
Abstract
Objectives
While insufficient code status documentation (CSD) is a longstanding challenge, all patients deserve the opportunity to participate in decision-making regarding code status, especially trauma patients with an unpredictable course. Prior interventions to increase CSD relied on reminder systems. We hypothesize that introducing a daily checklist will increase CSD for patients in the trauma ICU.
Methods
This quality improvement study examined the efficacy of a twice-daily checklist for improving CSD in trauma patients at a level I trauma center. A pre-intervention (PRE) and post-intervention (POST) daily census characterized the percentage of patients with CSD (primary outcome), time-to-code status (TTCS, secondary outcome) documentation, and information about patients who were discharged with no code status (DNCS, secondary outcome).
Results
Of 213 PRE and 207 POST, daily census CSD for all patients increased from a median of 50.0% PRE to 64.4% POST (P < .05). Time-to-code status was halved (PRE: 25.30 h, POST: 12.71 h, P < .05). Code status documentation within 12 h increased from 41.8% PRE to 60.9% POST (P < .05). Overall, the percentage of patients with CSD during their hospitalization increased 20% (PRE: 63.8%, POST: 83.6%, P < .05). Discharged with no code status patients decreased 20% (PRE: 35.2%, POST: 15.5%, P < .05).
Conclusion
Including code status in a daily checklist involving key aspects of care for trauma patients is an effective method for improving code status documentation. Capturing code status for more patients in trauma allows us to provide patient-centered, goal-concordant care.
Introduction
Insufficient code status documentation (CSD) has been a longstanding challenge in hospitalized patients. Code status discussions can be difficult and uncomfortable, and these prohibitive factors are heightened in the emergency setting. Trauma patients may be unstable, lack capacity, or not have surrogates available to help with decision-making. In addition to these challenges, the perception that patients are either too young or too sick has been cited as a barrier to CSD in trauma patients. 1
Despite these challenges, all patients deserve the opportunity to participate in decision-making regarding end-of-life wishes, especially patients with an unpredictable course such as in the trauma ICU. Further, the American College of Surgeons Trauma Quality Improvement Project recommends documentation of code status within 24 h of admission for trauma patients. 2 Prior interventions to increase CSD have relied on communication skills training, email reminders, and materials posted in patient rooms.1,3 These studies suggest that reminders to obtain code status are effective at increasing CSD, but these interventions relied on individual effort for maintenance.
The purpose of this study was to identify the efficacy of a twice-daily checklist for the improvement of code status documentation in trauma patients. We hypothesize that building reminders to obtain and document code status into pre-existing daily routines in the form of a checklist would increase CSD for patients in the trauma population.
Material and Methods
IRB Approval
This quality improvement study was exempted from the institutional review board review.
Study Design
This prospective quality improvement study examined the efficacy of a twice-daily checklist (Figure 1) used during morning and evening rounds for improving CSD in adult trauma patients at a level I trauma center from March to April of 2023. All patients admitted to the trauma service received this intervention. The checklist includes key information about a patient’s care and progression on the trauma service: oxygen details, diet recommendations, if a patient has voided and/or had a bowel movement, if they are on the appropriate prophylactic medications, disposition recommendations, and CSD status. During morning and evening rounds, residents and APPs verbally completed the checklist, stating the status of each category on the checklist aloud, ending with code status. Implemented checklist.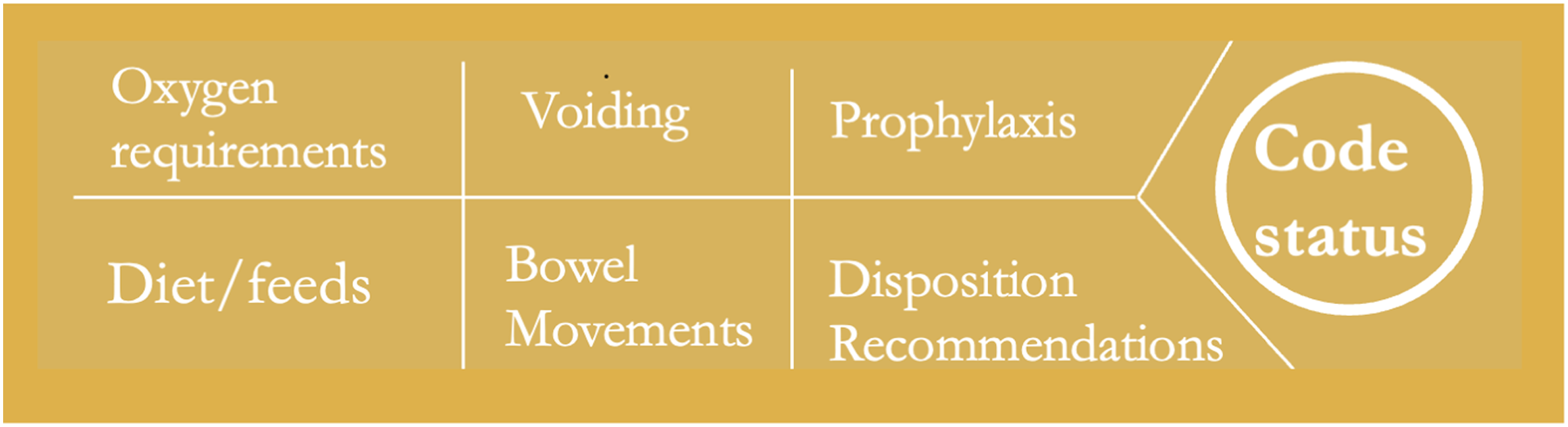
An example script reads as follows: the patient is on 2 liters of nasal cannula, has a regular diet, has a foley, last bowel movement was two days ago, is on appropriate prophylaxis, is recommended for IPR, and does not have code status documented.
Pre-intervention (PRE) and post-intervention (POST) data were gathered through a daily census characterizing the percentage of patients with CSD (primary outcome), documentation of time-to-code status (TTCS, secondary outcome), and information about patients who were discharged with no code status (DNCS, secondary outcome). The daily census CSD data was reported as a daily percentage of patients in the trauma ICU and trauma step-down unit with completed code status orders. Time-to-code status or time to DNCS was defined as the time of arrival to the emergency department to the time of code status order or discharge, respectively. Patient details including age and preferred language were recorded from the electronic health record (EHR).
Statistical Analysis
Analysis was performed using R Studio Team. R Studio: Integrated Development for R. Version 2023.03.0+386 (2023.03.0+386) R Studio, PBC, 2022. https://www.rstudio.com/. Univariate analysis was performed with chi-squared and t test for categorical and continuous data, respectively.
Results
Results.
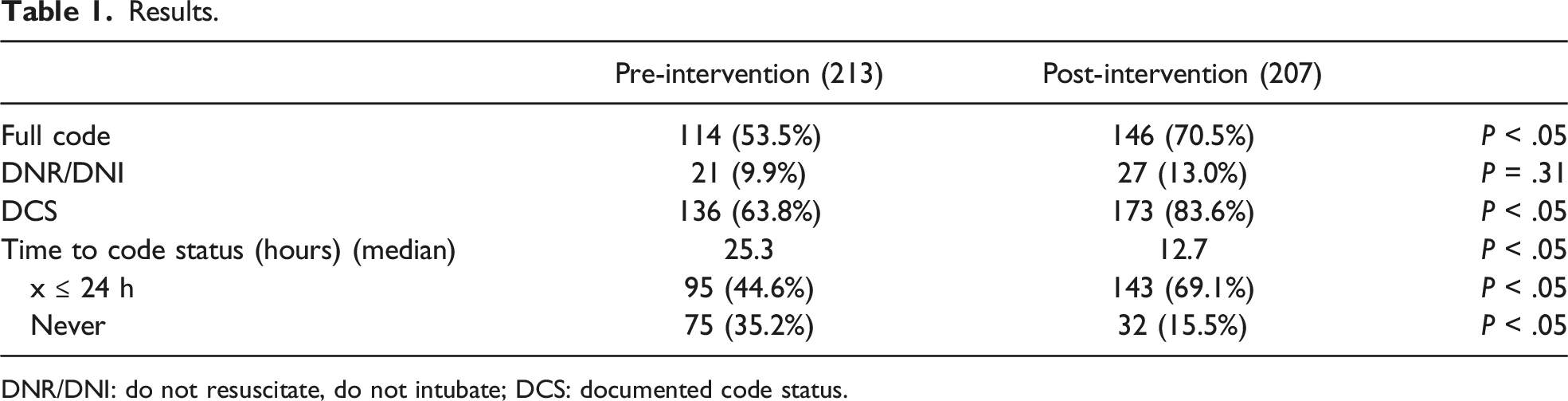
DNR/DNI: do not resuscitate, do not intubate; DCS: documented code status.
Discussion
Our data upholds that including code status in a daily checklist involving key aspects of care for trauma patients is an effective method for improving code status documentation. This intervention both increased the number of patients who were able to participate in code status decision-making and decreased the time it took for code status orders to be entered, improving overall documentation by 20% during our data collection period and halving the TTCS for all patients. This method takes approximately 20 sec to complete per patient and is minimally disruptive to workflow.
This study is not without limitations. Residents and APPs were aware that code status rates were being analyzed, potentially inflating the rate of compliance with CSD recommendations during the study period. Additionally, this study was completed over a short period and further studies analyzing the staying power of this method have not been completed. Another challenge of this study is that it was only implemented in one department, limiting the generalizability of these results.
We conclude that this checklist system is an effective intervention to improve CSD in the trauma population. Our data strongly supports that providers remembering to engage in code status conversations is a key barrier to its documentation, and the implementation of a self-sustaining reminder system in busy services may be a feasible method for improving patient-centered, goal-concordant care. We look forward to future studies implementing similar checklists in other departments, those addressing additional barriers to CSD, and work on the maintenance of this system in our department.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.