
Abstract
Background
The experiences of pager use among trainees across medical specialties is underexplored. The aim of this study was to assess experiences of pager burden and communication preferences among trainees in different specialties.
Methods
An online survey was developed to assess perceived pager burden (eg, pager volume, mistake pages, sleep, and off-time interruptions) and communication preferences at a tertiary center in the United States. All residents and fellows were eligible to participate. Responses were grouped by specialty: General surgery [GS], Surgical subspecialty [SS], Medicine, Anesthesiology, and Psychiatry. Multivariable linear regression was used to assess factors associated with pager burden. Free text responses were analyzed using open coding methods.
Results
Of the total 306 responses, the majority were female (58.8%), 30-39 years (59.2%), and White (70.6%). Specialty breakdown was: Medicine (40.2%), Psychiatry (10.8%), SS (18.0%), GS (5.6%), and Anesthesiology (3.6%). GS respondents reported receiving more mistake pages (P < .001), spending more time redirecting mistake pages (P = .003), and having the highest sleep time disruptions (P < .001). For urgent communications, surgical trainees preferred physical pagers, while nonsurgical trainees preferred smartphone pagers (P = .001). “Receive fewer nonurgent pages” was the most common change respondents desired.
Discussion
In this single center study, subjective experiences of pager burden were disproportionately high among GS trainees. Reducing nonurgent and mistake pages are potential targets for improving trainee communication experiences. Hospitals should consider incorporating trainee preferences into paging systems. Additional studies are warranted to increase the sample size, assess generalizability of the findings, and contextualize trainee experiences with objective hospital-level paging data.
Key Takeaways
• Subjective experiences of pager burden were disproportionately high among GS residents, who not only reported a higher number of pages and sleep or off-work interruptions, but also more frequent mistake and nonurgent pages. • Preferences for urgent communication methods differed across specialties with surgical trainees preferring physical pagers and nonsurgical trainees preferring smartphone-based paging. • Health systems should incorporate trainee preferences as they develop new communication systems.
Introduction
Pagers are a convenient, fast, and reliable way to communicate with health care professionals. Yet, studies have documented the burden associated with pagers, including high volumes of nonurgent pages,1-3 flow disruptions which can increase the risk of errors,4,5 interrupt patient care,6,7 educational activities,6,8 and lead to decreased sleep and greater fatigue. 9 Furthermore, communication through paging systems is often not standardized and risks violating HIPAA.7,10 To address these issues, hospitals have trialed new methods for streamlining paging systems. These include protocols to reduce the volume of nonurgent pages, particularly at night.11,12 Smartphone-based communication has also become more common, though ongoing challenges persist with maintaining confidentiality on personal devices. 13
The impact of pager burden on physicians across medical specialties, especially in the context of a hybrid paging system with traditional alphanumeric and smartphone-based pagers, is underexplored. In this study, we sought to evaluate the subjective experiences of pager burden among trainee physicians across medical specialties. We defined pager burden as the volume of pages received, mistake pages and time spent redirecting mistake pages, as well as sleep and off-time interruptions due to pages. Additionally, we sought to evaluate trainee communication preferences and obtain suggestions for paging system improvement. We hypothesized that subjective experiences of pager burden would be higher among surgical trainees compared to nonsurgical trainees, but that communication preferences would not differ across specialties.
Materials and Methods
Study Design and Population
All trainee physicians, who used a paging system, at a single tertiary center in the Southeast United States were eligible to participate. This study institution is a public, academic medical center that serves as a safety net hospital for the state. The primary campus where most residents and fellows complete their training is a 1000-bed facility and provides care to approximately 37,000 patients annually. There are additional inpatient and affiliate hospitals, ambulatory centers, and outpatient facilitates where trainees may complete part of their training. In total, the hospital system serves 800,000 patients annually. While each service and specialty operate differently, many training programs practice graduated autonomy. In-house vs home call varies across services, but most surgical services take in-house call during the junior years and home call in the senior years and as fellows.
This study was determined exempt by the University of North Carolina Institutional Review Board (#22-1122) and operated under a waiver of informed consent.
Survey Design and Pilot
Survey experts at the Odum Institute for Research in Social Science were consulted for survey development. The survey was anonymous and included 41 items (Appendix 1). Trainee experiences of pager burden was evaluated by asking the average number of pages received during a scheduled shift during the daytime, at home (not on call), during night call, and the perceived urgency of the pagers received during the day, while on home call, and during night shifts. Average number of mistake pages was assessed by the number of times an individual received “a page that is intended for someone else,” followed by a question about the average time (in minutes) spent redirecting those pages. Sleep and off-work (ie, personal time) disruptions due to pagers were assessed on a Likert scale. Pager burden was also assessed with the question, “In the last year, how often have you felt the volume of pages you received was too much for you to handle?”
Communication preferences for urgent and nonurgent messages were assessed with the following options: Electronic medical record (EMR) chat, EMR message (ie, Epic in-basket), Face-to-face conversation, Pager (smartphone application), Pager (physical), Personal text, Phone call, and Other. Desired change was assessed with a multiple-choice question, including an option for “Other” followed by a free text box. There was an open-ended question for sharing pager experiences at the end. The survey concluded with demographic questions, including self-identified race/ethnicity, gender, and age. Post-graduate year (ie, PGY) level was not obtained to avoid potential identification of trainees (eg, there is only 1 resident per PGY in certain surgical subspecialties).
The survey was piloted with a demographically diverse cohort of ten students, trainees, and faculty physicians from 7 different specialties randomly recruited by email. Feedback was solicited, and a finalized survey was tested by the research team.
Survey Administration
The survey was administered through an online platform (Qualtrics XM, Provo, UT). Participants were recruited by email using a listserv of all residents and fellows. Three emails were sent in June 2022: an initial email and 2 reminders sent 1 week apart. Participants could enter a $100 gift card drawing after survey completion. Email addresses were stored separately from the data.
Statistical Analysis
Categorical variables were presented as counts (percentage), continuous variables were presented as mean (standard deviation), and Likert data were presented as median (interquartile range). Analysis was performed using chi-squared tests for categorical variables and t-tests or analysis of variance tests (ANOVA) for continuous variables. Three multivariable linear regression were used to analyze factors associated with (1) average day shift pages, (2) average night call pages, and (3) average mistake pages. All models controlled for statistically significant covariates (P = .1 used as cutoff for selection) which included age, race, specialty, and training stage (resident vs fellow). Categories for medical specialties are summarized in Appendix 2. Statistical significance was set at P < .05 for all analyses. Stata 15.1 (StataCorp LP, College Station, TX) was used for all analyses.
Open-Ended Responses
Free responses were formatted in an encrypted spreadsheet (Microsoft Excel, 2019, Version 16, Redmond, WA: Microsoft Corporation). Short, free text responses were collected and analyzed by one member of the research team (YI), using open coding methods, grouping responses by common themes. 14 A second member (TMC) was consulted to assist with verification of themes. Exemplary quotes were selected after themes were identified.
Results
Participant Characteristics.
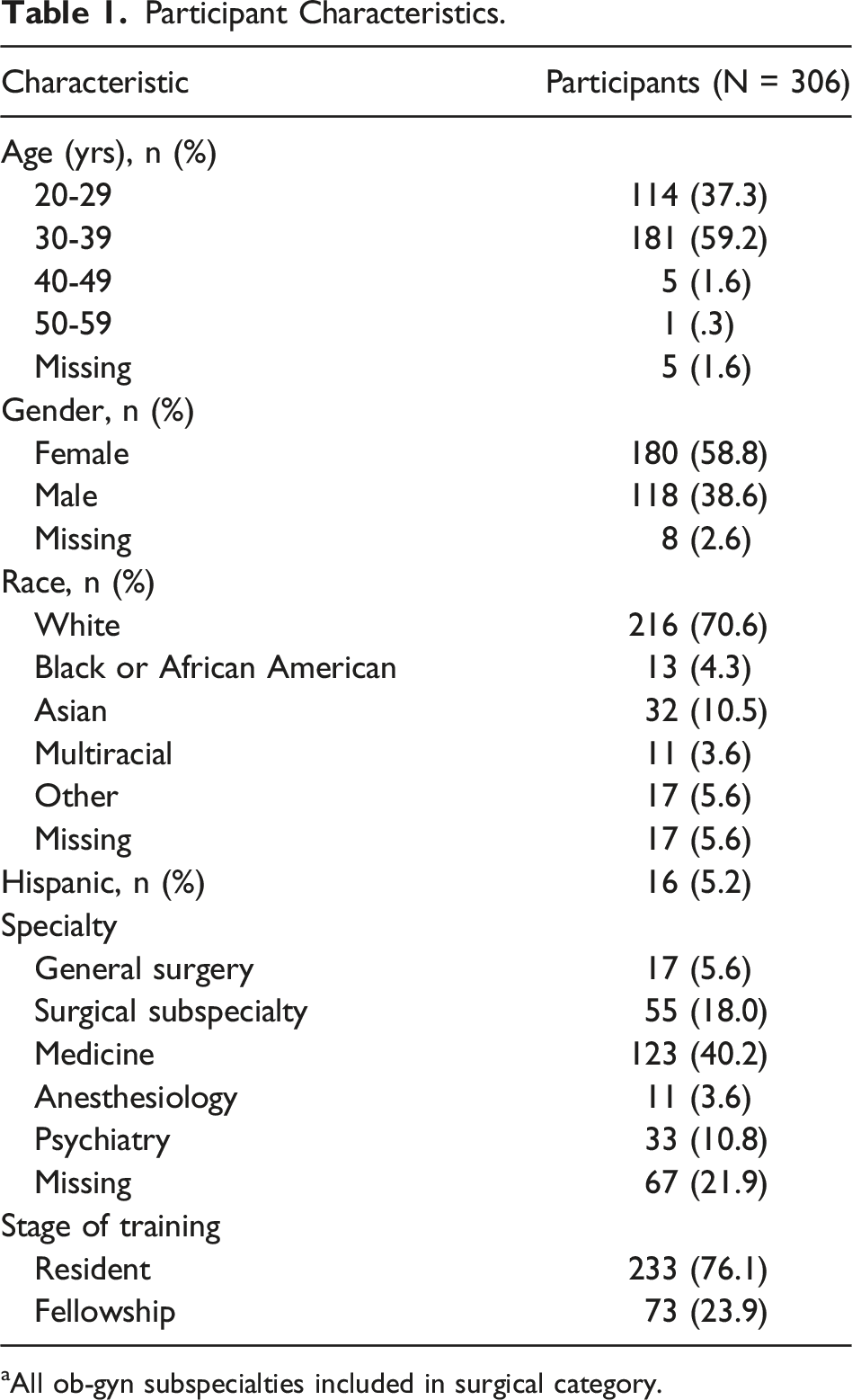
aAll ob-gyn subspecialties included in surgical category.
Pager Burden Outcomes Across Specialties
Perceived Pager Burden by Demographics and Specialty.
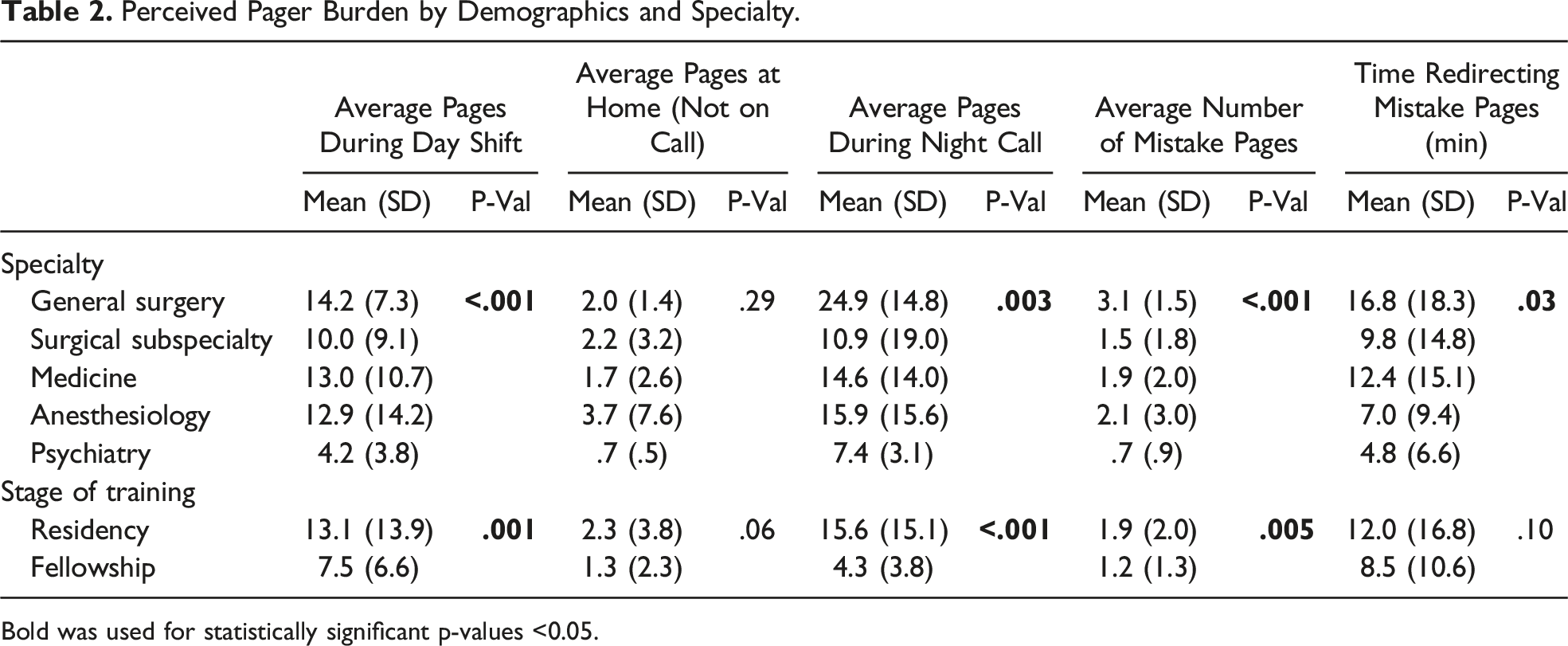
Bold was used for statistically significant p-values <0.05.
GS respondents reported receiving more mistake pages (mean (SD), 3.1 (1.5)), compared to respondents in SS (1.5 (1.8)), medicine (1.9 (2.0)), anesthesiology (2.1 (3.0)), and psychiatry (.7 (.9); all P < .001; Table 2). Additionally, GS trainees reported spending more time redirecting mistake pages GS (16.8 (18.3)), compared to medicine (12.4 (15.1)), SS (9.8 (14.8)), anesthesiology (7.0 (9.4)), and psychiatry (4.8 (6.6); all P = .03). GS respondents were more likely to report sleep time interruptions compared to all other groups (all P < .001). There was no difference in off-time (ie, personal time outside of work) interruptions across specialties. When asked how often the volume of pages was “too much to handle,” individuals in SS and psychiatry were less likely to report the volume of pages was too much handle compared to those in GS, medicine, and anesthesiology (P = .02).
On multivariable analysis, compared to GS respondents, psychiatry respondents had lower average day shift pages (OR = −9.24 [CI −14.91 to −3.58]; P = .002; Figure 1A). There were fewer average night call pages for SS (OR = −10.31 [CI −18.49 to −2.14]; P = .01) and psychiatry (OR = −15.93 [CI −24.60 to −7.26]) respondents compared to GS (P < .001; Figure 1B). There were also fewer average mistake pages received by individuals in SS (OR = −1.41 [CI −2.46 to −.35]; P = .009), medicine (OR = −1.06 [CI −2.04 to −.07]; P = .04], and psychiatry (OR = −2.21 [CI −3.32 to −1.10]) compared to GS (P < .001; Figure 1C). (A) Forest plot of demographic factors associated with average day shift pages. (B) Forest plot of demographic factors associated with average night call pages. (C) Forest plot of demographic factors associated with average mistake pages.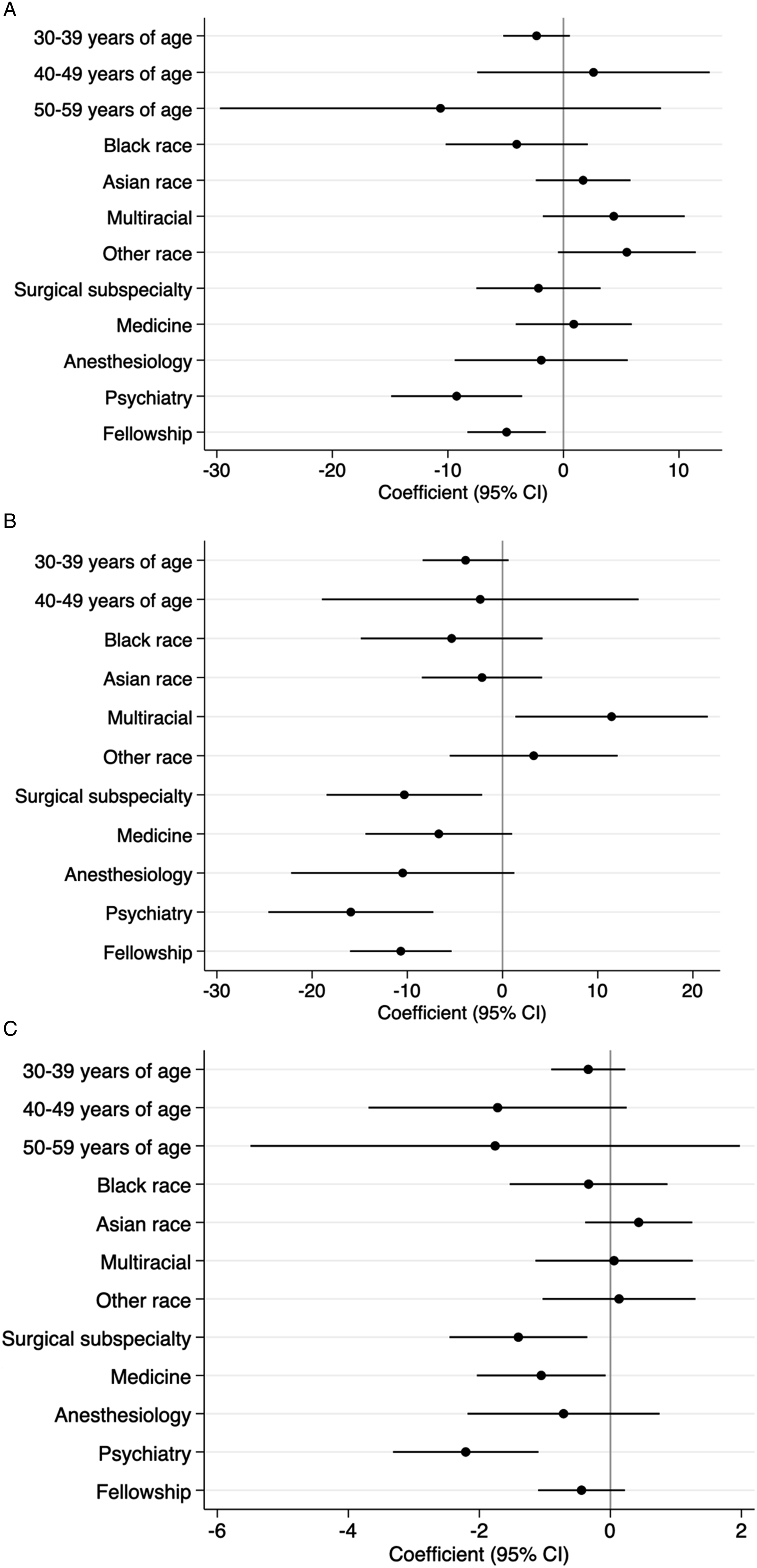
Communication Preferences
Communication preferences differed for urgent vs nonurgent messages. For urgent communications, individuals in surgical specialties (GS, SS) were more likely to prefer physical pagers compared to trainees in nonsurgical specialties (66.7% surgical vs 37.1% nonsurgical). Trainees in nonsurgical specialties were more likely to prefer smartphone pagers (18.1% surgical vs 44.3% nonsurgical; all P = .001; Figure 2A). When comparing across specialties, physical pagers were more frequently preferred by individuals in GS (82.64%) and SS (61.8%) compared to those in psychiatry (51.5%), medicine (35.0%), and anesthesiology (18.2%; all P = .003). Contrarily, smartphone paging was more frequently preferred by individuals in medicine (45.5%), anesthesiology (45.5%), and psychiatry (39.4%) compared to those in GS (0%) and SS (23.6%; all P = .003). For non-urgent messages, both surgical and nonsurgical trainees commonly preferred EMR chat (52.8% surgical vs 70.7% nonsurgical; Figure 2B). (A) Pie chart of urgent communication preferences by surgical vs nonsurgical trainees. (B) Pie chart of nonurgent communication preferences by surgical vs nonsurgical trainees.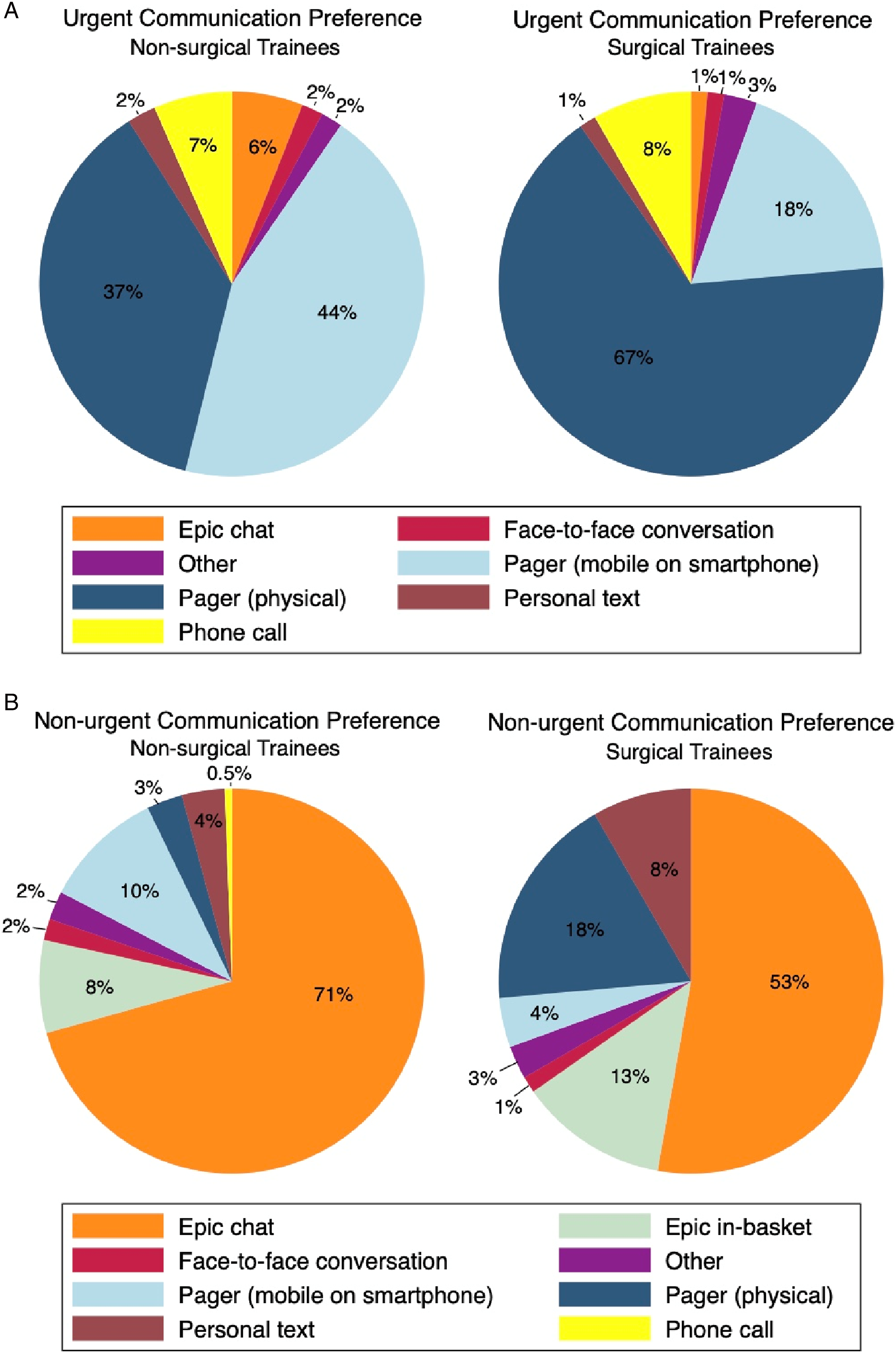
Desired Pager Change
When asked “if you could change one thing about pagers, what would it be?” differences were appreciated across specialties (P = .004). Among GS respondents, 50.0% indicated “Receive fewer nonurgent pages” and 37.5% indicating “Receive fewer pages intended for someone else.” Among SS respondents, 46.3% indicated “Receive fewer nonurgent pages,” followed by 13.0% indicating “Receive fewer pages intended for someone else” and “Other.” Of medicine respondents, 48.8% indicated “Receive fewer nonurgent pages,” 12.2% indicated “Everyone use the same physical paging device,” or “Other.” For anesthesiology respondents, 36.4% indicated “Receive fewer nonurgent pages” and 27.3% indicated “Everyone use the same physical paging device.” For psychiatry respondents, 45.5% indicated “Receive fewer nonurgent pages.” Among SS respondents who indicated “Other,” the most common free response was to “receive a work cell phone.” For medicine respondents, the most common “Other” preference was for the “ability to respond to pages directly through a text” and “be able to send a written response to pages in the app.”
Illustrative Quotes for Paging System Changes.
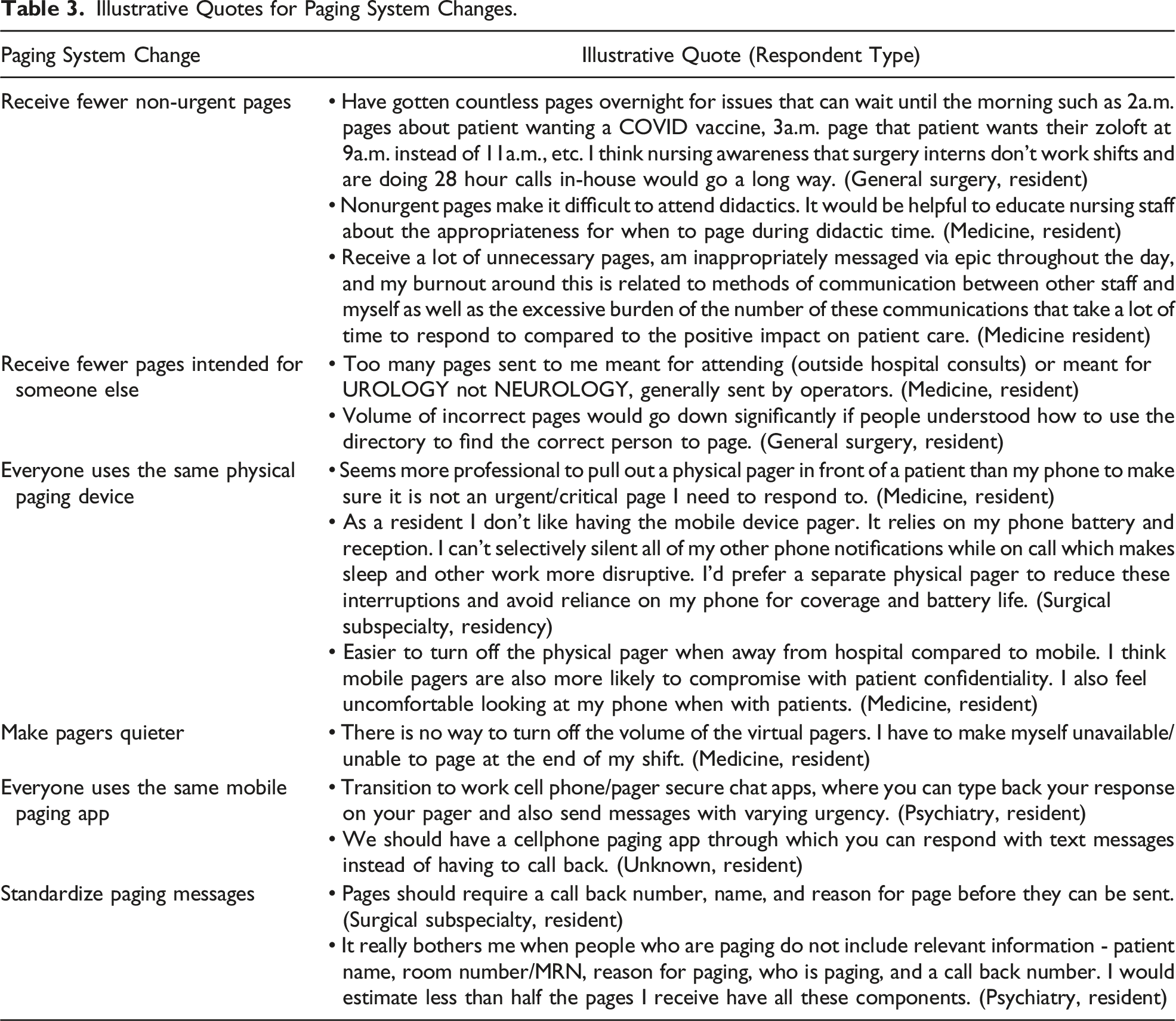
Other trainees discussed their desire for everyone to use the same physical paging device. Reasons for this desired change varied but were not limited to professionalism (“Seems more professional to pull out a physical pager in front of a patient than my phone”) and work-life separation (“Easier to turn off the physical pager when away from hospital compared to mobile. I think mobile pagers are also more likely to compromised with patient confidentiality”). One SS resident captured the complexity of using their personal device in their response: “As a resident I don’t like having the mobile device pager. It relies on my phone battery and reception. I can’t selectively silence all of my other phone notifications while on call which makes sleep and other work more disruptive. I’d prefer a separate physical pager to reduce these interruptions and avoid reliance on my phone for coverage and battery life.”
On the other hand, some trainees wrote about their desire for everyone to use the same mobile paging system. For example, one psychiatry resident emphasized the ability to triage according to urgency, “Transition to work cell phone/pager secure chat apps, where you can type back your response on your pager and also send messages with varying urgency.” Another resident of unknown specialty also spoke about wanting a mobile application in “which you can respond with text messages instead of having to call back.”
Finally, trainees wrote about their desire for a standardized messaging format to improve communication. One SS resident wrote, “Pages should require a call back number, name, and reason for page before they can be sent.” A psychiatry resident wrote about their frustration with inconsistent messaging as well: “It really bothers me when people who are paging do not include relevant information—patient name, room number/MRN, reason for paging, who is paging, and a call back number. I would estimate less than half the pages I receive have all these components.”
Discussion
In this single center survey study, we identified a disproportionate burden of pages across specialties. GS trainees reported receiving higher average pages during day shifts and night call, as well as mistake pages with subsequently greater time spent on redirecting pages. While GS respondents reported received the highest volume of pages, they also reported the lowest perceived urgency of pages, suggesting high rates of nonurgent messages. These findings are concerning for potential implications on surgical errors due to flow disruptions and physician wellbeing. 4 Rates of burnout are high among surgical trainees, 15 with approximately one-third of GS residents experiencing frequent fatigue and 18% experiencing disengagement.16,17 Prior studies have reported correlations between pager volume with reduced sleep time and fatigue.9,18 Burnout symptoms were outside of the scope of this study; however, we suspect that administrative stress due to a high burden of nonurgent and mistake pages may be a contributor, especially among GS trainees.
One novel finding of this study are differences in communication preferences unique to a hybrid mobile and physical pager system. Trainees in surgical specialties were more likely to report preferring physical pagers for urgent communications, while nonsurgical trainees preferred smartphone paging. This may be due to differences in practice settings, including surgery residents being in more physically distinct locations (eg, operating room) that makes computer access less reliable. Several barriers have been reported in the implementation of smartphone or text message-based paging. 19 Our findings suggest an opportunity for tailoring paging systems to the preferences and needs of physicians in different specialties. Adoption of a universal paging system may be difficult, and potentially unsafe, without understanding the drivers for these preferences.
Another important finding of this study includes the free responses from trainees which raised several important themes, including concerns about using personal devices for work, limited service and battery life, and difficulty in separating personal life from patient-related communications. Concerns regarding use of personal cell phones for hospital work was raised by approximately 8% of respondents (eg, “I feel very strongly that we should have the option to carry physical pagers. I would not want my pages coming to my cell phone b/c too many other things already come to my phone and pages would be more easily overlooked,” Medicine Resident). Individuals also raised concerns about cellular network usage and phone bills (“I don’t want a mobile app because the hospital doesn’t pay for my cell phone bill and I don’t want anyone swiping through my personal cell phone looking for a paging app.,” Unknown Resident), and battery life when using personal devices (“[mobile device pager] relies on my phone battery and reception. I can’t selectively silence all of my other phone notifications while on call which makes sleep and other work more disruptive. I’d prefer a separate physical pager to reduce these interruptions and avoid reliance on my phone for coverage and battery life,” SS Resident). These concerns are consistent with those highlighted by Byrd et al’s qualitative study on secure text messaging systems. 19
Hospitals looking to integrate or transition to smartphone-based communications should solicit user concerns and address barriers preemptively, such as offering work phones, providing financial support for increased data usage, creating charging stations, and ensuring privacy measures for personal device content. Additionally, we recommend the implementation of paging systems that allow trainees to select communication modes that are most conducive to their line of work.
Limitations
There are several limitations to this study. Our cohort was relatively small with a 30.8% response rate, and nearly 22% of respondents did not provide their medical specialty. Due to the sample size and limited responses, we combined specialties to prevent potential identification of participants. However, there may be differences within specialties which were obscured by our groupings. Similarly, PGY level was not obtained to prevent identification of participants given many surgical specialties only have 1 resident per class. Given the differences in content and urgency of pages received by junior vs senior residents, data collection and categorization based on seniority may have yielded more nuanced findings. Additionally, given the limited responses from GS trainees, it is possible that pager burden on GS trainees is underestimated as we suspect residents who receive the highest number of pages may have not completed the survey. This study was also subject to recall bias and selection bias. We aimed to mitigate selection bias by contacting all trainees through a shared listserv. For recall bias, we allowed participants to save and return to the survey. Since this survey was administered to current residents and fellows, the time between the experience and recall should be minimal. However, we were unable to corroborate our subjective findings with objective data obtained through the hospital pager data.
Our primary goal was to assess the subjective experiences of trainees using pagers; however, contextualizing these findings with objective pager data would be a meaningful next step. It is unclear how the true number of pages correlate with the perceptions and experiences of trainees from this present study alone. The study was conducted at a single center and while the hospital’s paging system supplies more than 2200 hospitals in the United States, 20 our findings are limited to the paging system that was studied. Additionally, free responses varied in response rate, length, and quality. To solicit subjective pager experiences more thoroughly, future directions include conducting in-depth qualitative interviews with trainees.
Finally, the specific culture of the institution and the study design being limited to a single center limits the generalizability of these findings. For example, the culture of sensitivity within the institution and within any given service may introduce biases that affect how trainees perceive pager burden. The culture of nursing staff at the institution also likely creates a unique threshold to page trainees based on personal relationships, resident availability, and accessibility of additional staff members. Thus, the findings are limited in its generalizability and would benefit from including other hospital systems with different nursing staff coverage and paging culture. Future studies may also benefit from inclusion of other healthcare professionals (eg, nursing staff) who play an important role in pager communication.
Conclusion
Subjective experiences of pager burden were disproportionately high among GS residents, who not only reported a higher number of pages and sleep or off-work interruptions, but also more frequent mistake and nonurgent pages. This increased pager burden may have implications on resident wellbeing and negatively impacting patient care. Further, preferences for urgent communication methods differed across specialties. Health systems should consider incorporating trainee preferences into paging systems. However, additional studies are warranted to increase the sample size, assess generalizability of the findings, and contextualize trainee experiences with objective hospital-level paging data.
Supplemental Material
Supplemental Material - Perceived Pager Burden Among Trainees Across Medical Specialties
Supplemental Material for Perceived Pager Burden Among Trainees Across Medical Specialties by Yoshiko Iwai, Elizabeth C. Ciociola, Taylor M. Carter, and Luigi Pascarella in Journal of The American Surgeon™.
Footnotes
Acknowledgments
The authors thank the survey experts who were consulted at the Odum Institute for Research in Social Science.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Meeting Presentation
Portions of this manuscript were presented at the 18th Annual Academic Surgical Congress, February 7-9, 2023, in Houston, TX.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.