8 for triaging trauma patients for mTBI-related cognitive symptoms. This test has previously been utilized for outpatient testing and sports-related injuries.9,10 However, no studies tested this as a method for cognitive evaluation in acute adult TBI patients within the Emergency Department.
Therefore, the primary aim of this study is to demonstrate the feasibility of implementing ImPACT-QT in the acute emergency and inpatient setting of a level-1 trauma center. We hypothesize in mTBI acute trauma populations the test can be performed rapidly with minimal negative impact on patient symptoms or workflow. As a secondary exploratory aim, we compare score differences between mTBI vs those without mTBI, hypothesizing that patients with mTBI would have worse performance of memory score.
Methods
The study adhered to ethical guidelines with protocol and consent exemption approval from our local Institutional Review Board (Protocol #3070).
Study Design
Prospective cohort study
ImPACT-QT neurocognitive testing
The Immediate Post-Concussion Assessment and Cognitive Testing – Quick Test (ImPACT-QT, ImPACT Application Inc, San Diego, CA) was used to measure neurocognitive performance. Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test is an FDA-approved iPad-based tool for pre-injury and post-injury concussion assessments. The ImPACT-QT iOS ImPACT-QT Application Toolkit was installed on a dedicated 10.2-inch 9th generation Apple iPad (Apple Computer Inc, Cupertino, CA) using iPad OS 15. The ImPACT-QT module consists of a self-reported demographic and symptom survey followed by neurocognitive tests, and the data is stored securely via a web interface.
Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test evaluates three broad cognitive domains “Attention Tracker,” “Motor Speed,” and “Memory” through a subset of five neurocognitive tests.
8
These tests are components of the larger computerized ImPACT test. 1. Symbol Match-Speed subtest: test takers match a series of paired symbols with numbers. 2. Symbol Match-Memory subtest: test takers recall the number-symbol pairs. 3. Three Letter Memory—speed subtest: test takers are presented with a grid of randomized numbers and are asked to choose the numbers in a backward order. 4. Three Letter Memory—memory subtest: test takers are shown three random consonants and must recall the consonants after performing another test. 5. Attention Tracker—reaction time and sustained attention: test takers watch a moving circle and tap the circle when it changes color.
The test outputs a composite score in three domains, representing percentile performance compared to a normative data set. This normative data set consists of a 772-person cohort across various ages and races without known neurologic, psychiatric, or drug use history. ImPACT testing also took place in a research environment as specified by the ImPACT-QT manual.8,11 Manufacturer recommendations include a testing environment free of noise/distraction, no alcohol or recreational drug use, testing in one sitting, and taking the test in an upright position using a table.
Participants, Procedure, and Outcomes
Immediate Post-Concussion Assessment & Cognitive Testing-Quick Test was sequentially administered to trauma activations at our level-1 trauma center. This prospective and sequential administration aimed at evaluating cognitive functions within 72 hours of patient arrival. A convenience sample encompassed both ED and admitted trauma patients. To identify suitable participants, daily trauma service patient lists were scrutinized on weekdays. Test administrators, independent of the study’s design and blind to its analysis, conducted this review. Testing was restricted to a single attempt per patient, during which the administrators refrained from interaction or assistance. The duration of the ImPACT cognitive modules was recorded. Following testing, patients were given an optional post-test paper survey. Patient demographics, hospital metrics, and Rancho Los Amigos Scores were manually extracted from the electronic medical record.
The primary outcome was self-reported survey metrics by patients after performing ImPACT testing. Secondary outcomes were a clinical diagnosis of concussion and Rancho Los Amigos Score.
Inclusion and Exclusion Criteria
mTBI was classified using specific criteria: a Glasgow Coma Scale of 13-15 at initial assessment, loss of consciousness less than 30 minutes, witnessed or reported head trauma, high-risk mechanism (MVC, peds vs adult, fall), and a clinical mTBI diagnosis in the trauma attending physician’s note. This definition shares clinical definitions with updated American Congress of Rehabilitation Medicine Diagnostic Criteria 12 and was intentionally broad in order to achieve sample size. We utilize a TBI definition that includes both radiographically (CT) negative and positive TBI because of a priori determination that CT-positive TBI accounts for a small minority of our population and radiographically negative TBI is most common and is known to cause disability and cognitive symptoms. 13 Non-head trauma controls were identified as trauma activations not meeting the aforementioned mTBI criteria upon chart review.
Inclusion criteria were trauma activations, age 12 to 70, and proficiency in reading Spanish or English. We excluded encephalopathic patients, active alcohol withdrawal, recent sedation/analgesia, and physical impediments barring the use of an iPad. Test administrators were at discretion to exclude patients determined to be medically or surgically unstable or with bodily injury (eg, eye and arm) that would not be compatible with using an iPad. Patients unable to complete testing despite selection were excluded.
Statistical Analysis
Descriptive statistics and univariate analysis were performed. Continuous variables were assessed using Student’s t test, while categorical variables were analyzed using Chi-Square or ANOVA. Normality was determined with the Shapiro-Wilk Test. Non-parametric testing was used for the Kruskal-Wallis Test for continuous variables or Fischer’s Test for categorical variables. Multivariable logistical regression identified potential confounders in acute cognitive testing informed by literature review and group consensus. Statistical significance was defined as P < .05. Statistical Analysis was performed with R Studio v. 4.3.2 (Boston, MA).
Data Statement: Anonymized data source is available per request.
Results
Study Demographics
Of 233 included patients, 71% (166/233) were female, 56% (130/233) were non-white, and the median age was 33 [IQR 23-50]. Of all patients, 77% (179/233) sustained mTBI. The median ISS was 5 [IQR 1-9], Abbreviated Injury Scale (AIS) Head Score was 1 [IQR 1-2], and only 25% of patients underwent Rancho Los Amigos testing with scores ranging between 6 and 8 (median score = 8).
Univariate Analysis of mTBI vs Trauma Patients
Demographic and Cognitive Scoring in Mild Traumatic Brain Injury (mTBI) Versus Non-traumatic Brain Injury Trauma Controls.
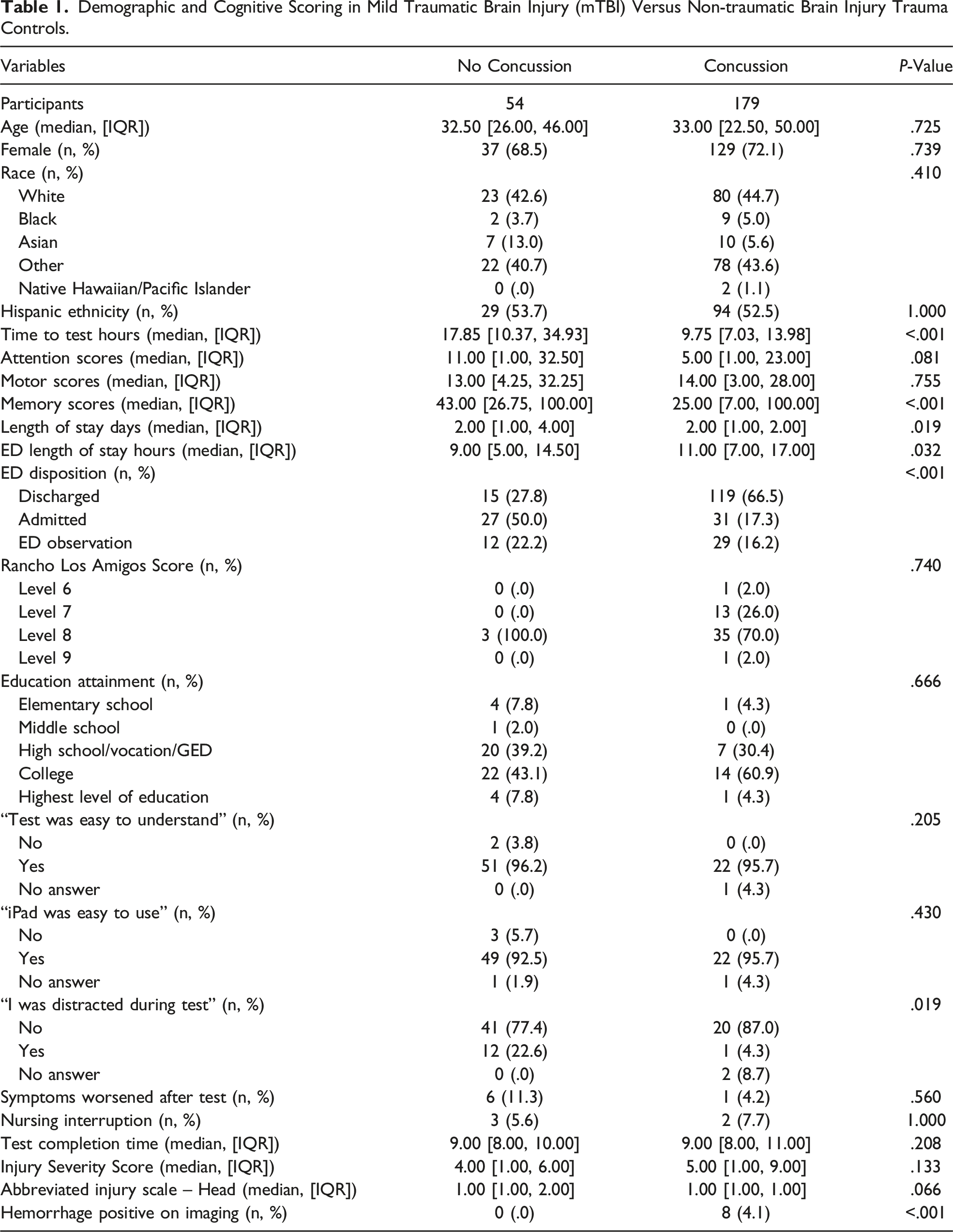
Regardless of TBI status, average cognitive scores were below the 50th percentile. There was no difference in motor (14 vs 13 percentile, P = .755) or attention scores mTBI (5 vs 11 percentile, P = .081) between mTBI and control groups. Memory scores were significantly lower in the mTBI group vs control (25 vs 43 percentile, P < .001) (Figure 1). Violin plots of scores in mild traumatic brain injury (mTBI) versus non-traumatic brain injury trauma controls.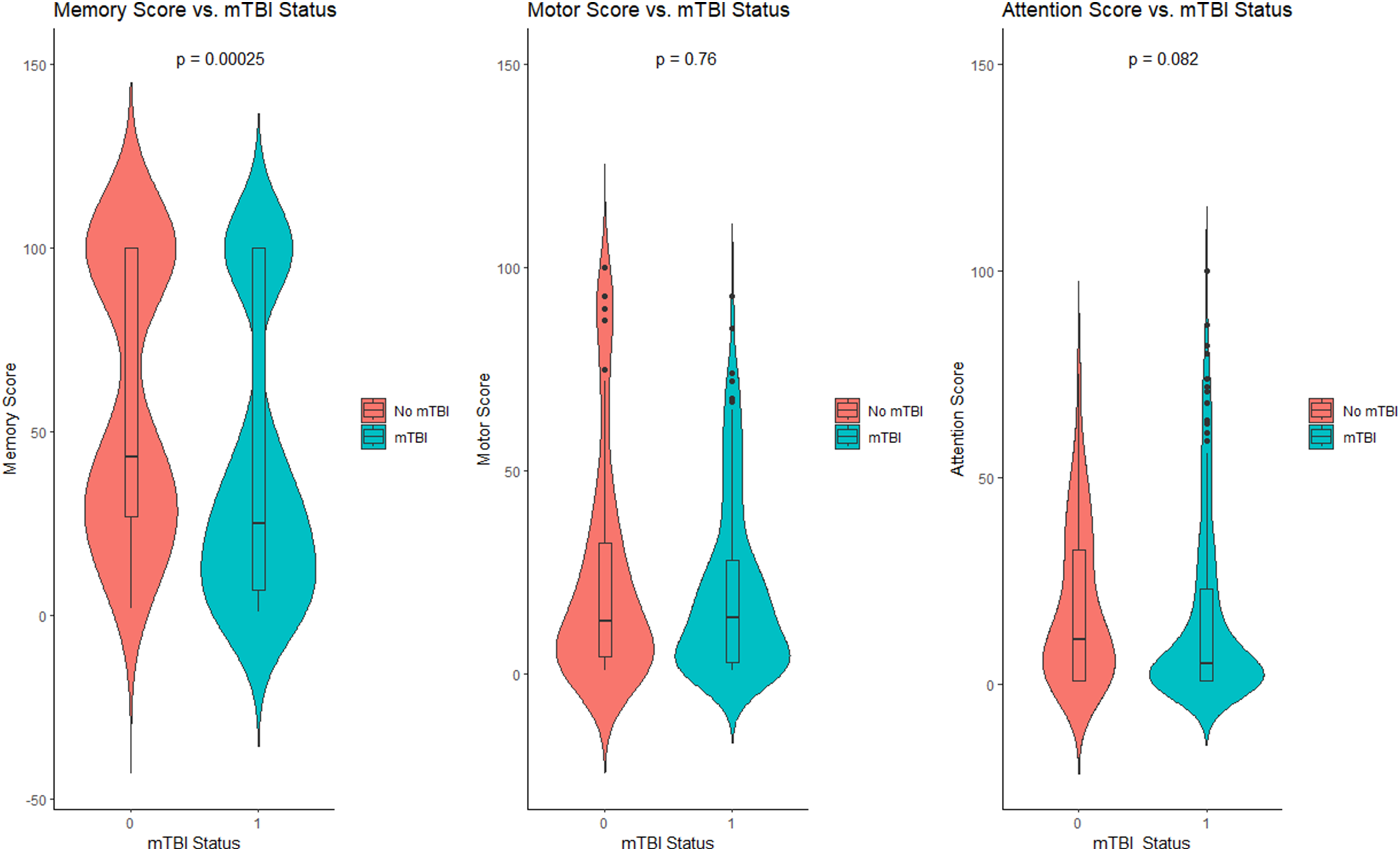
Post-Testing Survey Results
A total of 76 (32%) participants completed post-ImPACT surveys. Highest level of education in 53 percent (41/76) of surveyors was college-graduate or above. Of those surveyed, testing was deemed easy to understand, and the iPad easy to use in more than 90% of participants regardless of cohort (Table 1). Only 1 patient (4%) in the mTBI group felt symptoms worsened post-testing, and both groups had minimal disruption to nursing care. More control patients felt distracted during testing than patients in the mTBI group (22% vs 4%, P = .019). Median test completion time for all participants was 9 minutes.
Multivariable Analysis
On multivariable analysis, when controlling for age, sex, race, highest education level, ISS, and time to test administration, an increased memory score predicted a lower risk of mTBI (OR .96, CI .94-.98, P = .004). In an exploratory regression model of scores predicting Rancho Los Amigos score by inpatient speech therapy, none of the ImPACT-QT cognitive tests predicted Rancho Los Amigos of >8 (OR 1, CI: 98-1.01, P = .9).
Discussion
This is the first study to demonstrate that ImPACT-QT, an iPad-based neurocognitive test, is feasible in a busy trauma setting. Notably, the test is safe, performed under 10 minutes, understandable by patients, and does not disrupt clinical care. In our exploratory second analysis, we found the test demonstrates lower memory scores in mTBI than in non-TBI trauma patients. This rapid bedside tool may be useful for triaging post-mTBI cognitive deficits in resource-limited environments without access to speech-language pathologist, psychologist, or specialty concussion care.
We show in this study that ImPACT-QT is feasible once a patient obtains the device, nevertheless a key next step in practical implementation is better understanding the effect and barriers of patient flow. The barriers to implementation are seen by the fact that time to testing was longer in the non-concussion group. This may reflect our hospital and research screening bias. For example, non-head trauma may be deemed lower priority for cognitive assessment because of need for extra-axial care or pending discharge. In contrast, our hospital protocol prioritizes cognitive screening for primary head trauma, especially if intracranial abnormalities are identified. Patient location may also be a factor in testing implementation. mTBI patients had longer ED stays and higher proportion of discharge from the ED. In contrast, non-mTBI patients had higher admission rates and more testing was performed in the ward setting rather than ED. This suggests complexities intrinsic to some groups of trauma patients, and the movement and disposition of patients may delay identification or testing of appropriate patients. There were no differences in ISS or AIS between groups, but the effect of imbalances in hospital setting on scoring will need to be studied.
Memory scores were lower in clinical TBI patients vs non-head trauma patients, while attention and motor scores were low in both TBI and non-head trauma patients. This exploratory study sought to evaluate the score ranges of ImPACT-QT in a “real-world” setting. Patients in the emergency room and trauma settings in contrast to manufacturer recommendations are in an uncontrolled setting. The trauma setting has multiple distractors including hospital sound, medical care/intervention, medications, and psychological stressors. ImPACT reports scores as percentile outputs which are performance percentile from a reference group that took the test in a highly controlled setting and it is common for healthy populations to score below 25th percentile on one score parameter. 11 Unsurprisingly, cognitive scores of even non-TBI trauma patients were below the 50th percentile. This suggests all scores are to some extent confounded by the trauma setting. Nevertheless, the finding of significantly lower memory scores in TBI patients despite this uncontrolled test setting suggests memory score may be an objective biomarker in clinical mTBI.
To date, only two other studies have tested ImPACT-QT in non-normative populations, both in athletic populations.9,14 The iPad interface is appealing in a trauma setting due to its mobility and user-friendly interface compared to traditional cognitive batteries which often require trained personnel. Though ImPACT-QT shares similarities with the computerized ImPACT, the effect of mobile device interfaces on reported scores is not known. In a comparison between ImPACT Computerized vs ImPACT-QT batteries, a study found the latter had significantly higher scores in four speed-based motor subtests. Furthermore, ImPACT testing in non-sports populations lacks rigorous evaluation and is more robust with a pre-testing baseline, which is not practical in an acute concussion population. ImPACT testing is known to have a high rate of baseline invalidity 15 and varying retest reliability, 16 and it is unknown what general trauma population factors may contribute to the known limitations of ImPACT.
Our findings are important because the current literature on neurocognitive testing in the acute non-sport TBI setting is mixed and limited. Lunter et al successfully implemented the Cambridge Neuropsychological Test Automated Battery iPad application in an emergency department and found differences in reaction time and executive functioning among concussion vs trauma control. 17 Similarly, computerized ImPACT was implemented in a pediatric emergency department with no disruption to workflow and showed most pediatric mTBI patients performed below the 25th percentile across neurocognitive domains. 18 In contrast, a battery of computerized neurocognitive tools including ImPACT failed to differentiate between mTBI and trauma controls. 19 Though we did not find a relationship between ImPACT-QT scores and the Rancho Los Amigos Scale or investigate long-term cognitive outcomes, studies found early acute neurocognitive changes predict risk for persistent post-concussion syndrome. 20 The heterogeneity of study findings likely reflects the heterogeneity of methodology, test batteries utilized, and study outcomes. Future randomized head-to-head testing across rapid-neurocognitive batteries and gold-standard neuropsychology testing in acute adult mTBI is still needed.
Key limitations in our study include the small sample size, lack of pre-injury testing, serial testing, lack of health control, and dependence on normative percentiles. We utilized a clinician definition of mTBI, relied on EMR chart extraction, and performed convenience sampling of ED trauma patients fitting a pre-determined criterion. Though we found no difference among number of patients cared for by the providers, we acknowledge possible diagnosis bias from different clinicians. Therefore, this study may not reflect the true incidence of mTBI. We did not investigate the role of radiographic positive head trauma on findings due to small sample size. We did not perform patient matching such as propensity given limitations of study design, though we are conducting an ongoing study to address this. Our findings reflect an academic level-1 trauma center in Southern California which may limit generalizability. Though we noted no differences in baseline demographics and education level between mTBI and trauma controls, we did not account for all socioeconomic or baseline patient factors that may influence cognitive testing performance. Our study was underpowered to assess the validity of the device in screening cognitive deficits, relationship between test scores, and standard inpatient cognitive testing (Rancho Score) and lacks long-term outcomes. Finally, patients only had one attempt at testing, and we did not control for all confounding neurological, medications, and hospital environment factors, which may account for poor performance on testing.
Conclusion
In this study, we demonstrate the feasibility of an iPad-based neurocognitive in adult patients at a level-1 trauma center. We show lower memory scores in clinical mTBI than non-head trauma controls. This study suggests ImPACT-QT as one possible adjunct tool to screen for mTBI in acute trauma and assist in triaging mTBI patients for further cognitive workup. Future studies will investigate the impact on quality metrics and long-term patient cognitive outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.