
Abstract
Background
Patients undergoing emergency general surgery (EGS) often require complex management and transfer to higher acuity facilities, especially given increasing national efforts aimed at centralizing care. We sought to characterize factors and evaluate outcomes associated with interhospital transfer using a contemporary national cohort.
Methods
All adult hospitalizations for EGS (appendectomy, cholecystectomy, laparotomy, lysis of adhesions, small/large bowel resection, and perforated ulcer repair) ≤2 days of admission were identified in the 2016-2020 National Inpatient Sample. Patients initially admitted to a different institution and transferred to the operating hospital comprised the Transfer cohort (others: Non-Transfer). Multivariable models were developed to consider the association of Transfer with outcomes of interest.
Results
Of ∼1 653 169 patients, 107 945 (6.5%) were considered the Transfer cohort. The proportion of patients experiencing interhospital transfer increased from 5.2% to 7.7% (2016-2020, P < .001). On average, Transfer was older, more commonly of White race, and of a higher Elixhauser comorbidity index. After adjustment, increasing age, living in a rural area, receiving care in the Midwest, and decreasing income quartile were associated with greater odds of interhospital transfer. Following risk adjustment, Transfer remained linked with increased odds of in-hospital mortality (AOR 1.64, CI 1.49-1.80), as well as any perioperative complication (AOR 1.33, CI 1.27-1.38; Reference: Non-Transfer). Additionally, Transfer was associated with significantly longer duration of hospitalization (β + 1.04 days, CI + .91-1.17) and greater costs (β+$3,490, CI + 2840-4140).
Discussion
While incidence of interhospital transfer for EGS is increasing, transfer patients face greater morbidity and resource utilization. Novel interventions are needed to optimize patient selection and improve post-transfer outcomes.
Key Takeaways
• A growing proportion of patients undergoing emergency general surgical operations (EGS) are transferred to a different hospital for surgical management. • Older age, hospitalization in the Midwest, residence in a rural area, decreasing income, and White race were associated with increased odds of interhospital transfer. • After risk adjustment, interhospital transfer remained associated with greater morbidity, resource utilization, and discharge to extended care facilities.
Introduction
Accounting for >3 million hospitalizations and $28 billion in expenditures across the United States, each year, emergency general surgery (EGS) represents a significant and growing public health burden.1,2 Patients requiring EGS have been noted to face significant morbidity and may require higher levels of care than offered by local hospitals. 3 Altogether, an estimated 7%-21% of EGS patients are transferred to a different center for further workup and management.2,4 In line with increasing emphasis on centralization of care, the national incidence of interhospital transfer has increased by nearly 150% over the last decade. 2
Prior work examining interhospital transfer has reported such patients to face treatment delays, repeated diagnostic testing, increased complications, and greater expenditures.4–9 However, such reports have largely relied on dated cohorts, considered non-surgical patients, or focused exclusively on high-acuity procedures. Given the lack of consensus guidelines regarding transfer for EGS, a contemporary understanding of the management of such patients would provide a framework for improvement of both quality and value of care.
We examined the association of interhospital transfer with clinical and financial outcomes using a national cohort of high-acuity EGS hospitalizations. We hypothesized that transfer patients would demonstrate face increased complications and costs following EGS compared to those treated at the admitting center.
Methods
Data Source and Study Cohort
The 2016-2020 National Inpatient Sample (NIS) was queried to identify all adult (≥18 years) non-elective hospitalizations involving laparotomy, large bowel resection, lysis of adhesions, perforated ulcer repair, or small bowel resection within 2 days of admission, using previously validated International Classification of Diseases, Tenth Revision (ICD-10) procedure codes.1,10 The NIS is the largest all-payer national database in the United States and provides survey-weighted estimates for ∼97% of all hospitalizations, annually. 11
Entries entailing interhospital transfer were grouped in the Transfer cohort, while those who remained at the admitting facility were considered Non-Transfer. Records for traumatic injuries (3.9%) or missing key data (<1%) were excluded from analysis (Figure 1). Study CONSORT diagram of survey-weighted estimates. Of an estimated 1 728 634 records entailing emergency general surgery identified in the 2016-2020 National Inpatient Sample, 1 653 169 were considered for analysis. Of these, 107 945 (6.5%) experienced interhospital transfer and comprised the Transfer cohort.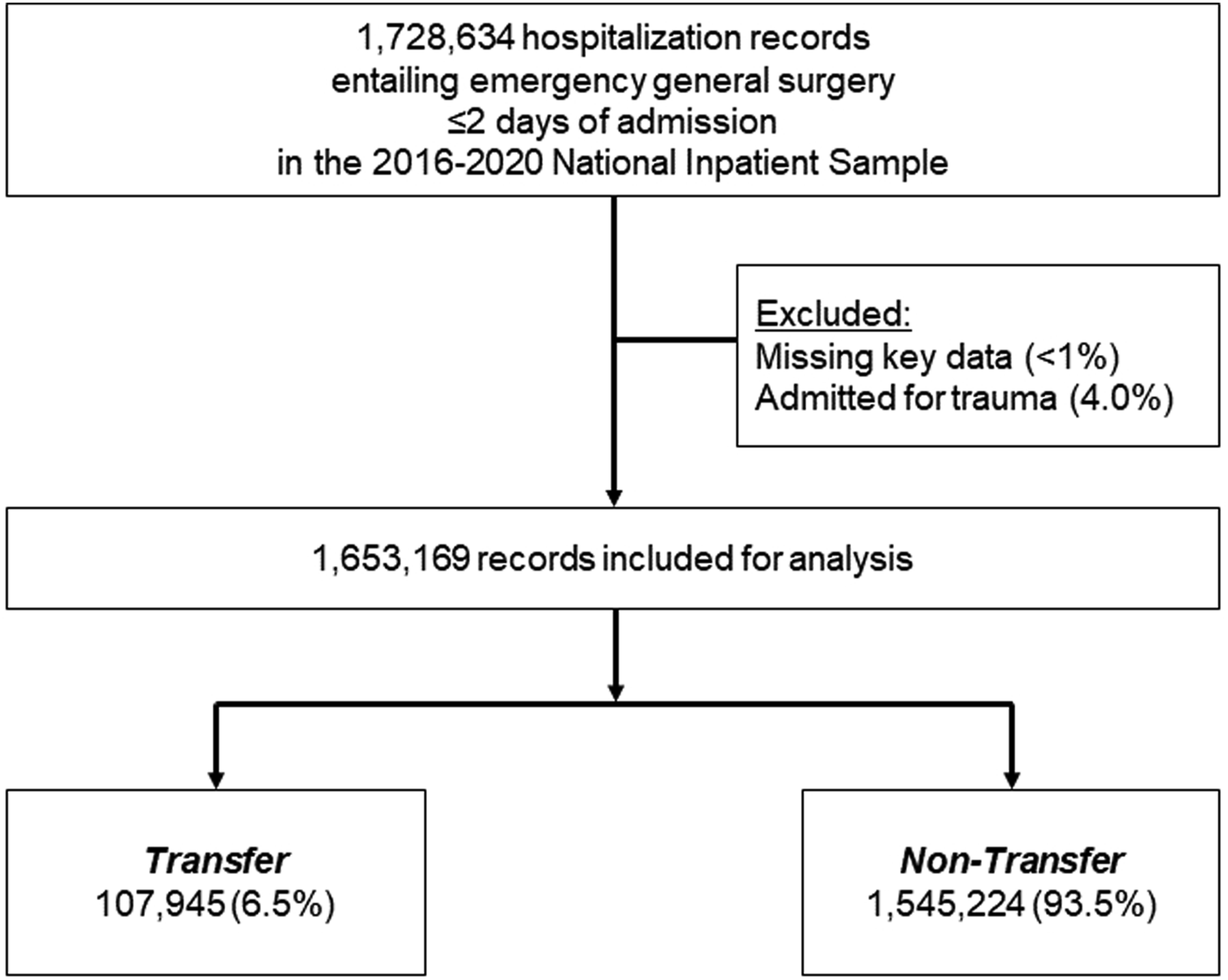
Variable Definitions
Patient and hospital factors, including age, sex, income quartile, insurance coverage, race, and hospital teaching status, were enumerated using the Healthcare Cost and Utilization Project Data Dictionary. 11 The burden of chronic conditions was ascertained using the van Walraven modification of the Elixhauser comorbidity index. 12 Patient rurality was defined in accordance with the county-based urban-rural classification scheme established by the National Center for Health Statistics. 11 Comorbidities and perioperative complications were tabulated using previously described ICD-10 codes. 10 Complications were further stratified into cardiac, gastrointestinal, infectious, renal, respiratory, and thrombotic categories. Unique hospital cost-to-charge ratios were applied to compute overall costs, which were then inflation-adjusted using the 2020 Personal Healthcare Price Index. 11
Study Outcomes
The primary endpoint of this study was in-hospital mortality. We secondarily evaluated the incidence of any perioperative complication, duration of hospitalization (LOS), costs, and discharge to extended care facilities.
Statistical Analysis
Continuous data are presented as medians with interquartile range (IQR), while categorical variables are reported as proportions (%). Bivariate comparisons were performed using the Pearson χ2 and Mann-Whitney U test, as appropriate. The significance of temporal trends was assessed using Cuzick’s nonparametric test.
Entropy balancing was used to adjust for differences in cohort characteristics. Briefly, this approach applies optimal sample weights to achieve covariate balance, while retaining the entire study population. Importantly, entropy balancing has been demonstrated to be a more robust technique compared to propensity matching. 13
Multivariable regression models were subsequently fit to consider the independent association of interhospital transfer with key study outcomes. All covariates for entropy balancing and regression models were selected for inclusion using elastic net regularization. This automated selection method relies on a penalized least-squares method to increase out-of-sample generalizability and minimize model overfitting. 14 Selected covariates included patient age, sex, race, income quartile, insurance coverage, operative type, Elixhauser comorbidity index, rural or urban location, hospital volume, hospital teaching status, hospital region, and year of admission. The receiver operator characteristic (C-statistic) was used to evaluate model goodness of fit. Logistic model outputs are detailed as adjusted odds ratio (AOR), while linear outputs are reported as β-coefficients (β), both with 95% confidence intervals (CIs).
All statistical analyses were performed using Stata 16.1 (StataCorp LLC, College Station, TX). Statistical significance was set at α = .05. The Institutional Review Board at the University of California, Los Angeles determined this study was exempt from full review due to the deidentified nature of the NIS.
Results
Baseline Characteristics of the Study Cohort
Of 1 653 169 records eligible for analysis, 107 945 (6.5%) required interhospital transfer and comprised the Transfer cohort. The proportion of patients transferred to another facility increased over the study period, from 5.2% in 2016 to 7.7% in 2020 (P < .001) (Figure 2). Trends in interhospital transfer for emergency general surgery. Over the 5-year study period, rates of interhospital transfer increased from 5.2% to 7.7% (2016 to 2020). *indicates statistical significance, P for trend <.001.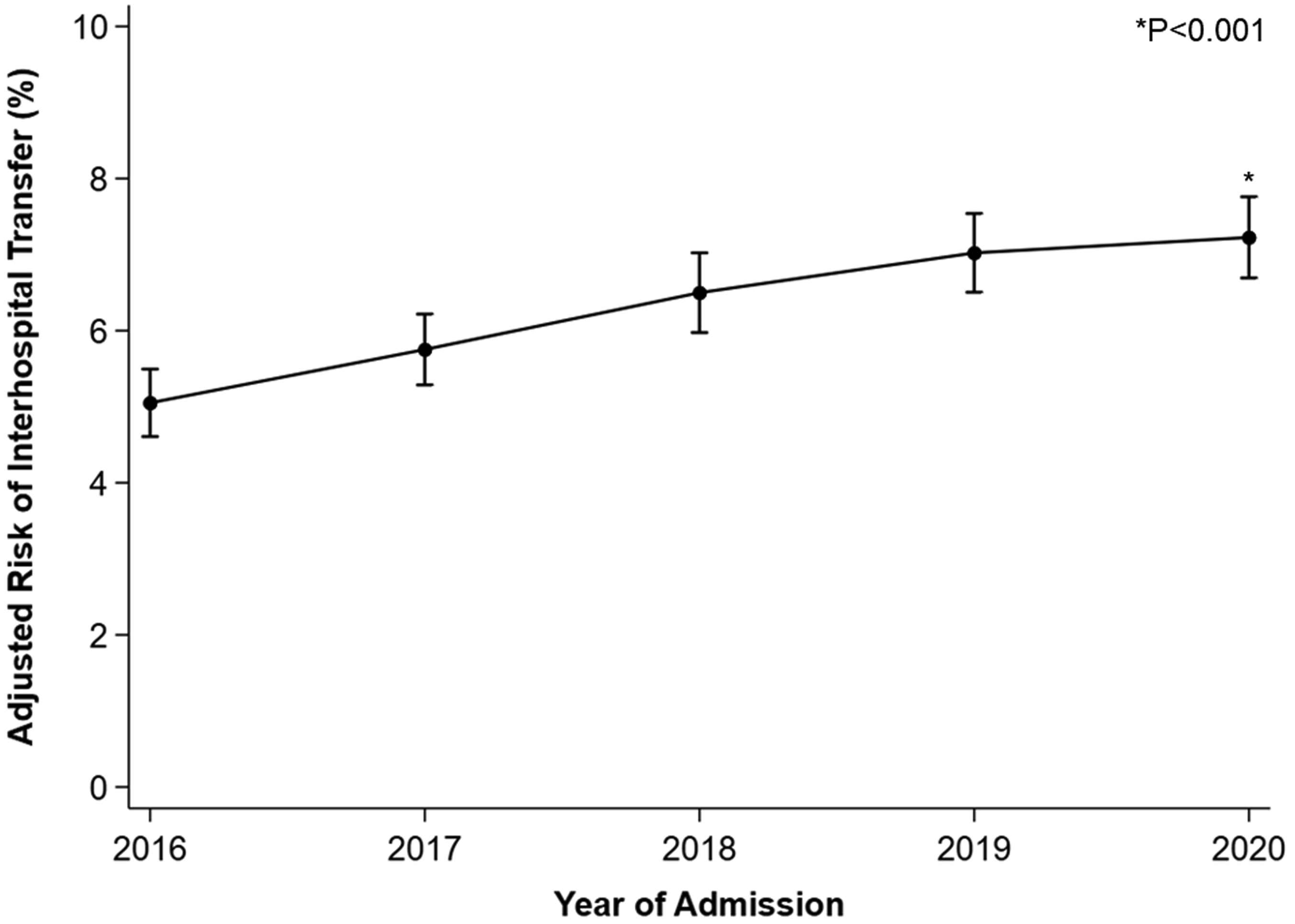
On average, Transfer subjects were older (61 [46-72] vs 57 years [41-71], P < .001), more commonly male (43.0 vs 41.1%, P < .001), and had a higher Elixhauser comorbidity index (3 [1-4] vs 2 [1-4], P < .001). Further, the Transfer cohort was more often of lowest income quartile (34.4 vs 28.1%, P < .001), of White race (77.6 vs 64.0%, P < .001), and insured by Medicare (46.0 vs 37.6%, P < .001), compared to Non-Transfer. Transfer patients more commonly resided in micropolitan (20.7 vs 7.9%) or rural areas (21.3 vs 5.3%, P < .001), and were treated at hospitals in the Midwest (31.9 vs 18.7%, P < .001) (Figure 3). Relative to Non-Transfer, Transfer more frequently underwent large bowel resection (13.5 vs 11.3%), lysis of adhesions (15.9 vs 13.8%), and small bowel resection (10.7 vs 7.4%), but less commonly cholecystectomy (49.6 vs 57.1%, P < .001). Geospatial mapping of transfer patients. We further stratified the study cohort by geographic region of the operating center. Considering all patients undergoing emergency general surgical operations, the proportion experiencing interhospital transfer within each region ranged from 4.3% to 14.9%. The West North Central, including Missouri, North Dakota, South Dakota, Nebraska, Kansas, and Iowa, had the highest proportion of transfer patients (14.9%). Meanwhile, the South Atlantic (4.3%), comprising Delaware, Maryland, District of Columbia, Virginia, West Virginia, North Carolina, South Carolina, Georgia, and Florida, and the Mid Atlantic (4.4%), representing New York, Pennsylvania, and New Jersey, had the lowest proportions of transfer patients.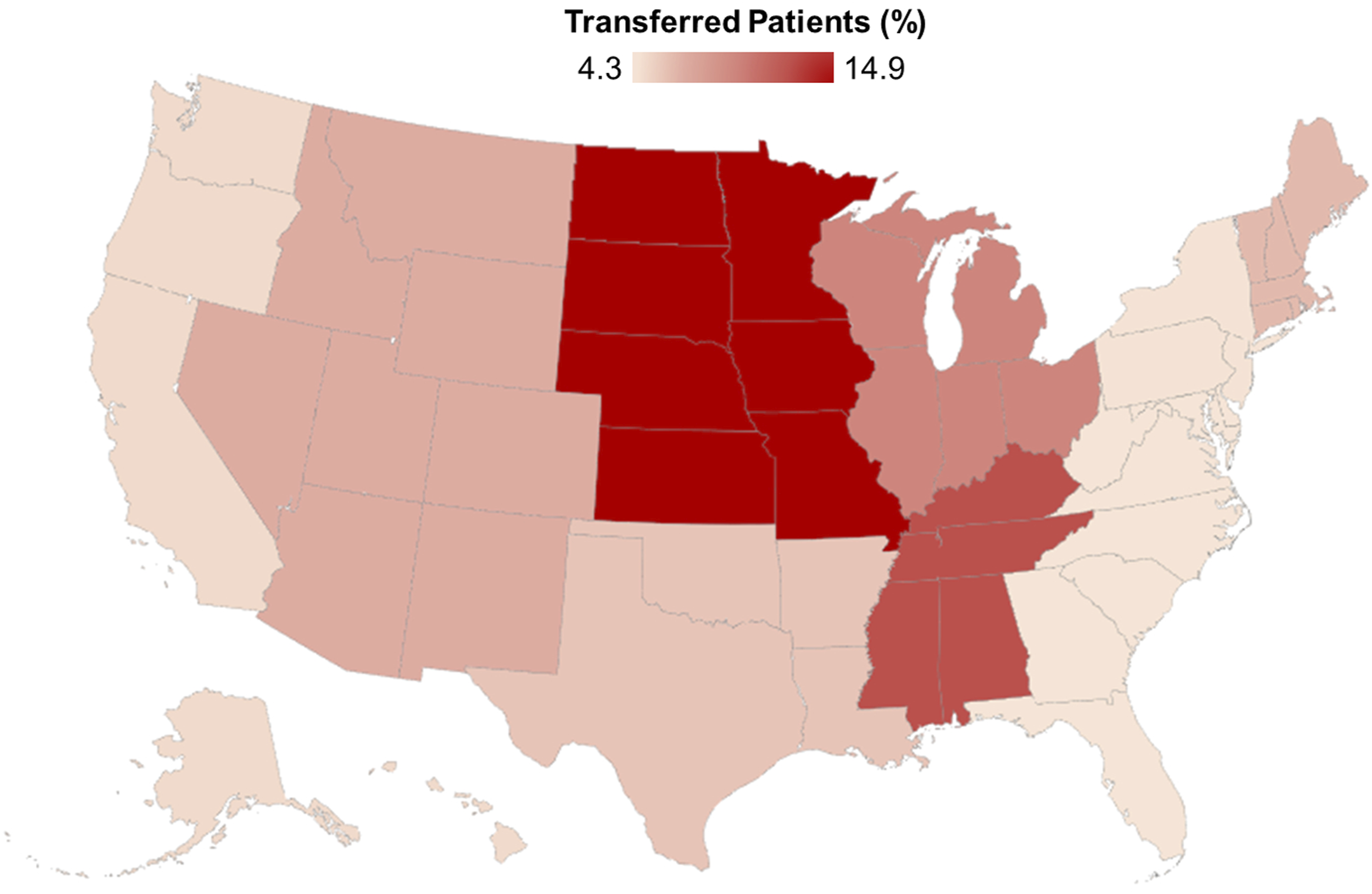
Demographic, Clinical, and Hospital Characteristics.
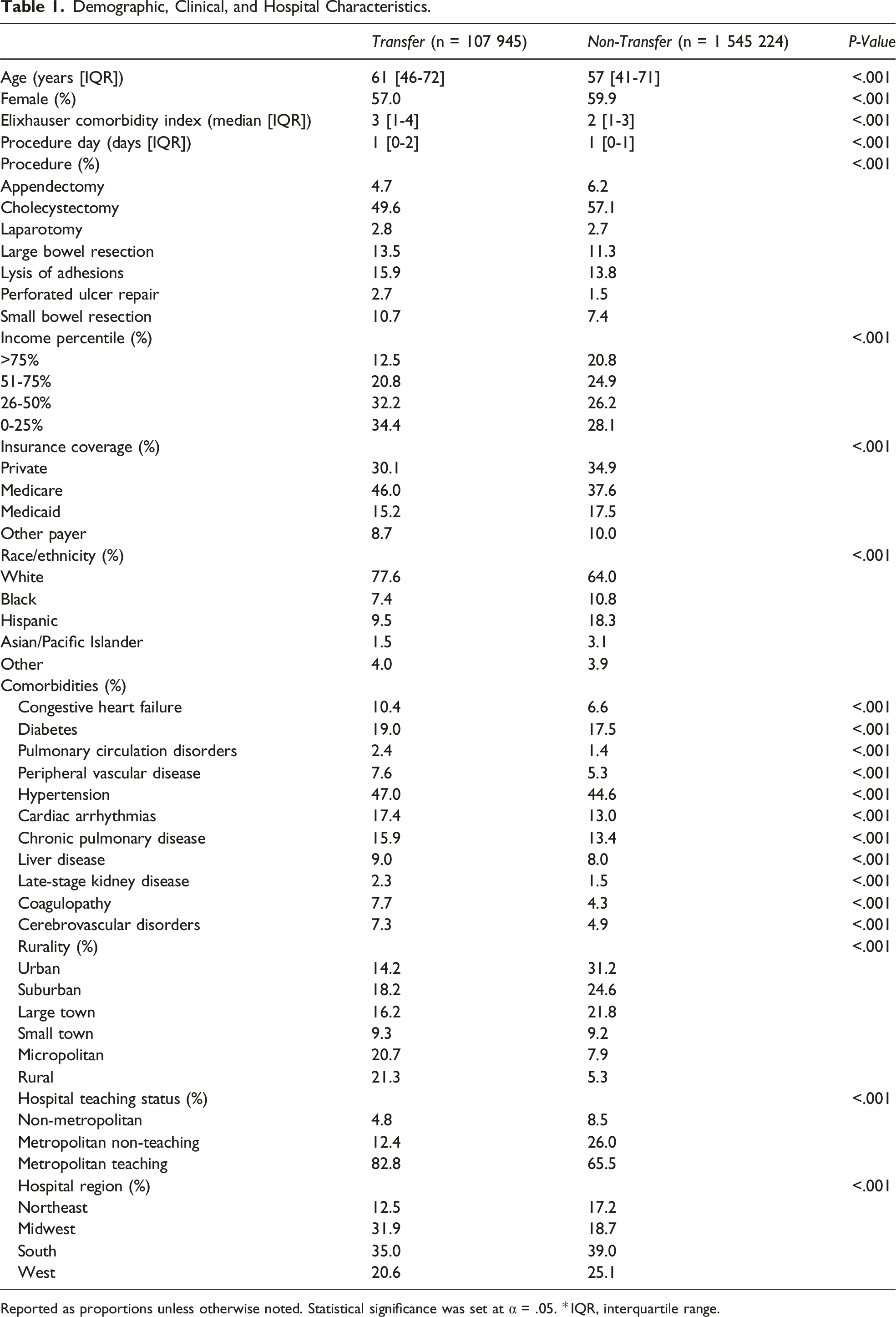
Reported as proportions unless otherwise noted. Statistical significance was set at α = .05. *IQR, interquartile range.
Factors Associated With Transfer
After adjustment, several factors remained independently associated with risk of interhospital transfer (Model C-statistic .76). Indication for small bowel resection (AOR 1.26, CI 1.18-1.34), peptic ulcer repair (AOR 1.62, CI 1.45-1.80), and lysis of adhesions (AOR 1.13, CI 1.06-1.20) were also associated with increased odds of transfer, relative to large bowel resection (Figure 4). Risk-adjusted interhospital transfer rates, stratified by operation. Following risk adjustment, patients requiring peptic ulcer repair (9.6%, CI 8.7-10.4%), small bowel resection (7.7%, CI 7.3-8.1%), lysis of adhesions (7.0%, CI 6.7-7.3%), and large bowel resection (6.3%, CI 6.0-6.6%) faced the highest predicted rates of interhospital transfer. Those with indications for appendectomy (4.8%, CI 4.5-5.1%) and cholecystectomy (6.0%, CI 5.7-6.2%) demonstrated lower predicted transfer rates. *indicates statistical significance at P < .05, with large bowel resection as reference. *LBR, large bowel resection; LOA, lysis of adhesions; SBR, small bowel resection; PU Repair, peptic ulcer repair.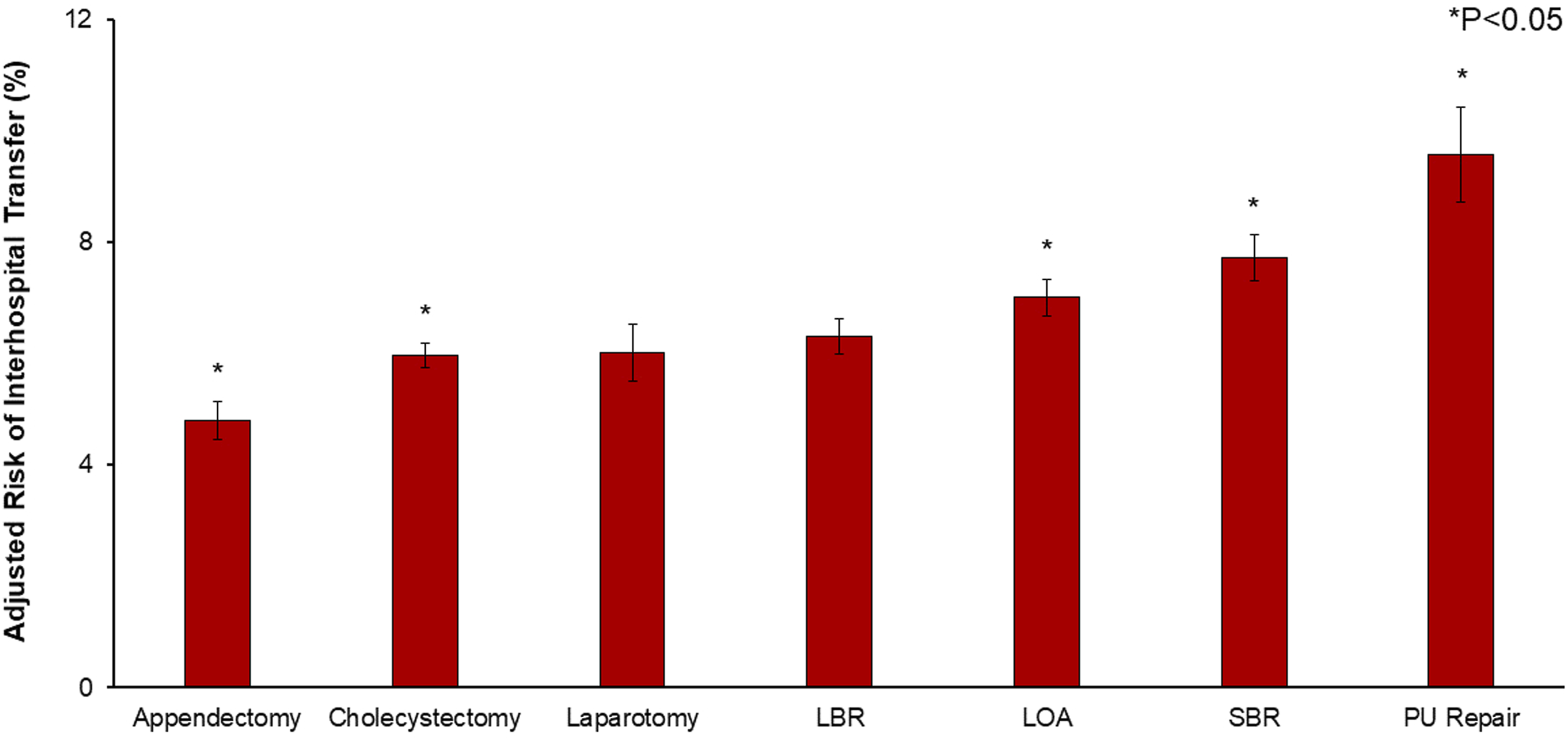
Increasing age and Elixhauser score were linked with greater likelihood of transfer, as was care in the Midwest (AOR 1.54, CI 1.36-1.75) or Western regions (AOR 1.23, CI 1.08-1.39), with Northeast as reference. Further, residence in rural areas was associated with increased odds of transfer (Micropolitan AOR 4.57, CI 4.19-4.98; Rural AOR 7.11, CI 6.50-7.78; Ref: Urban). Black race (AOR .74, CI 0.69-.80) and Hispanic ethnicity (AOR .69, CI 0.64-.75) were also linked with reduced adjusted probability of interhospital transfer, with White race as reference. However, decreasing income quartile was associated with greater transfer odds (Figure 5). Coefficient plot demonstrating factors linked with interhospital transfer. Following risk adjustment, increasing age and Elixhauser index were linked with greater likelihood of transfer. However, Black race and Hispanic ethnicity were associated with reduced odds of transfer, relative to White race. Increasing rurality was linked with significantly increased transfer likelihood, with urban regions as reference. Additionally, care in the Midwest and South was linked with increased relative risk of transfer, relative to the Northeast.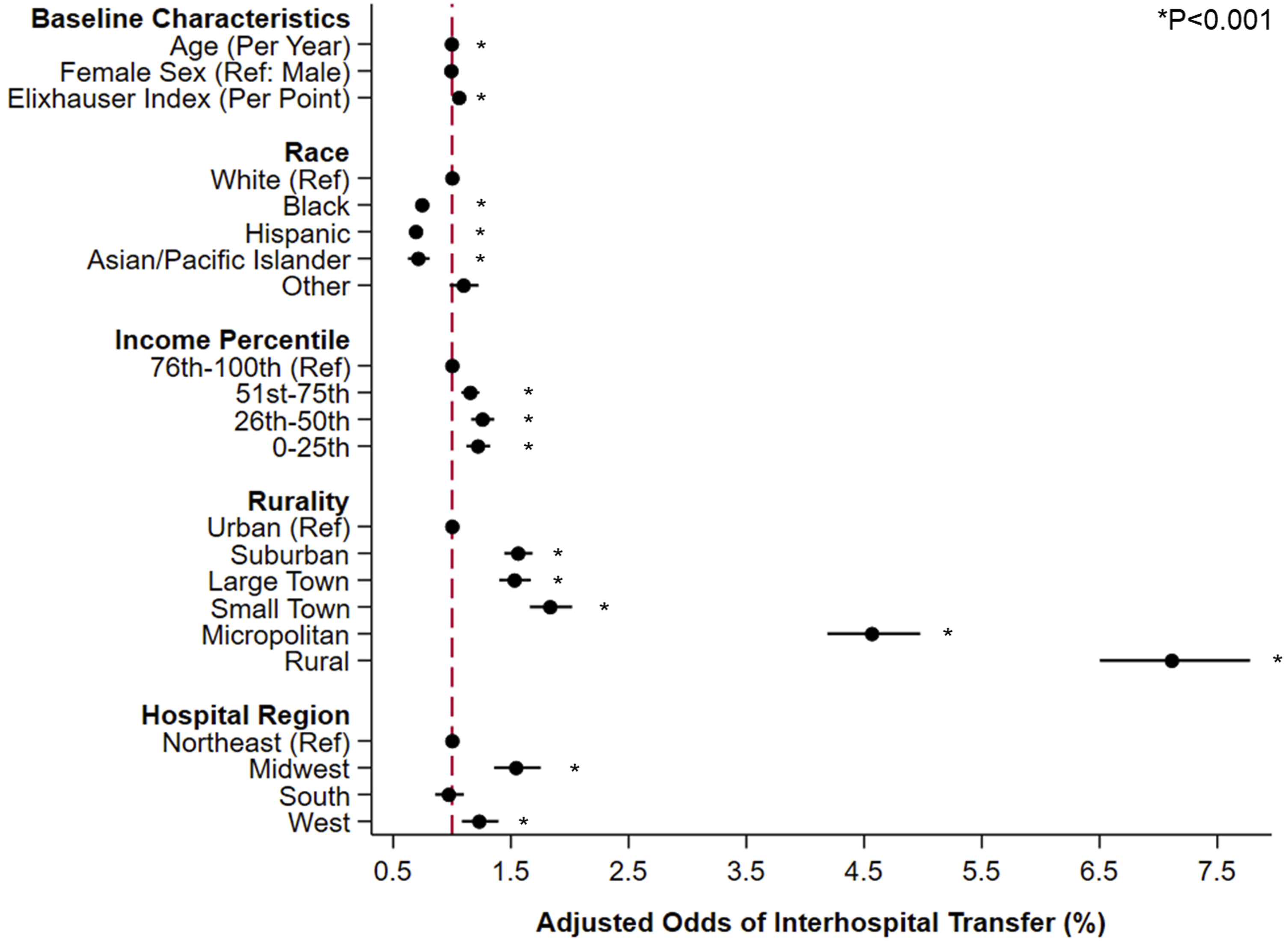
Postoperative Outcomes
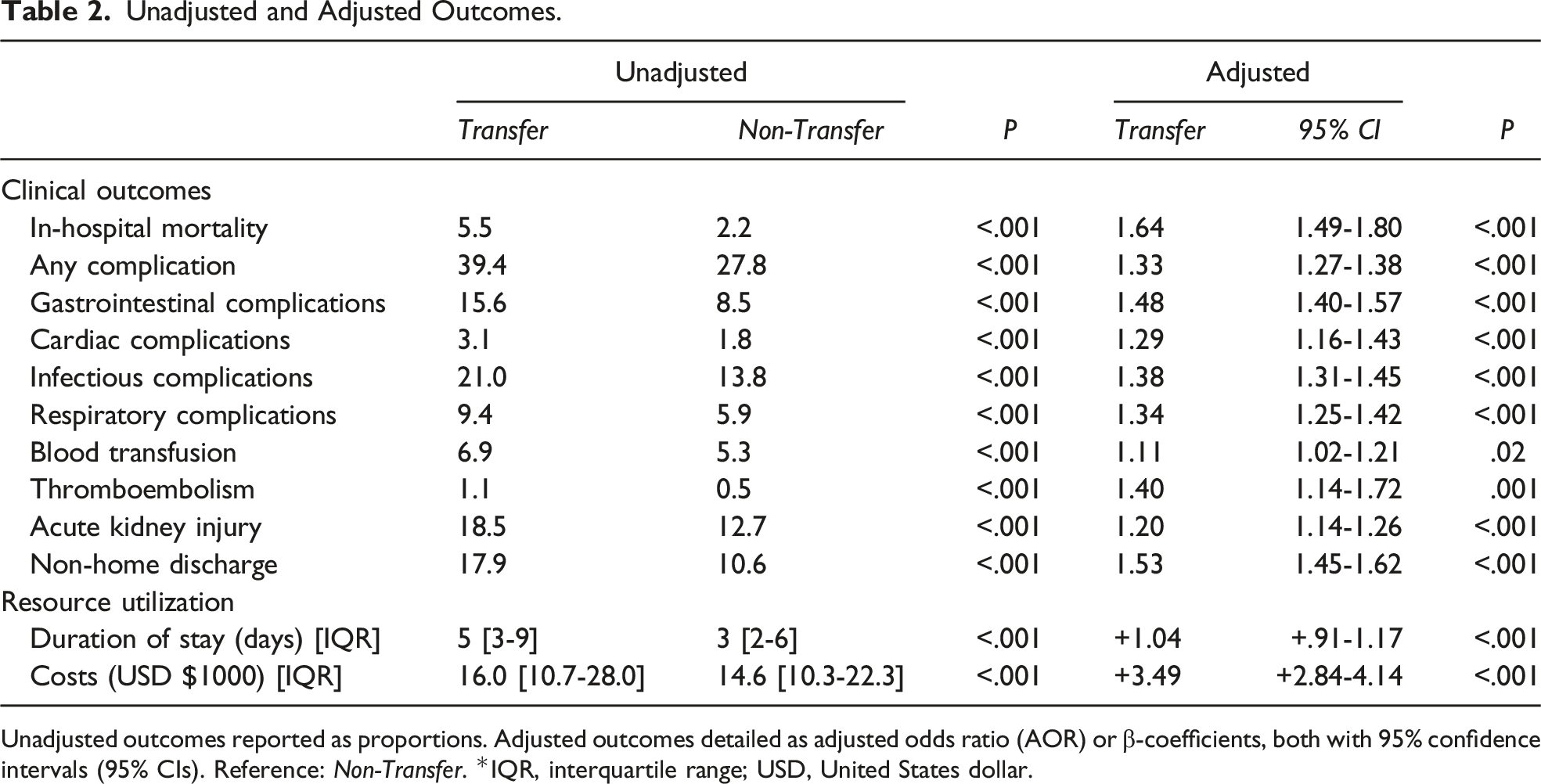
On bivariate comparison, the Transfer cohort exhibited higher rates of in-hospital mortality (5.5 vs 2.2%, P < .001) and postoperative complications (39.4 vs 27.8%, P < .001). In addition, Transfer faced significantly longer LOS (5 [3-9] vs 3 days [2-6], P < .001) and hospitalization costs ($16,000 [10.7-28.0] vs 14 600 [10.3-22.3], P < .001).
Following entropy balancing and risk adjustment, Transfer demonstrated higher odds of in-hospital mortality (AOR 1.64, CI 1.49-1.80; Model C-statistic .90) and any complication (AOR 1.33, CI 1.27-1.38) (Figure 6). Specifically, Transfer had greater likelihood of cardiac (AOR 1.29, CI 1.16-1.43), gastrointestinal (AOR 1.48, CI 1.40-1.57), infectious (AOR 1.38, CI 1.31-1.45), and respiratory sequelae (AOR 1.34, CI 1.25-1.42), as well as acute kidney injury (AOR 1.20, CI 1.14-1.26). Moreover, Transfer remained linked with longer LOS (β + 1.04 days, CI + .91-1.17), greater expenditures (β+$3,490, CI + 2840-4140), and increased odds of non-home discharge (AOR 1.53, CI 1.45-1.62) (Table 2). Adjusted risk of in-hospital mortality and complications, stratified by transfer status and operation. Across all procedures, the Transfer cohort (red) demonstrated increased likelihood of in-hospital mortality (A) as well as greater perioperative complications (B). Patients faced the greatest risk of mortality and complications following peptic ulcer repair (In-hospital mortality: Transfer 11.6 vs Non-Transfer 5.7%; Complications: 55.5 vs 44.1%) and small bowel resection (In-hospital mortality: 9.1 vs 4.3%; 58.6 vs 47.2%). *LBR, large bowel resection; SBR, small bowel resection; PU Repair, peptic ulcer repair; LOA, lysis of adhesions. Unadjusted and Adjusted Outcomes. Unadjusted outcomes reported as proportions. Adjusted outcomes detailed as adjusted odds ratio (AOR) or β-coefficients, both with 95% confidence intervals (95% CIs). Reference: Non-Transfer. *IQR, interquartile range; USD, United States dollar.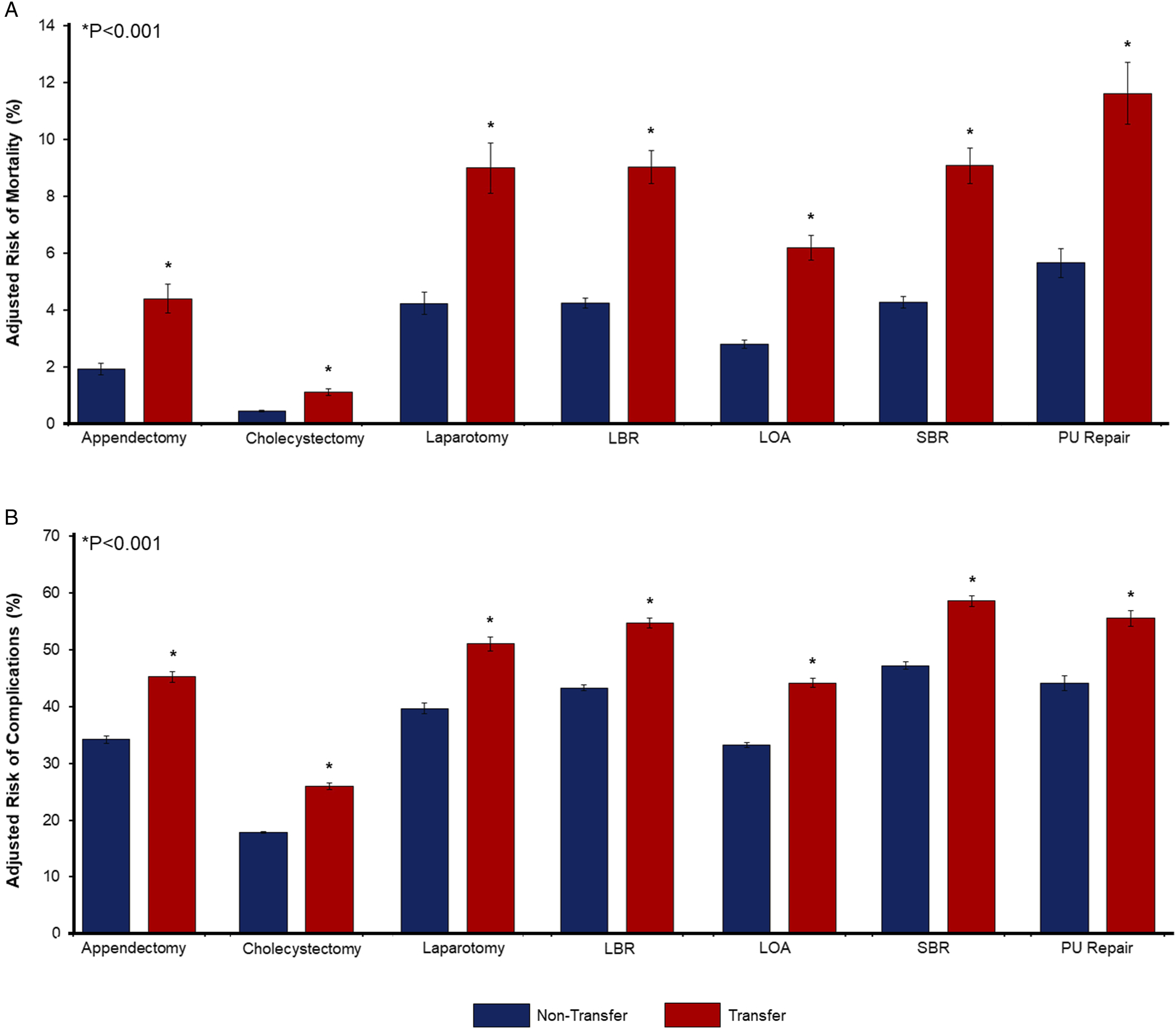
Discussion
In this nationally representative analysis of patients undergoing emergency general surgery, we examined contemporary outcomes associated with interhospital transfer. We noted a growing proportion of patients transferred for surgical management. After risk adjustment and application of covariate balance techniques, interhospital transfer remained linked with greater in-hospital mortality and complications. Lastly, we found transfer to be associated with significantly increased resource utilization. With implications for national policy and practice, several of these findings merit further discussion.
Patients requiring hospital transfer comprise a growing and vulnerable surgical cohort. We found 6.5% of the study population to experience interhospital transfer, with the proportion of such patients significantly increasing from 2016 to 2020. Compared with others, the transfer cohort was more commonly socioeconomically disadvantaged, publicly insured, and of a higher comorbidity burden. As these sociodemographic characteristics have been independently associated with reduced access to high quality care, as well as inferior health outcomes, they may both predicate and augment the risk of transfer. In line with prior work, we also noted transfer patients to be more often of White race. 15 While the aspects underlying this relationship remain to be fully elucidated, some have suggested patients of minority race to be less likely to present to hospitals with streamlined transfer protocols, or face other barriers to specialized surgical care. 16 Further, transfer patients most often resided in rural or micropolitan areas and sought care in Midwestern states. This finding is particularly revealing given current trends in centralization of care. While rural community hospitals continue to serve nearly one-fifth of the U.S. population, the combination of worsening financial circumstances and continued clinician shortages have sharply reduced access to emergency care and comprehensive, on-call surgical services. 17 As such, these smaller often lower-volume centers are significantly more likely to transfer sick and medically complex patients to more specialized and higher volume institutions. 18 Our finding that interhospital transfer remained independently associated with inferior clinical and financial outcomes is likely reflective of the higher acuity of illness among such individuals.
We identified transfer patients to face significantly increased likelihood of in-hospital mortality, as well as the incidence of any perioperative complication. While this group generally represents a higher acuity cohort, relative to non-transfer patients,2,5–8 these associations remained even after applying entropy balancing to address baseline comorbidity differences between groups, and adjusting for relevant patient, hospital, and procedural factors. Whether attributable to increased illness severity or delays in care, the differential in risk associated with interhospital transfer persisted across both low and higher acuity operations. Therefore, clinicians should carefully weigh the risks associated with transfer against the potential benefits of further workup at tertiary referral centers. Given that certain patients will require higher level surgical management, irrespective of any risks, efforts should also focus on enhancing the efficiency of the transfer process. Indeed, in the absence of standardized American College of Surgeons guidelines, in-hospital protocols are needed that expedite recognition of those in need of transfer and communication with accepting providers. 19 Further, specific pathways should be implemented to ensure the sharing of complete laboratory, radiographic, and physiologic records, to reduce the need for duplicate testing and associated delays in definitive treatment.
Lastly, we noted interhospital transfer to be associated with greater resource utilization. Indeed, the transfer cohort demonstrated a ∼1-day incremental increase in duration of hospitalization, as well as ∼$3500 greater per-patient costs. Ultimately, we proffer these additional expenditures may stem from both duplicated testing and the need for more involved care, including respiratory therapy, repeated imaging, increased pharmacy requirements, and admission to the intensive care unit. 2 Of note, transfer patients also demonstrated a ∼53% increase in relative risk of discharge to extended care facilities. Thus, earlier involvement of social work could minimize the need for delayed discharge, and ensure patients and their families have necessary resources and support for continued post-hospitalization care. Importantly, the present resource analysis only evaluates costs at the treating facility and cannot ascertain expenditures incurred at the referring center, or those associated with non-elective readmission. We also could not evaluate uncaptured costs, including travel expenses for family members and the psychological burden of delayed care. With more emphasis on value-based health care delivery in the United States, future studies are needed to comprehensively assess the additional resource burden imposed by interhospital transfer.
Prior studies considering the impact of interhospital transfer on outcomes of EGS have reached conflicting findings but have been limited by international or smaller cohorts, limited sample sizes, or older datasets that restrict generalizability to the contemporary setting.4–8 Allen et al 20 considered 1846 Canadian EGS patients and found transfer to be an independent predictor of postoperative complications, but not mortality. In contrast, Philip et al 6 reported greater mortality and complications, while Lucas et al 4 reported equivalent outcomes among transfer patients. Across these works, the definition of transfer has varied, with some including transfers from nursing homes. 9 Meanwhile, other studies have been confounded by delayed surgery >3 days following admission.6,7,9 In contrast to this literature, the present study utilizes a strict definition for interhospital transfer, considers only operations performed emergently, and applies robust statistical methods and covariate balancing techniques to a nationally representative cohort.
Our work has several important limitations. As a retrospective database, the NIS utilizes ICD coding, which may vary based on clinician, hospital, or regional practices. The NIS does not detail granular laboratory, radiographic, or procedural data, nor does it report patient acuity. Ultimately, all of these factors may influence the decision to transfer a patient. Further, information regarding the transferring facility was similarly unavailable for analysis. Therefore, we could not consider the case volume or teaching status of the referring center. Surgeon availability or experience at either the index or accepting center was similarly not detailed. Lastly, we could not ascertain the time to transfer, which could contribute to greater morbidity. Despite these limitations, however, we applied thorough statistical methodology and evaluated a large, nationally representative cohort to present a comprehensive analysis of interhospital transfer.
In conclusion, we identified a growing cohort of patients experiencing interhospital transfer for EGS. Additionally, we found transfer to be associated with greater mortality, complications, costs, and non-home discharge. Earlier identification of the need for interhospital transfer and improved information sharing across centers could reduce unnecessary delays in care. Future studies should also more comprehensively elucidate the factors contributing to increased patient vulnerability and develop appropriate interventions to improve perioperative outcomes. Finally, given the steady trend toward centralization of care and consolidation of hospitals, national efforts are needed to ensure all patients have access to high quality emergency surgical treatment.
Footnotes
Author’s Note
Presentation: Accepted as a Plenary Presentation at the Southern California Chapter, American College of Surgeons Annual Meeting January 19, 2024 | Santa Barbara, CA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.