
Abstract
Background
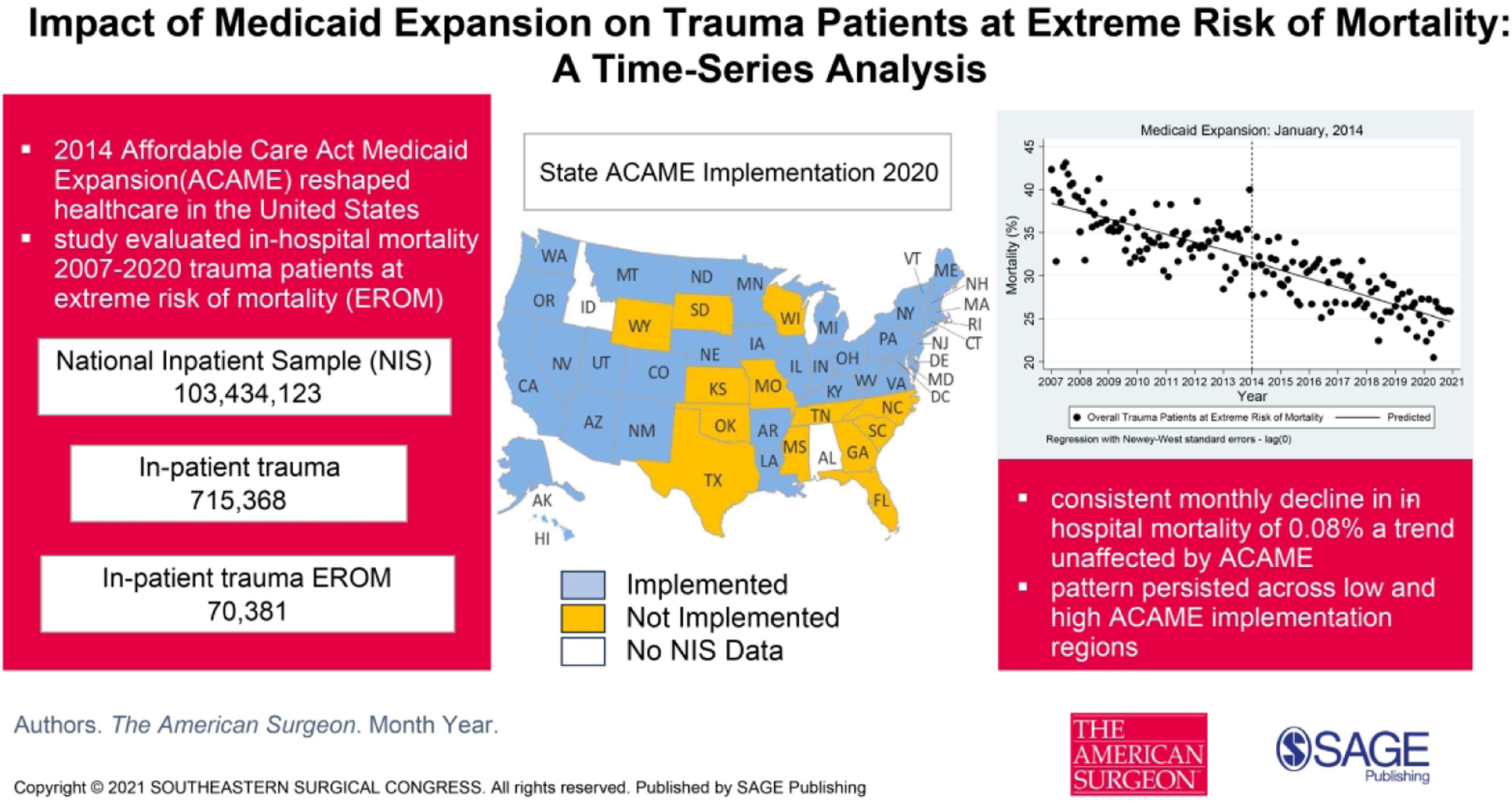
The 2014 expansion of Medicaid under the Affordable Care Act (ACA) reshaped healthcare delivery in the United States. This study assessed how Medicaid expansion affected in-hospital mortality in patients with extreme risk of mortality (EROM) from traumatic injuries.
Methods
Data from inpatients aged 18-64 years, registered in the National Inpatient Sample between 2007 and 2020, and identified with trauma-related All-Patient Refined Diagnosis Related Groups (APRDRG) codes, were analyzed. Within this group, a subset of patients was selected based on the APRDRG classification identifying them as at EROM for the principal unit of analysis. The cohort was divided into high-implementation (HIR) and low-implementation (LIR) regions based on Medicaid expansion coverage. In-hospital mortality was assessed using interrupted time-series analysis. Sensitivity analyses considered seasonality, autocorrelation, and exogenous events.
Results
Analysis encompassed 70 381 trauma inpatient stays, corresponding to 346 659 patients based on National Inpatient Sample weighting. There was a consistent monthly decline in in-hospital mortality of .08% (95% CI: −.103 to −.048; P < .001) prior to Medicaid expansion, a trend unaffected by expansion. This pattern persisted across both LIR and HIR Medicaid implementation regions. Although Medicaid enrollment increased in HIR, that in LIR remained unchanged.
Discussion
Over the study period, the in-hospital mortality among severely injured patients consistently decreased, and this trend was not influenced by Medicaid expansion. The statistical models and results from this study can offer valuable guidance to policymakers and healthcare leaders as they formulate more efficient and effective policies.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.