
Abstract
Background
Thyroid nodule fine needle aspiration (FNA) biopsies are associated with a low false-negative rate. There is limited data regarding the predictive value of American College of Radiology Thyroid Imaging Reporting and Data System for false-negative FNA.
Methods
This single-center retrospective study evaluated 119 patients who underwent thyroidectomy. The association of TR category, along with other clinical variables, with false-negative FNA was evaluated.
Results
The overall false-negative rate of FNA was 10.8% (n = 9). False-negative FNAs were associated with younger age (mean 42 years vs 50.6 years, P = .04), larger nodule size (mean 4.4 cm vs 3.2 cm, P = .03), and a lower TR category (median 3 v 4, P = .01).
Discussion
Lower TR category, younger age, and larger nodule size were associated with false-negative FNA of thyroid nodules. These findings should be taken into context when counseling patients with thyroid nodules who have a benign FNA.
Key Takeaways
• Lower ACR TI-RADS category is associated with false-negative FNA of thyroid nodules. • Younger age and larger nodule size are also associated with false-negative FNA. • Consider continued surveillance or repeat FNA in at-risk thyroid nodules.
Introduction
Ultrasound plays an integral role in the initial evaluation of thyroid nodules. Multiple societies including the American Thyroid Association, Korean Society of Thyroid Radiology, and European Thyroid Association have created classification systems to stratify the risk of malignancy for thyroid nodules based on ultrasound characteristics in attempts to decrease the number of unnecessary biopsies. The American College of Radiology (ACR) developed the ACR Thyroid Imaging, Reporting and Data System (TI-RADS) to determine which nodules are clinically relevant and warrant biopsy evaluation. 1
Once a nodule is deemed high enough risk to warrant biopsy, fine needle aspiration (FNA) is the preferred diagnostic maneuver. Fine needle aspirations are used to differentiate benign from malignant lesions, which in turn determines the need for surgical intervention. Though FNA false-negative rates are generally low, some studies have reported a false-negative rate as high as 21%; a literature review of 12 studies involving over 4000 patients with statistical modeling estimated that the sensitivity of FNA could be as low as 66%.2,3 There are conflicting results regarding which factors impact false-negative rate including nodule size, multi-nodularity, microcarcinomas, and expert cytopathologist involvement.4–6 Current American Thyroid Association (ATA) guidelines for surveillance of nodules that have had a benign FNA are based on sonographic appearance of the nodule but without correlation to TI-RADS scoring or size. 7 Indeed, few studies have investigated the relationship between ultrasound risk stratification systems and false-negative FNAs of thyroid nodules.6,8 Thus, the objective of this study was to evaluate the relationship between false-negative FNA and ACR TI-RADS category (TR category).
Material and Methods
Following exemption from the Institutional Review Board at Harbor-UCLA Medical Center, all adult patients who underwent thyroidectomy between January 2017 and June 2022 at a single urban safety-net hospital were identified by chart review. Patients who were missing preoperative US or FNA or who had a prior history of thyroidectomy were excluded. Retrospective chart review was used to collect data on patient demographics, clinical symptoms, ACR TI-RADS category (TR), nodule size, Bethesda score, FNA cytology, and surgical pathology.
The primary outcome was false-negative FNA. False negative was defined as a nodule with an FNA Bethesda score of 2 and a malignant surgical pathology. Microcarcinomas, defined as malignancy <1 cm on surgical pathology, were not considered as false negatives. In patients with multiple nodules, each nodule that underwent FNA was independently assessed for evaluation and matched to final pathology based on pathologic description of location. In patients with multiple nodules, each nodule that underwent FNA was independently assessed for evaluation and matched to final pathology based on pathologic description of location. Fine needle aspiration cytopathology was categorized according to the Bethesda System for Reporting Thyroid Cytopathology. 9 Ultrasound findings were reported according to ACR TI-RADS category. 1 Given ACR TI-RADS was not widely adopted at our institution until 2018, patients who did not have a charted TR category were retrospectively reviewed by our radiologists, who were blinded to the pathologic results of the nodules.
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. Data were collected into a Microsoft Excel database (Microsoft Corp) and imported to SAS format version 9.4 (SAS Institute) for statistical analyses. All variables were evaluated with descriptive statistics. Categorical variables were described as proportions and continuous variables were described as means or medians with 95%CI or interquartile ranges, as appropriate. For categorical variables (Bethesda score, TR category, and final pathologic subtype), chi-square analysis with odds ratios and their 95%CI were described. Fisher’s exact test was utilized to adjust for those cells with <5 units of analysis. For continuous variables, such as nodule size and age, median and mean values were compared between the positive and false-negative cohorts. The diagnostic test characteristics (sensitivity, specificity, etc) for FNA were also described. Statistical significance was determined at a P < .05 or if the 95%CI did not cross unity (effect estimates for OR would not cross 1, and continuous differences would not cross 0).
Results
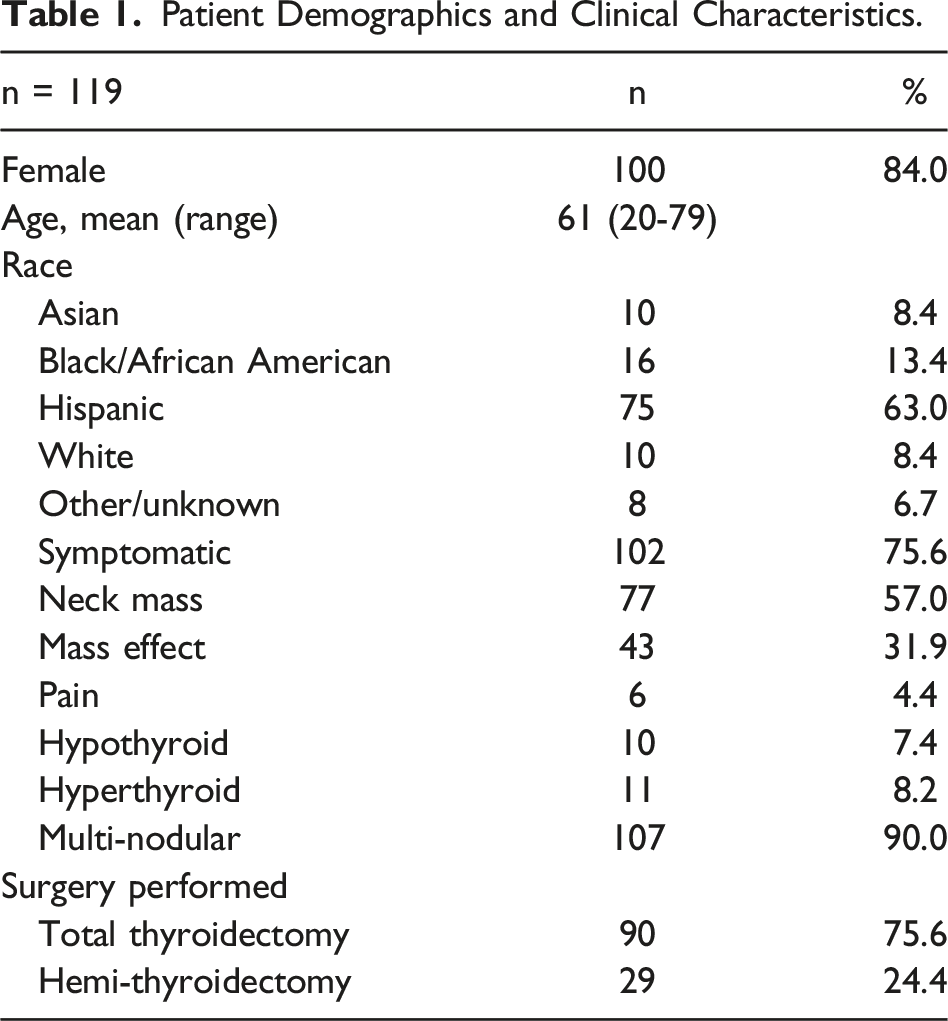
Patient Demographics and Clinical Characteristics.
Ultrasound and Pathology Results.
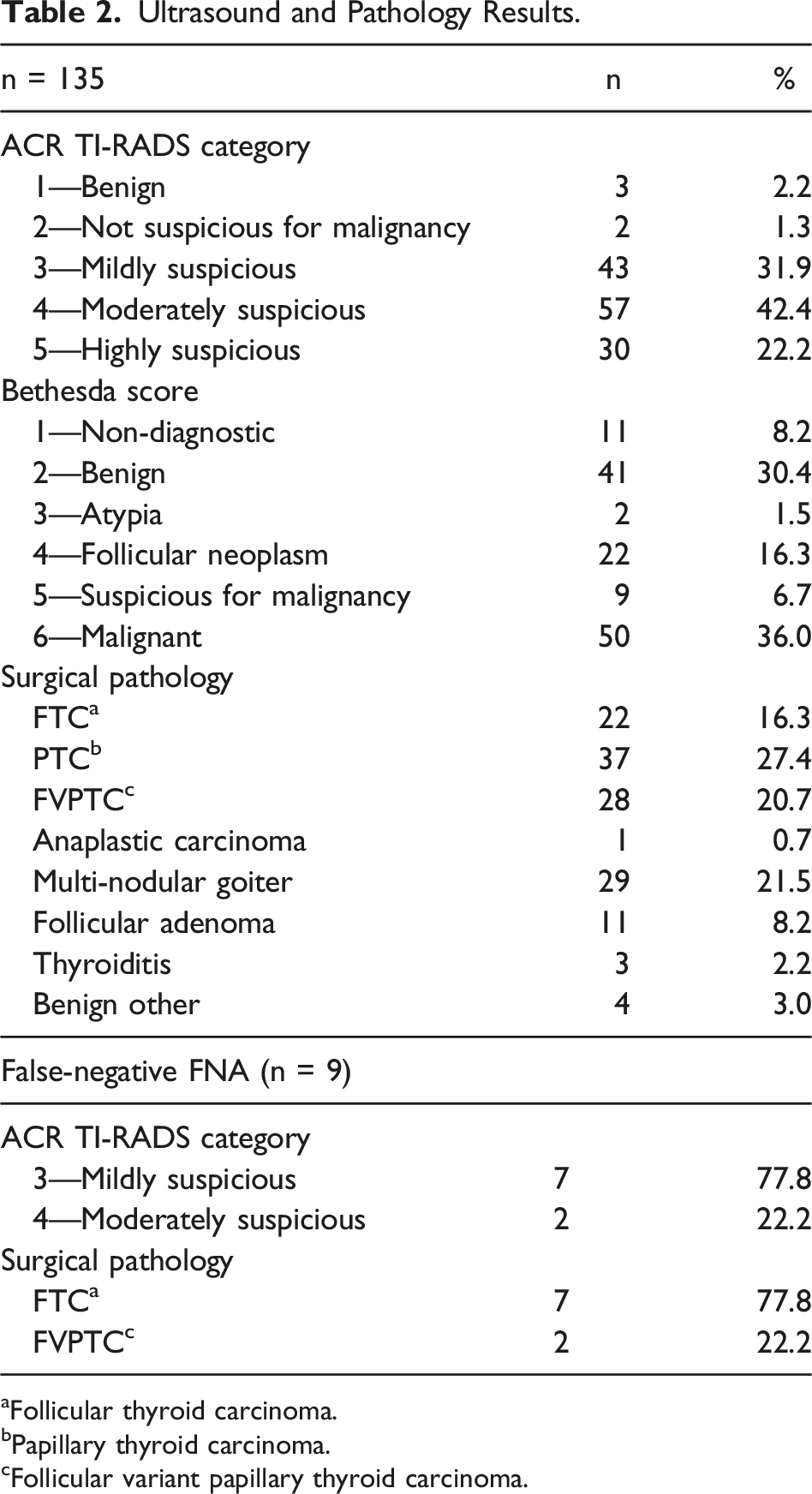
aFollicular thyroid carcinoma.
bPapillary thyroid carcinoma.
cFollicular variant papillary thyroid carcinoma.
The sensitivity of the FNA in this study was 89.2% with a specificity of 84.2%. The positive predictive value of the FNA was 89.2%, and the negative predictive value was 78%. Eleven non-diagnostic FNAs were excluded from this analysis, which resulted in 5 malignant and 6 benign surgical pathologies. The overall accuracy of the test was 85.5% with a false-negative rate of 10.8%. The negative predictive values (NPV) of each TIRAD category are as follows: TR 3 .68, TR 4 .86, and TR 5 1.0.
Association With False-Negative FNA.

aAmerican College of Radiology Thyroid Imaging, Reporting and Data System.
Discussion
Prior studies have evaluated Korean TIRAD (K-TIRAD) scores in association with false negatives and found that nodules >3 cm with a K-TIRAD 4 (intermediate suspicion of malignancy) lesion or greater were associated with a higher rate of false negatives.6,8 Similarly, in nodules >4 cm with suspicious US patterns, the false-negative rate was 42.5% and lobectomy was recommended in these patients. 7 Current ATA guidelines for surveillance of thyroid nodules with benign FNAs recommend repeat biopsy at 1 year only for nodules with high suspicion ultrasound pattern. 10 As such, it is of interest that our study found that false-negative FNAs were more likely to be associated with nodules with a mean score of TR 3, and TR 3 nodules have an NPV of .68 which was significantly lower than any other TIRAD category. TR 3 nodules are defined as having mildly suspicious ultrasound features, and ACR recommendations are for biopsy only for those nodules greater than 2.5 cm.
One factor that may explain the association with lower TR category is the prevalence FVPTC or FTC in the false-negative nodules. These malignancies tend to have less suspicious findings on US, with FVPTCs classified as “probably benign” in up to 25% of cases.
11
The US features of FVPTC are typically benign in nature and not strongly suggestive of malignancy. They generally appear to be hypoechoic solid nodules but lack calcifications, and this was demonstrated for false-negative nodules in our study that resulted in FVPTC (Figure 1). When evaluated by K-TIRADS, FTCs typically are low (K-TIRAD 3) to intermediate suspicion (K-TIRAD 4) for malignancy on US in 88.9% of cases.
12
In stark contrast, classic PTCs were highly suspicious for malignancy (K-TIRADS 5) in 78.9% of cases, compared to 11.1% of FTCs. Furthermore, FVPTC tends to be characterized by abundant colloid and lack papillary formations or psammoma bodies, and as such, FNAs are more likely to be interpreted as benign.
13
In our current study, 7 of the 9 false-negative FNAs were TR 3 indicating mild suspicion for malignancy, and none of the nodules were highly suspicious for malignancy. False-negative TR 3 nodule. Large nodule occupying nearly half of the thyroid gland. Determined TR 3 due to being a solid nodule (2 points) that is isoechoic to the gland (1 point) without any suspicious features. Fine needle aspiration of this nodule was benign while final pathology resulted in follicular variant papillary thyroid cancer.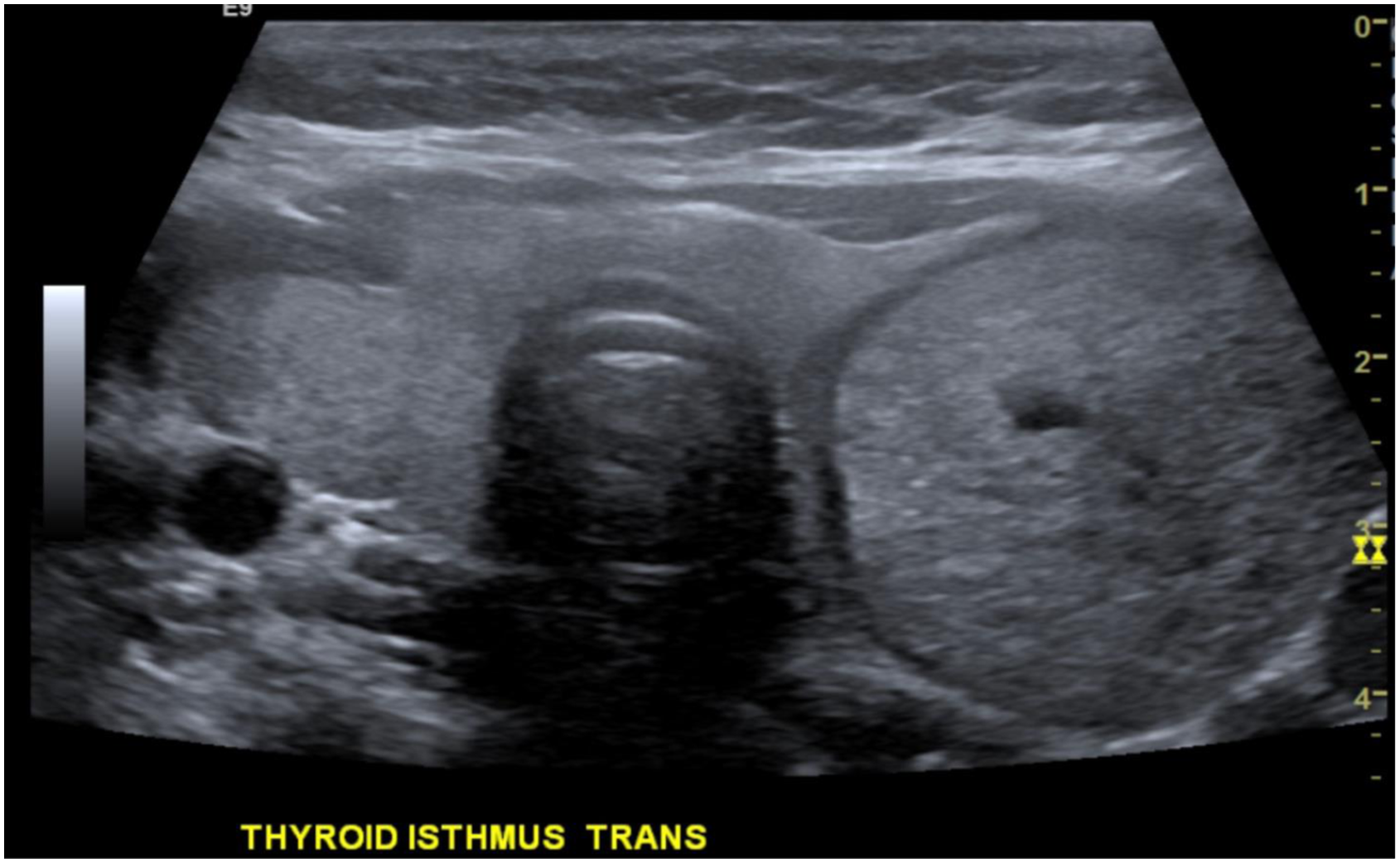
The current literature is also conflicting regarding the risk false-negative FNA and the subsequent management of larger thyroid nodules. Indeed, the ATA guidelines do not mention size when making recommendations for follow-up of benign FNAs. Several studies have found that nodules >4 cm are at a higher risk of false-negative FNA.5,14 Wharry et al found the incidence of malignancy in nodules >4 cm was 22% with a false-negative rate of 10.4%. Additionally, US was not helpful in determining malignant from benign nodules. 14 These studies recommend lobectomy for large thyroid nodules based on size alone. Conversely, several studies found in the setting of an adequate sample, proper cytologic preparation, and analysis by an expert cytopathologist, the false-negative rate of nodules >3-4 cm was less than 1%.4,15 These authors do not recommend using size alone as criteria for lobectomy.14,15 Our findings support that larger nodules are significantly associated with false-negative FNAs. This association may be influenced by the prevalence of FTC in the false-negative FNAs in this study. Prior studies have demonstrated that while thyroid cancer risk is not overall increased in nodules >2 cm, the risk of FTC in particular increases with nodule size. 16 Therefore, given the increased risk of FTC and the potential risk of increased false-negative FNA in larger nodules, clinicians should consider the role of continued surveillance or repeat FNA if initial cytology is benign in larger nodules.
Younger age was also found to be associated with a higher risk of false-negative FNA in our study. Although older patients tend to have higher-risk thyroid malignancies when found, Kwong et al found the incidence of malignancy in newly identified nodules steadily declines from age 20 to 60 years. In the youngest cohort of patients (age 20-29) the incidence of thyroid malignancy was 22.9%, compared to 12.6% in the oldest cohort (age >70). 17 In addition, age <55 years was found to be 3.7-fold more likely to have a false-negative FNA in nodules >4 cm. 18 This study supports that younger patients are at a higher risk of false-negative FNA. Given that incidence of malignancy in nodules is higher in younger patients and who are at a higher risk of false negatives, age should be considered when interpreting FNA results and counseling patients on benign findings.
The overall consequence of a false-negative biopsy and not undergoing subsequent surgery is considered to be low. One study followed over a thousand patients with initially benign FNAs for a total of 8.5 years. 19 During the study period, 18 false-negative malignancies were identified and resected at a mean of 4.5 years after the initial biopsy. In the entire cohort, there were no deaths attributed to thyroid cancer during the follow-up period. While these good results present a sense of comfort regarding false-negative biopsies, it remains hard to justify discounting the risk given the young age of the patients in our study with false-negative biopsies. It must also be pointed out that most of our patients did undergo subsequent radioactive iodine ablation for their malignancies. Although their outcomes are likely to be good, the delay in diagnosis of cancer was not inconsequential.
There are several limitations to this study. First, this was a retrospective study using surgical pathology as the criterion standard to distinguish false negative from true negatives. This could confer selection bias for larger, symptomatic lesions, as in indication for surgical intervention. Studies have supported the use of two negative biopsies as an indicator as a true negative with a less than 1.3% false negative rate, and this criteria should be considered for future studies. 20 Additionally, there were few false negatives in the study, which limited the power to detect differences in our subgroup analysis. Larger studies are warranted to further investigate the relationship of false-negative FNA with ACR TI-RADS category.
Lower ACR TI-RADS score, younger age, and larger nodule size are associated with false-negative thyroid FNA. These factors should be taken into consideration when counseling patients with a benign FNA and determining the need for continued follow-up or repeat biopsy.
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.