
Abstract
Compartment syndrome (CS) is a well-known surgical emergency with high morbidity including potential long-term disability and limb loss. The most important factor determining the degree of morbidity with CS is time to treatment; therefore, early diagnosis and surgery are vital. We present a patient who fell off his bicycle and sustained cervical spine fractures causing near complete quadriplegia. He was found by the road over 12 hours later, so his creatine phosphokinase (CPK) was trended and serial examinations were performed. We identified tight deltoid, trapezius, and latissimus compartments and brought him to the operating room for fasciotomies. Although lab values and compartment pressures can be helpful, they should not guide treatment. It is important to consider atypical sites for CS and complete a head to toe physical examination. Patients should proceed to the operating room if clinical suspicion exists for CS because of the morbidity associated with a missed diagnosis.
Compartment syndrome is a well-known surgical emergency with high morbidity including potential long-term disability, limb loss, renal failure, and death. 1 Increased compartment pressures lead to ischemia which can progress to necrosis and limb loss. Extremity compartment syndrome is usually the result of fractures and most commonly occurs in the calf (∼3.8%) and forearm (1.25%). Compartment syndrome in other parts of the body like the buttock or shoulder is rare often resulting in delayed diagnosis and management. 2 Compartment syndrome can also occur in the abdomen. Although abdominal hypertension is common (∼33%) after aggressive fluid resuscitation, abdominal compartment syndrome is much more rare (∼3%). Early decompression with fasciotomy is the treatment for all compartment syndrome, with earlier time to treatment being associated with better outcomes.1,3
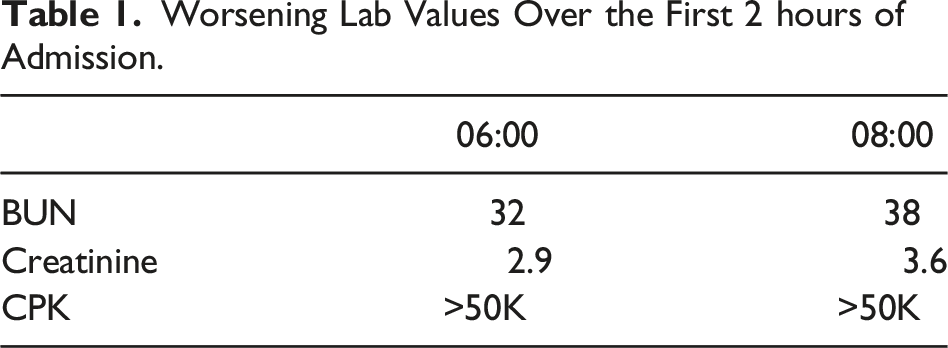
Worsening Lab Values Over the First 2 hours of Admission.
We began our procedure by performing our gluteus fasciotomy. Fasciotomies of the gluteus are much more common than of the shoulder, so we will not go into detail about this part of the procedure. We did, however, find one area of bulging edematous muscle that appeared to have full function. Next, we directed our attention to the right shoulder. We made two curvilinear incisions. The anterior one curved from the lateral clavicle to the deltoid tuberosity. The posterior one ordinarily curves from the anterolateral scapula to the deltoid tuberosity, but on exam, we could feel bulging toward the patient’s back over the trapezius and latissimus dorsi. We therefore began our incision more posterior toward the medial scapula and curved more caudal toward the deltoid tuberosity (Figure 1). Compartments were opened to reveal the trapezius, latissimus dorsi, and deltoid muscles, much of which was bulging and edematous with some appearing slightly dusky. Wound vacs were placed over the fasciotomy sites. Although the patient tolerated the procedure, he did progress to need continuous renal replacement therapy (CRRT) on post op day 1 for correction of acute tubular necrosis and rhabdomyolysis. Traditional incisions for deltoid fasciotomy (left) vs modified posterior incision to release trapezius and latissimus (right).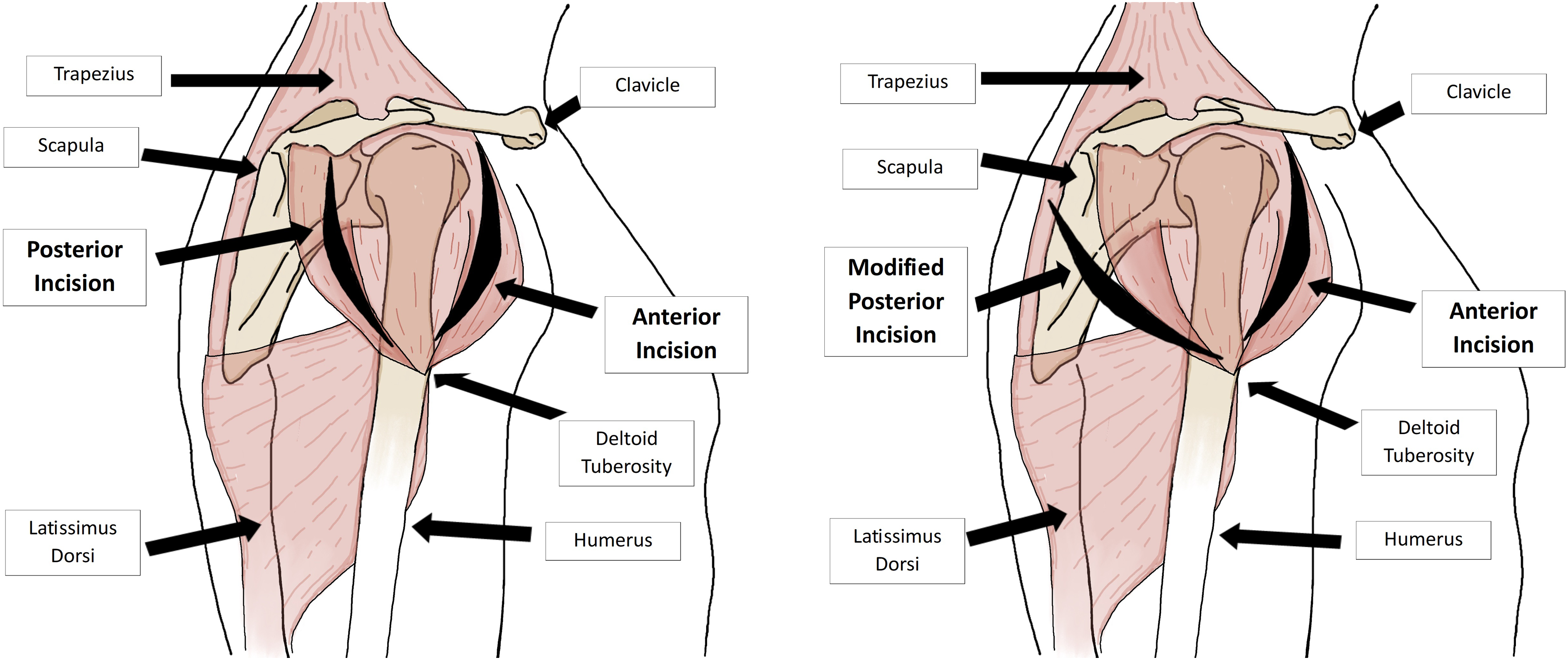
The patient had successful posterior laminectomy and fusion for his spinal cord injury. His subsequent hospital course was notable for failed extubation, hypoxic cardiac arrest with return of spontaneous circulation (ROSC), and DVT. After conversations with family and the palliative care team, he was ultimately discharged to hospice on hospital day 11.
Any time the fluid volume rises within a fixed compartment, the pressure within that compartment will increase. This increased pressure can lead to decreased blood flow, local ischemia, and subsequent anoxia. If untreated, this anoxia can lead to tissue loss, limb loss, end organ dysfunction, or even death. These complications can occur in as early as 3-4 hours. Common sites include the leg, forearm, and abdomen, but it can also occur anywhere with enclosed fascial compartments. Given that the fascia of the deltoid, trapezius, and latissimus are more compliant than other compartments, they are able to tolerate more muscular swelling without compartmental pressure changes and as such require a much greater level of insult to develop compartment syndrome. 2 The literature is essentially absent on recommendations for the treatment of compartment syndrome in these areas, most notably the trapezius and latissimus. A few scattered cases describe compartment syndrome in these locations either as a result of intense athletic activity or after surgical procedures. 4 A review by Scollan et al focusing on acute compartment syndrome of the deltoid showed that the majority of cases were due to prolonged recumbency as was seen in our patient. Other less common causes include intramedullary nailing of humeral fractures, intramuscular injections, revascularization after aortic dissection, severe extremity trauma (such as long bone fractures and crush injury), arterial injury, prolonged ischemia with reperfusion, massive transfusion, burns, SIRS. 2
Given the rarity of compartment syndrome of the shoulder and even more so of the back, both can be easily missed. In the case of our patient, the elevated CPK level and myoglobinuria which did not improve with fluid resuscitation raised our index of suspicion for compartment syndrome, prompting us to do a thorough reexamination of the patient during which we identified tight compartments of his left gluteus, right shoulder, and right back. Based on our examination in the operating room, muscles in all 3 places were becoming compromised, with the shoulder and back being the worst.
The traditional teaching of the 5Ps (pain, pallor, pulselessness, paresthesias, and paralysis) for compartment syndrome is more indicative of arterial compromise which can occur late in the development of compartment syndrome.1-3 Pain out of proportion of exam or with passive range of motion is more suggestive of compartment syndrome. Although measurement of compartment pressures with calculation of Delta P (normal Delta P = diastolic pressure-compartment pressure= <20 mmHg) or serial CPK (normal = CPK <5000) levels can be helpful, compartment syndrome remains a clinical diagnosis. Urgent surgical intervention should never be delayed in order to obtain compartment pressures or laboratory results. 1 If patients present with either a concerning mechanism or initial exam, serial examinations with calculation of Delta P should be performed. Although trending CPK can be helpful, there is no real evidence to support trending serum creatinine, urine myoglobin, or serum lactate. Despite this, serum creatinine and lactate can be trended based on trauma resuscitation guidelines.
The complications associated with acute compartment syndrome can be avoided by early diagnosis and appropriate treatment. The goal is to decompress all affected muscle compartments by performing fasciotomies thereby relieving pressure on and anoxia of nerves and vessels. 1 Although this anoxia can occur in as early as 3-4 hours, irreversible damage can occur after 8 hours, and delays beyond this can lead to infection, amputation, or death. 1 Surgeons are trained to consider compartment syndrome in distal upper and lower extremities, but it is important to remember that it can occur anywhere. Maintaining a low threshold to reexamine patients and to go to the operating room because of any concerning findings can preserve patients’ functional outcomes and possibly their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.