
Abstract
Introduction
Fibrosis and cirrhosis are associated with worse outcomes after hepatectomy. Aspartate transaminase to platelet ratio index (APRI) is associated with fibrosis and cirrhosis in hepatitis C patients. However, APRI has not been studied to predict outcomes after hepatectomy in patients without viral hepatitis.
Methods
We reviewed the ACS-NSQIP dataset to identify patients who underwent a minor hepatectomy between 2014 and 2021. We excluded patients with viral hepatitis or ascites as well as patients who underwent emergent operations or biliary reconstruction. APRI was calculated using the following equation: (AST/40)/(platelet count) × 100. APRI ≥0.7 was used to identify significant fibrosis. Univariable analysis was performed to identify factors associated with APRI ≥0.7, transfusion, serious morbidity, overall morbidity, and 30-day mortality. Multivariable logistic regression was performed to identify adjusted predictors of these outcomes.
Results
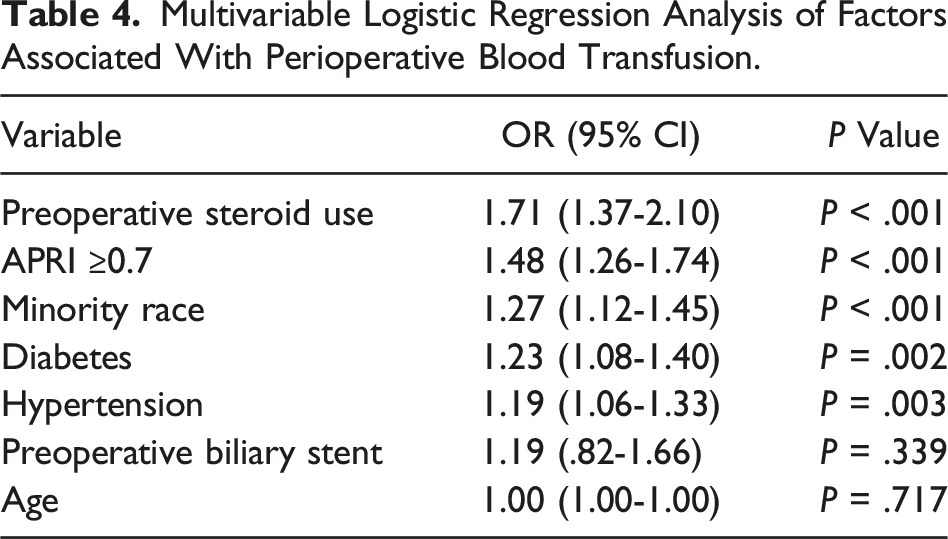
Of the 18,069 patients who met inclusion criteria, 1630 (9.0%) patients had an APRI ≥0.7. A perioperative blood transfusion was administered to 2139 (11.8%). Overall morbidity, serious morbidity, and mortality were experienced by 3162 (17.5%), 2475 (13.7%), and 131 (.7%) patients, respectively. APRI ≥0.7 was an independent predictor of transfusion (adjusted OR: 1.48 [1.26-1.74], P < .001), overall morbidity (1.17 [1.02-1.33], P = .022), and mortality (1.97 [1.22-3.06], P = .004). Transfusion was an independent predictor of overall morbidity (3.31 [2.99-3.65], P < .001), serious morbidity (3.70 [3.33-4.11], P < .001), and mortality (5.73 [4.01-8.14], P < .001).
Conclusions
APRI ≥0.7 is associated with perioperative transfusion, overall morbidity, and 30-day mortality. APRI may serve as a noninvasive tool to risk stratify patients prior to elective minor hepatectomy.
Introduction
Degrees of fatty liver disease (FLD), such as fibrosis and cirrhosis, are associated with an increased risk of perioperative surgical complications and transfusions after hepatectomy.1-4 In a matched cohort analysis of patients who underwent major hepatectomy, McCormack and colleagues found a 14% mortality rate in the moderate/severe hepatic steatosis cohort compared to 6.8% in the mild hepatic steatosis cohort and 1.7% in the normal liver cohort. 4 Furthermore, a higher rate of intraoperative blood transfusions was found among patients with nonalcohol fatty liver disease (NAFLD) compared to those without NAFLD (37.8% vs 28.0%, P = .0208) in a retrospective review of patients undergoing hepatectomy for hepatocellular carcinoma (HCC). 2 Since preoperative liver biopsy is not routinely performed to determine degree of steatosis, identifying which patients are at risk for these complications remains a challenge for surgeons.
The aspartate transaminase to platelet ratio index (APRI) is a biomarker that has previously been found to be a sensitive and specific predictor of fibrosis and cirrhosis among nonsurgical patients with hepatitis C. 5 Likewise, in populations with viral hepatitis undergoing liver resection, an elevated APRI was found to be associated with morbidity and mortality.6-8 However, its application to a surgical population without viral hepatitis remains unknown. In this study, the ACS-NSQIP was reviewed to assess the ability of APRI to predict outcomes following elective minor hepatectomy in a population of patients without viral hepatitis. We hypothesized that APRI would be a significant independent predictor of perioperative transfusion, mortality, overall morbidity, and serious morbidity after minor hepatectomy.
Methods
Patient Selection and Variable Definitions
The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) is a de-identified, hospital-based data set, capturing cases from over 700 hospitals and accruing over a million cases annually. 9 This study was approved by the Institutional Review Board. Cases were reviewed from participant user file (PUF) years 2014 to 2021. Case identification was used to merge cases with the ACS NSQIP Procedure Targeted Database for Hepatectomy. We used Current Procedural Terminology (CPT) code 47120 to identify patients who underwent a minor hepatectomy, which is defined as resection of ≤3 liver segments. 9 These were selected as having the least amount of variability of complication and risk from patient to patient in order to evaluate our study variables. Major hepatectomies (those with >3 resected liver segments) were excluded to limit operative variability in patient risk assessment. Additionally, we excluded patients who underwent an emergent operation, patients with viral hepatitis, and patients with unknown variables. Additionally, as there is no variable for preoperative diagnosis of cirrhosis in the NSQIP, ascites was used as a clinical surrogate for cirrhosis. Patients with ascites were excluded in order to better study operative risk in a surgical population without advanced stage liver disease, but still at-risk for steatohepatitis or fibrosis. Patients who underwent biliary reconstruction were excluded as this would significantly increase risk of complications after a minor hepatectomy.
Baseline demographic and clinical data included in the NSQIP were examined along with our addition of metabolic syndrome, which was defined as a composite of diabetes, hypertension, and BMI ≥30 kg/m2 as previously described.
1
Differences in laboratory values, though statistically significant, were not clinically significant, with the exception of AST and platelet count. Thus, these values were not included. AST to platelet ratio index (APRI) was defined using the following equation:

The upper limit of normal (ULN) for AST was 40 U/L, and this value was used in the numerator for the APRI equation. An APRI value of ≥0.7 was used to identify patients with clinically significant fibrosis, as previously described in patients with hepatitis C. 10 NSQIP 30-day outcomes and hepatectomy-specific outcomes were analyzed. The primary outcomes were mortality and perioperative transfusion. Mortality was defined by death within 30 days after surgery. Perioperative transfusion was defined as receipt of a packed red blood cell transfusion within 72 hours after surgery start time. 9 Serious morbidity was defined as a composite of pneumonia, unplanned intubation, failure to wean from the ventilator after 48 hours, deep surgical site infection, organ space infection, wound dehiscence, pulmonary embolism, myocardial infarction, cardiac arrest, stroke, acute renal failure, sepsis, septic shock, bile leak, invasive postoperative biliary procedure, post-hepatectomy liver failure (PHLF) grade B or C, or reoperation. 1 Overall morbidity included the occurrence of any serious morbidity with the inclusion of the following additional complications: superficial surgical site infection, urinary tract infection, progressive renal insufficiency (postoperative rise in creatinine >2 mg/dl from preoperative value, with no requirement for dialysis), deep vein thrombosis, or PHLF grade A.
Statistical Analysis
Unadjusted analyses were performed to compare demographic and clinical factors associated with APRI ≥0.7, perioperative blood transfusion, mortality, serious morbidity, and overall morbidity. Categorical variables were compared with Pearson’s chi-squared test, and continuous variables were compared with the Mann-Whitney U test. Variables that were both statistically and clinically significant on unadjusted analysis were included in multivariable logistic regression models to identify independent predictors of perioperative blood transfusion, mortality, serious morbidity, and overall morbidity. Additionally, variables with interactions were excluded in our final logistic regression tables. All statistical tests were two-sided and performed using RStudio statistical software with a significance set at P < .05.
Results
Summary
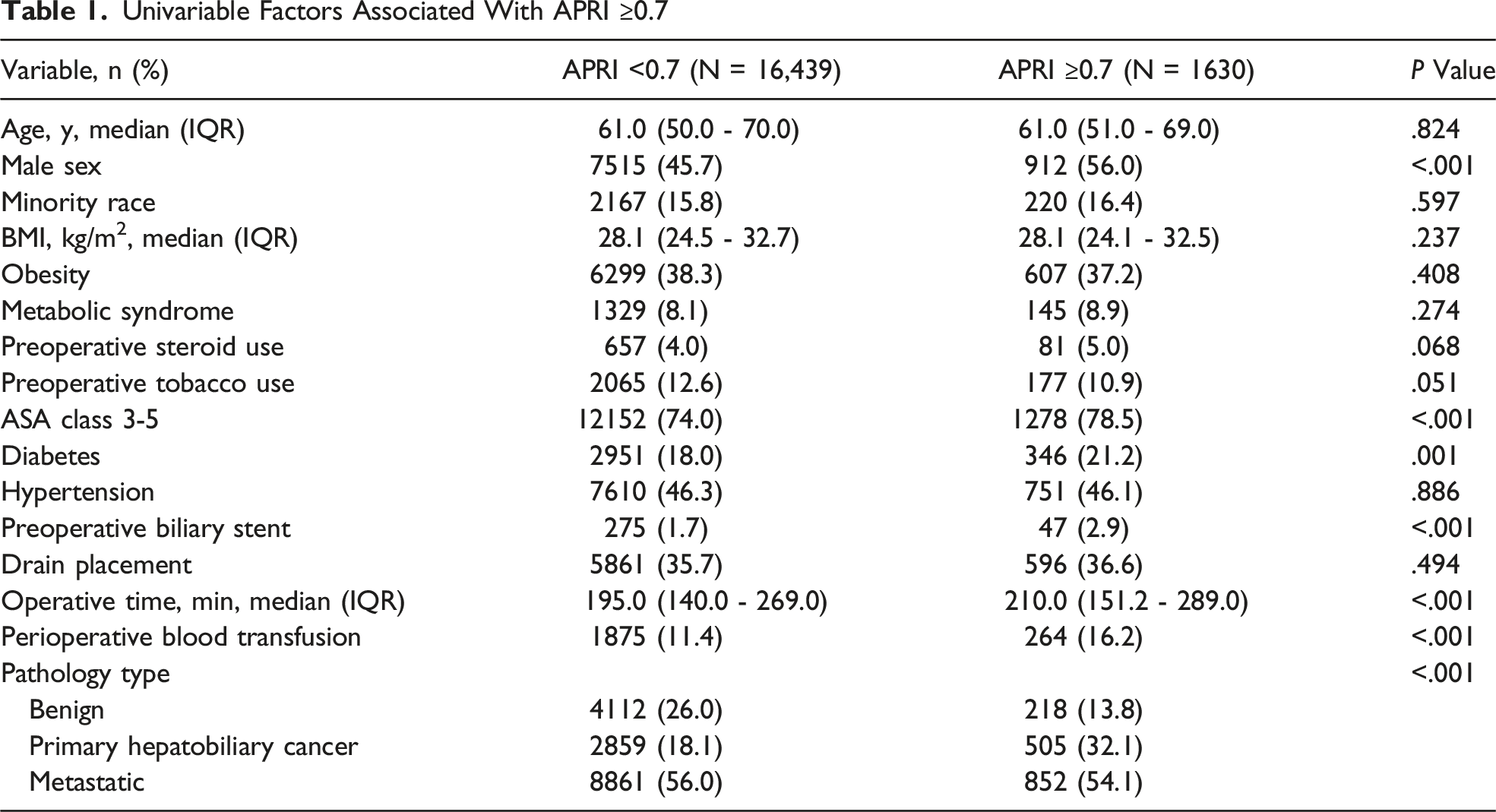
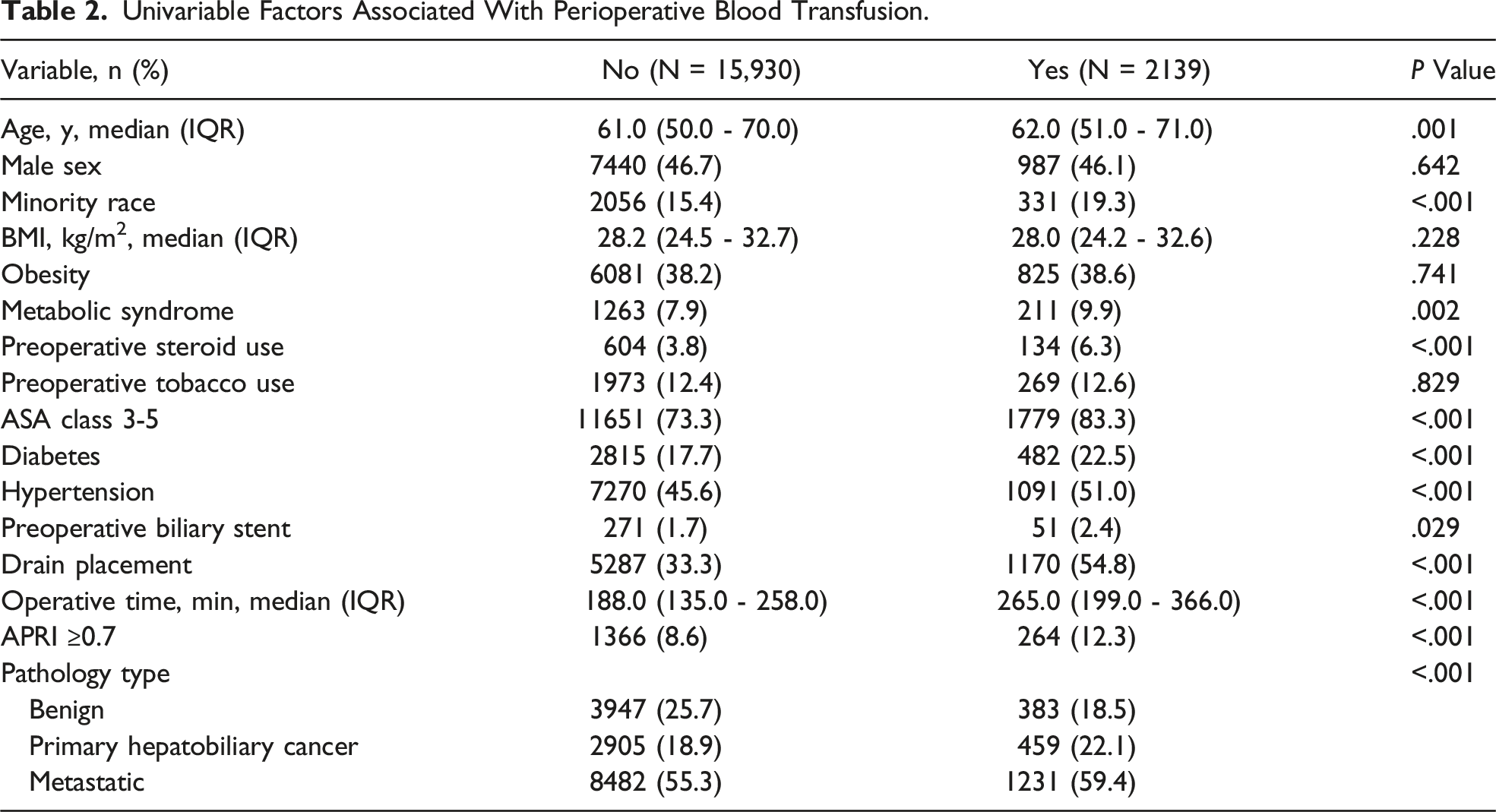
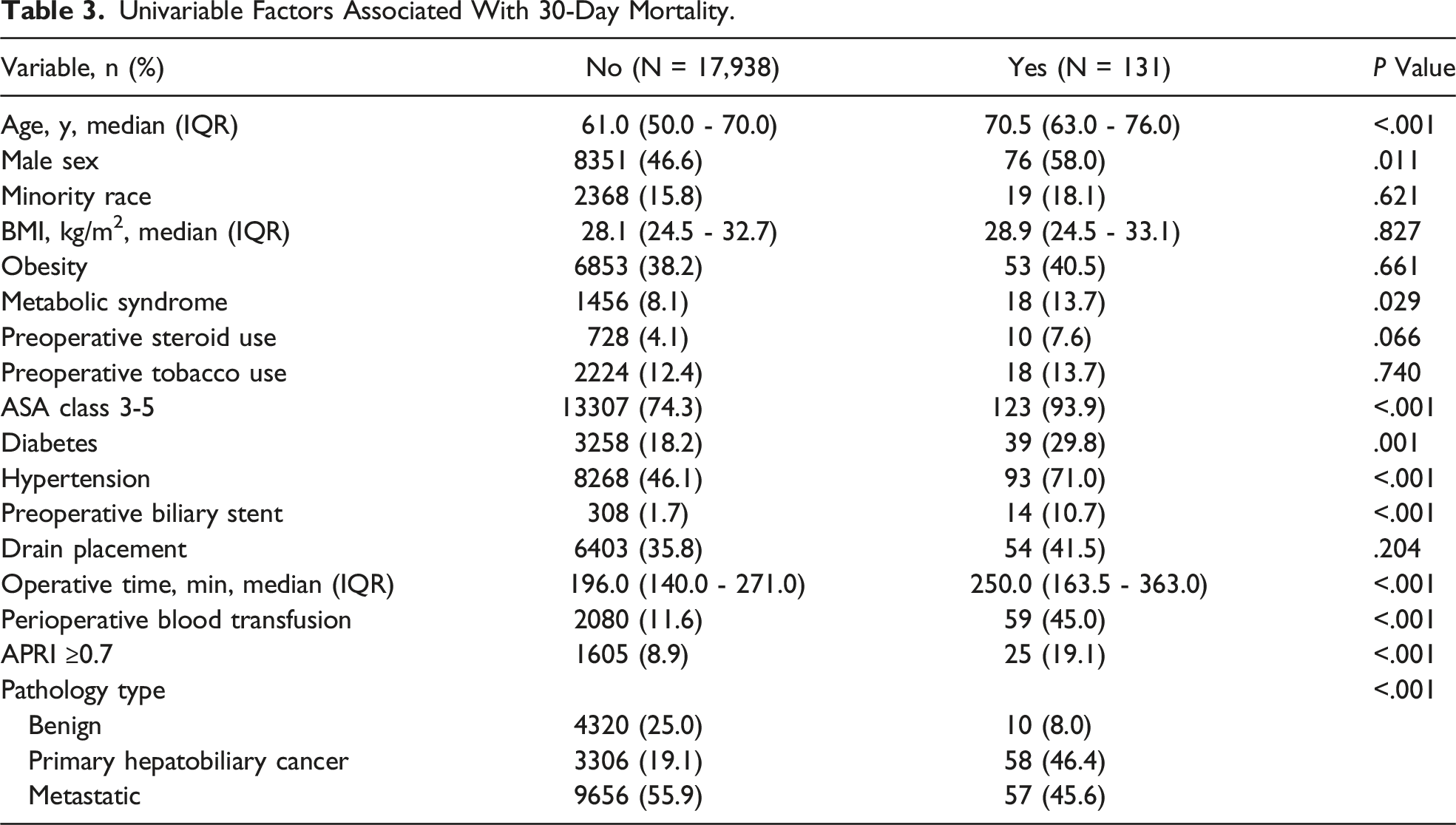
After inclusion and exclusion criteria were applied, 18,069 patients were included in our final cohort. The median age of this cohort was 61.0 years old (IQR: 50.0-70.0). The majority of patients were female (53.3%) and of white race (70.0%). An elevated APRI was found in 1630 (9.0%) patients. A perioperative blood transfusion was administered to 2139 (11.8%) patients. The 3 most common postoperative complications in our study were invasive biliary procedure (6.1%), organ space infection (4.9%), and bile leak (4.3%). Overall morbidity was experienced by 3162 (17.5%) patients; serious morbidity was experienced by 2475 (13.7%) patients. Overall, 131 (0.7%) patients died within 30 days of surgery.
Univariable Analysis by APRI
Univariable Factors Associated With APRI ≥0.7
Univariable Analysis by Perioperative Blood Transfusion
Univariable Factors Associated With Perioperative Blood Transfusion.
Univariable Analysis by Mortality
Univariable Factors Associated With 30-Day Mortality.
Univariable Analysis by Overall and Serious Morbidity
Univariable analysis of preoperative factors associated with overall and serious morbidity revealed comparable findings. Age, male sex, tobacco use, preoperative steroid use, ASA class ≥3, diabetes, hypertension, and preoperative biliary stent placement were all associated with morbidity (Supplemental Tables 2 and 3). Intraoperatively, patients who experienced morbidity were more likely to have undergone drain placement and longer operations. APRI and transfusion were both associated with overall and serious morbidity.
Multivariable Analysis by Transfusion
Multivariable Logistic Regression Analysis of Factors Associated With Perioperative Blood Transfusion.
Multivariable Analysis by Outcome
Multivariable Logistic Regression Analysis of Factors Associated With 30-Day Mortality.
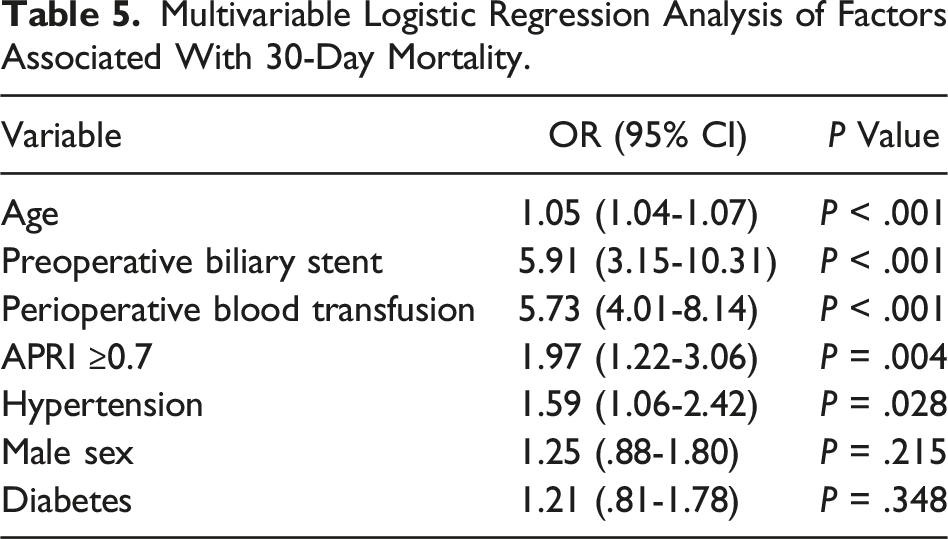
Multivariable regression analysis found transfusion to be predictive of both overall and serious morbidity (Supplemental Table 4 and Supplemental Table 5). Initially, APRI ≥0.7 remained a significant predictor of overall morbidity but not serious morbidity. However, due to collinearity between APRI ≥ 0.7 and transfusion, mortality, serious morbidity, and overall morbidity regression models were re-analyzed without transfusion to test the significance of an elevated APRI without the confounder of transfusion. In these models, APRI ≥0.7 remained independently associated with mortality (2.17 [1.35-3.35], P = .001), serious morbidity (1.23 [1.07-1.41], P = .004), and overall morbidity (1.23 [1.08-1.40], P = .001).
Discussion
In this study, APRI is identified as a predictor of outcomes following non-emergent minor hepatectomy in a population of patients without viral hepatitis. Specifically, an elevated APRI is an independent predictor of an increased risk for perioperative blood transfusion, 30-day mortality, and overall and serious morbidity. Additionally, perioperative transfusion was an independent predictor of mortality, overall morbidity, and serious morbidity. These findings are important in the context of an increasing population of patients receiving hepatectomy with varying degrees of FLD. 11 There has also been an increase in the number of minor hepatectomies being performed, compared to major hepatectomies, further supporting the significance of our study’s findings. 11
Nonalcohol fatty liver disease (NAFLD) is defined as the accumulation of hepatic fat on biopsy or imaging in the absence of secondary causes, including viral hepatitis and alcohol use. 12 With advancements in treatment for and prevention of viral hepatitis, NAFLD is increasing in the western population and is predicted to be the leading cause of fibrosis and cirrhosis by 2030. The gold standard for diagnosing NAFLD is through a liver biopsy; however, a biopsy remains limited in utility due to its invasive nature and risk for sampling error. 13 Thus, utilization of a novel tool to predict post-hepatectomy complications is necessary.
The AST to platelet ratio index (APRI) is one noninvasive biomarker that was first developed in a cohort of 192 patients with hepatitis C in order to predict fibrosis and cirrhosis. 5 Although a single cut-off value for APRI was not determined in this initial study, a subsequent meta-analysis found an optimal APRI cut-off value of 0.7 to predict fibrosis. 10 Our study was designed to further expand the use of APRI as a prediction tool for transfusion and complications after minor hepatectomy. We intentionally excluded viral hepatitis to validate the utility of APRI on a NAFLD population.
Our results are comparable to previous analyses of the ACS-NSQIP. Fagenson et al studied 13,699 minor hepatectomies between 2014 and 2018 and found transfusion to be a significant independent predictor of both serious morbidity (P < .001) and mortality (P < .001). 14 In another analysis of 5337 minor hepatectomies between 2014 and 2018, Villagomez et al found transfusion to be an independent predictor of postoperative infectious complications (P < .05). 3 Previous systematic reviews and single-institution retrospective analyses have found transfusion to be predictive of overall morbidity, major complications, and greater length of stay after hepatectomy.15-18
In addition to short-term mortality risk, there is evidence that transfusions may portend poor 90-day survival as well as long-term disease free survival (DFS) and overall survival (OS) after hepatectomy. Goh et al found intraoperative blood transfusion to be an independent predictor of 90-day mortality (P = .018) in an analysis of patients who underwent minor hepatectomy for HCC. 11 A meta-analysis including 21 studies on patients undergoing hepatectomy for colorectal liver metastases found transfusion was associated with inferior OS. 18 In another systematic review of 18 studies studying the relationship between transfusion after hepatectomy and long-term survival outcomes, 10 of 18 studies, after multivariable analysis, found that transfusion was a negative predictor of OS, DFS, or both. 17 The predictive value of APRI for transfusion in our study suggests that APRI may potentially be predictive of decreased 90-day and long-term survival outcomes after hepatectomy.
There have been few prior analyses examining the utility of APRI and outcomes after liver resections. A 2016 retrospective review of 360 patients with HCC undergoing hepatectomy for HCC, all of whom had viral hepatitis, found an APRI >9.5 to be an independent predictor of postoperative complications. 7 In a 2019 analysis of 321 minor hepatectomies for HCC from the Veterans Administration Corporate Data Warehouse database, an APRI >1.5 was associated with an increased risk for 30-day mortality on multivariable analysis (P < .001). 6 The majority of the patients in this study had hepatitis C, and an APRI cut-off of 1.5 was chosen to identify patients at risk for cirrhosis. A 2020 retrospective review of patients undergoing hepatectomy for HCC found an elevated APRI to be an independent predictor of postoperative morbidity. 8 This analysis also consisted of primarily a cohort of patients with viral hepatitis. In our analysis of a population of patients without viral hepatitis undergoing liver resections for any indication, the ability of APRI to predict transfusion, which was predictive of all outcomes, supports the utility of APRI as a clinical tool to preoperatively risk stratify patients for minor hepatectomy. In patients with an elevated APRI, surgeons should discuss the elevated risk of transfusion and mortality after hepatectomy. In the case of when a patient does not accept blood products, surgeons and patients should consider forgoing hepatectomy.
Our study is limited by inherent selection bias due to retrospective design. As the database only tracks outcomes for 30 days after surgery, we were unable to draw conclusions on postoperative morbidity and mortality after 30 days. Also, while the ACS NSQIP provides a sample of all hepatectomies done in North America, the majority of hepatectomies are performed at academic centers which may bias the results. Additionally, a minor hepatectomy in our study consists of anywhere from a single segmentectomy to up to resection of 3 hepatic segments; the distinction between a wedge resection and a segmentectomy is at the discretion of the operating surgeon. The cut-off value of 0.7 we have used to describe an elevated APRI is based on a meta-analysis of hepatitis C patients, and although we chose this value because of its previously studied association with fibrosis, there may be a more optimal cut-off of APRI for NAFLD.
In conclusion, this study illustrates the utility of APRI as a predictor of transfusion and mortality following non-emergent minor hepatectomy. We have provided further evidence that receiving a perioperative transfusion is a risk factor for postoperative morbidity and mortality. The utility of APRI as a noninvasive and readily available clinical tool will assist in clinical decisions making regarding the risks of minor hepatectomy in the ambulatory setting.
Supplemental Material
Supplemental Material - “The Prognostic Role of AST to Platelet Ratio Index (APRI) on Outcomes Following Non-emergent Minor Hepatectomy”
Supplemental Material for “The Prognostic Role of AST to Platelet Ratio Index (APRI) on Outcomes Following Non-emergent Minor Hepatectomy” by Dhruv J. Patel, Michael T. LeCompte, Hong Jin Kim, and Elizabeth M. Gleeson in The American Surgeon™
Footnotes
Author’s Note
This work was presented as an oral presentation at the Southeastern Surgical Congress 2024 Annual Meeting on February 5th, 2024 in Clearwater Beach, Florida.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.