
Abstract
Background
Acute uncomplicated diverticulitis (AUD) is a common cause of acute abdominal pain. Recent guidelines advise selective use of antibiotics in AUD patients. This meta-analysis aimed to compare the effectiveness of no antibiotics vs antibiotics in AUD patients.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses to identify randomized controlled trials (RCTs) involving AUD patients which compared the use of antibiotics with no antibiotics. Pooled outcome data was calculated using random effects modeling with 95% confidence intervals (CIs).
Results
5 RCTs with 1934 AUD patients were included. 979 patients were managed without antibiotics (50.6%). Patients in the no antibiotic and antibiotic groups had comparable demographics (age, sex, and body mass index) and presenting features (temperature, pain score, and C-reactive protein levels). There was no significant difference in rates of complicated diverticulitis (OR: .61, 95% CI: 0.27-1.36, P = .23), abscess (OR: .51, 95% CI: .08-3.25, P = .47) or fistula (OR: .33, 95% CI: .03-3.15, P = .33) formation, perforation (OR: .98, 95% CI: .32-3.07, P = .98), recurrence (OR: .96, 95% CI: .66-1.41, P = .85), need for surgery (OR: 1.36, 95% CI: .47-3.95, P = .37), mortality (OR: 1.27, 95% CI: .14-11.76, P = .82), or length of stay (MD: .215, 95% CI: −.43-.73, P = .61) between the 2 groups. However, the likelihood of readmission was higher in the antibiotics group (OR: 2.13, 95% CI: 1.43-3.18, P = .0002).
Conclusion
There is no significant difference in baseline characteristics, clinical presentation, and adverse health outcomes between AUD patients treated without antibiotics compared to with antibiotics.
Introduction
Diverticular disease is one of the commonest causes of acute lower abdominal pain, representing a significant burden to health care. 1 In patients aged over 60, 50% have diverticular disease and whilst the majority remain asymptomatic, up to 25% can present with an episode of acute diverticulitis.2,3 An episode of acute diverticulitis without any complications such as abscess formation, peritonitis, obstruction, or fistula formation has traditionally been treated with antibiotics. 4 However, recently the use of antibiotics in AUD has been disputed given its new definition of an inflammatory reaction rather than an intra-abdominal infection. 5 Antibiotic treatment has several limitations such as economic cost, potential risk of adverse drug reactions, superinfection due to susceptibility to opportunistic infection, and resistance due to overprescribing. 4
Multiple observational studies and randomized controlled trials (RCTs) have investigated comparative outcomes of AUD treated with and without antibiotics. This has led to a change in guidelines advocating avoidance of antibiotic therapy in selected cases of AUD. 6 A recent Cochrane review of 3 RCTs, which evaluated the comparative outcomes of management of AUD with or without antibiotics, concluded that the available evidence regarding use of antibiotics for AUD seems to be uncertain for the rationale of using antibiotics to reduce complications, emergency surgery, recurrence, elective colonic resections, and long-term complications. Therefore, the authors recommended the need for more RCTs in this context. 4
Considering the existence of more RCTs, we aimed to conduct a meta-analysis of randomized evidence with respect to patient’s baseline characteristics and reported outcomes, to evaluate the impact of use of antibiotics vs no antibiotics on the outcomes of patients with AUD.
Methods
This systematic review and meta-analysis were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement and registered on PROSPERO (registration number CRD42023438632). 7 Given the fact that this study was a meta-analysis of published data, no ethical approval was required to conduct the study.
Inclusion and Exclusion Criteria
Randomized controlled trials (RCTs) only were considered eligible. Case reports, review articles, editorials, research letters, case series, case-control studies, observational studies, systematic reviews, and meta-analyses were excluded. The population of interest were adults (>18) with a diagnosis of left-sided AUD. The comparison was the use of an antibiotic versus no antibiotic or placebo in patients with AUD. The primary outcomes of interest were mortality and adverse outcomes (perforation, abscess, need for emergency surgery, and fistula). Secondary outcomes were readmissions, length of stay (LOS), and recurrence.
Screening and Data Extraction
Two authors independently screened the titles and abstracts of the identified studies. Any disputes were resolved with discussion, with any further disputes resolved by a third reviewer. Data were extracted by 2 independent authors using pre-formed tables. Study characteristics such as first author, publication year, study design, and journal were extracted. Study results were extracted and stratified according to group (no antibiotics vs antibiotics). The extracted results included demographic information of patients (age, sex, body mass index, and comorbidity score), presentation on admission (white blood cell count, c-reactive protein, and temperature) and outcomes (mortality, complications, readmission, and LOS). Any disagreements were resolved by a third reviewer.
Risk of Bias Assessment
Two authors independently assessed the methodological quality of each included study using Cochrane’s tool for RCTs. 8 The tool considers risk of performance, reporting, detection, attrition, and any other sources of bias in each of the included studies. Any disputes between authors were resolved by discussion, with any further disputes resolved by a third reviewer.
Data Analysis
Data analysis was performed using Review Manager 5.4. 9 One author extracted and entered data into Review Manager 5.4 and another author cross-checked the data. For dichotomous outcomes, odds ratios (ORs) were calculated. For continuous outcomes, mean difference (MD) between groups was calculated. Where median and interquartile range were reported instead of the mean, extracted data were converted to mean and standard deviation using Hozo et al’s equation. 10 All analyses were performed with random-effects modeling. Outcomes were reported with Forest plots with 95% confidence intervals (CIs). The unit of analysis was the individual patient.
Cochran Q test was used to assess the heterogeneity between studies. I2 was calculated to assess the degree of heterogeneity. 0% to 50% was interpreted as insignificant heterogeneity, 50% to 75% was interpreted as moderate heterogeneity, and 75% to 100% was interpreted as large heterogeneity. Trial sequential analysis was performed to investigate the likelihood of type 1 and type 2 errors using random-effects modeling and a 95% CI using TSA software. 11 To determine the likelihood of type 1 and type 2 errors, O’Brien-Fleming α-spending function and futility boundaries were used.
Sensitivity Analyses
Sensitivity analyses were conducted to explore potential sources of heterogeneity and assess the robustness of the results. Finally, the effect of each study was evaluated on the overall effect size and heterogeneity by repeating the analysis following excluding 1 study at a time (leave-one-out sensitivity analysis).
Results
A total of 153 articles were retrieved and 120 were screened after removal of duplicates (Figure 1). A total of 5 RCTs met the inclusion criteria.12-16 A total number of 1934 patients with AUD were included, 979 were managed without antibiotics while the remaining 954 received antibiotics. PRISMA flow chart.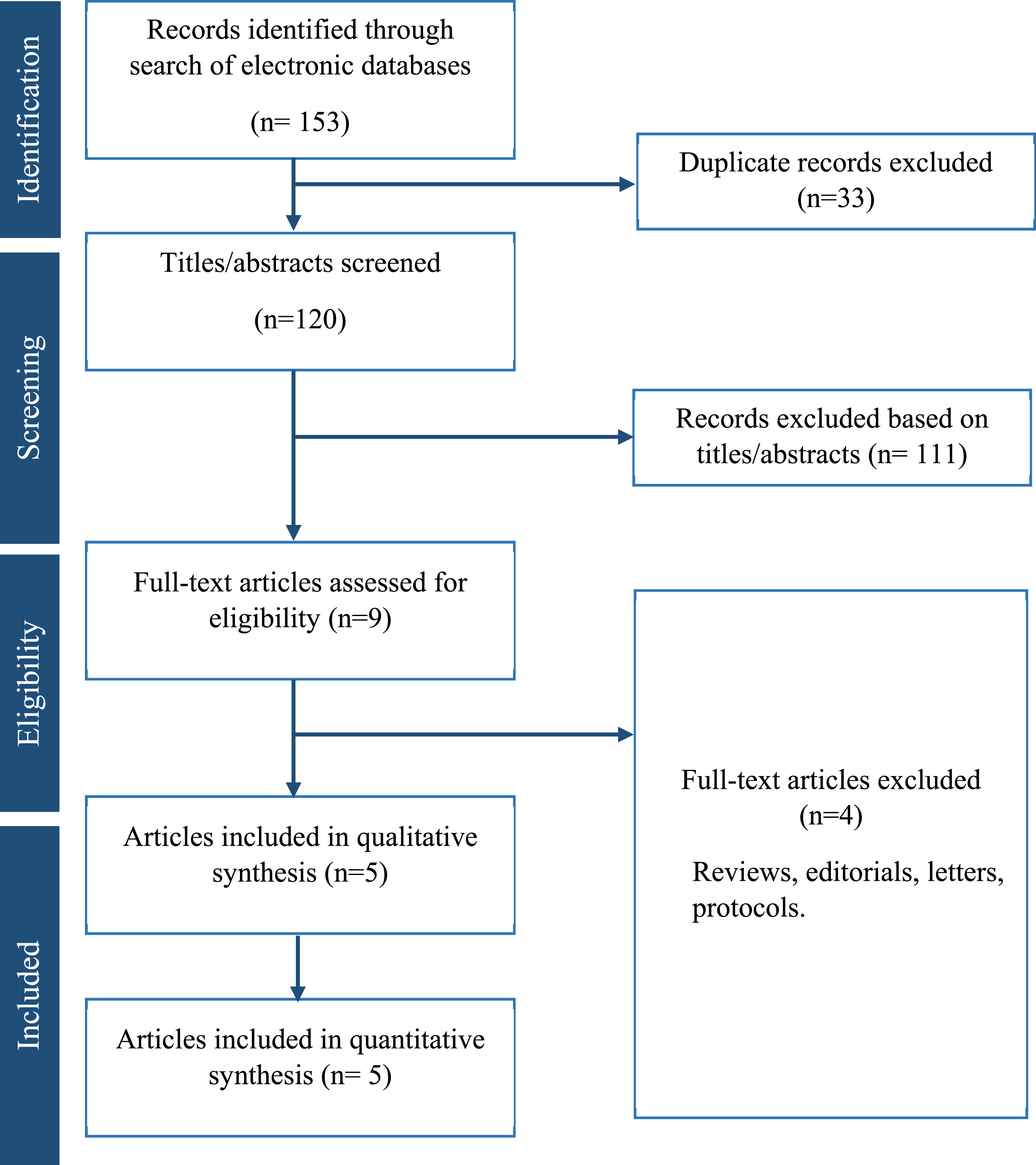
Study Related Data.
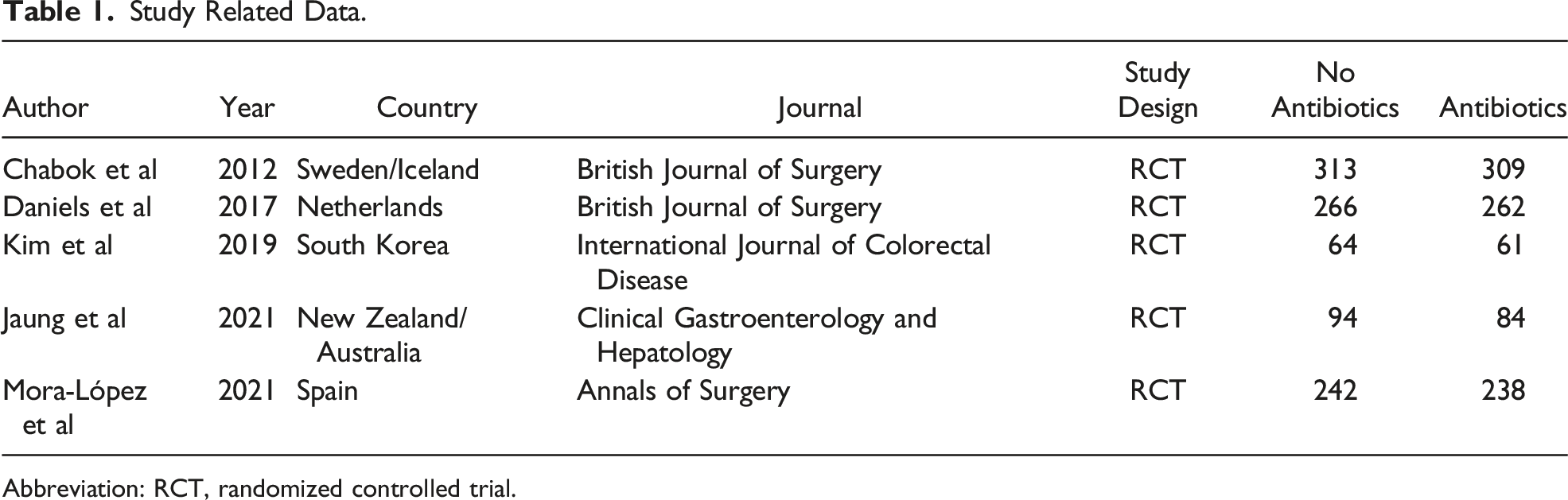
Abbreviation: RCT, randomized controlled trial.
Baseline Characteristics of Included Populations.
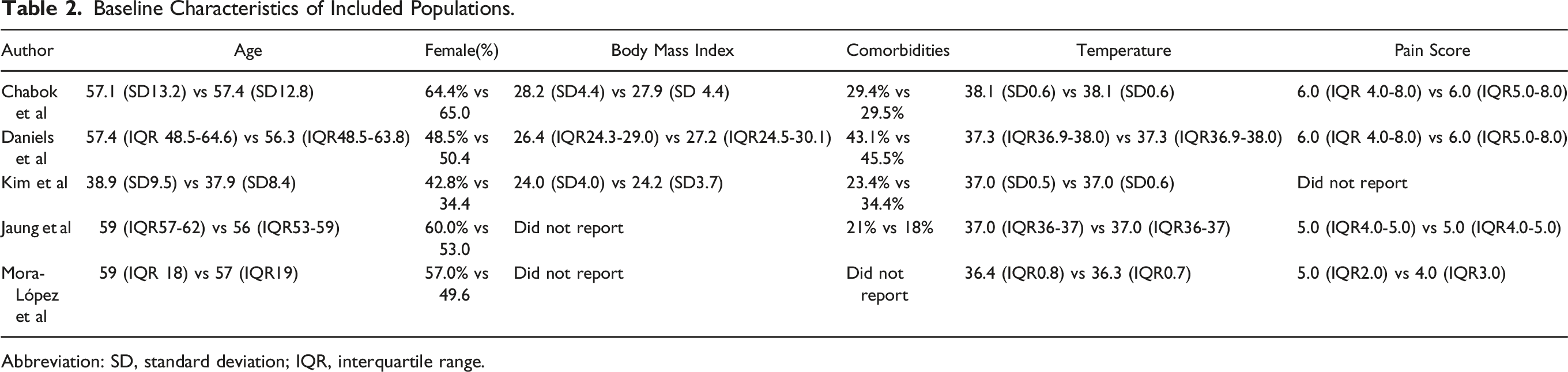
Abbreviation: SD, standard deviation; IQR, interquartile range.
Patients in both the no antibiotic group and antibiotic group were of a similar age (52.91 ± 7.51 vs 54.14 ± 7.69, P = .19), sex (56.0% female vs 54.5% female, P = .49), and BMI (26.45 ± 1.61 vs 26.24 ± 1.72, P = .50). There was no significant difference between temperature at presentation (MD −.01 95% CI −.04-.02, P = .54), pain score (MD −.07 95% CI −.37-.22, P = .63), WBC count (MD −.08 95% CI −.48-.33, P = .72), and CRP levels (MD 1.33 95% CI −3.10-5.76, P = .56). However, a history of previous diverticulitis was significantly higher in patients in the no antibiotic group than those in the antibiotic group (41.8% vs 34.6%, P = .03).
Risk of Bias Assessment
Figure 2 presents the risk of bias assessment of the included RCTs. 3 studies had a low risk of selection bias, and 2 studies had unclear risk of selection bias due to lack of provided data on allocation concealment. 4 studies had a high risk of performance and detection bias due to lack of blinding of patients and assessors. All included studies had a low risk of attrition, reporting bias, and other types of bias. Risk of bias summary and graph showing authors’ judgments about each risk of bias item.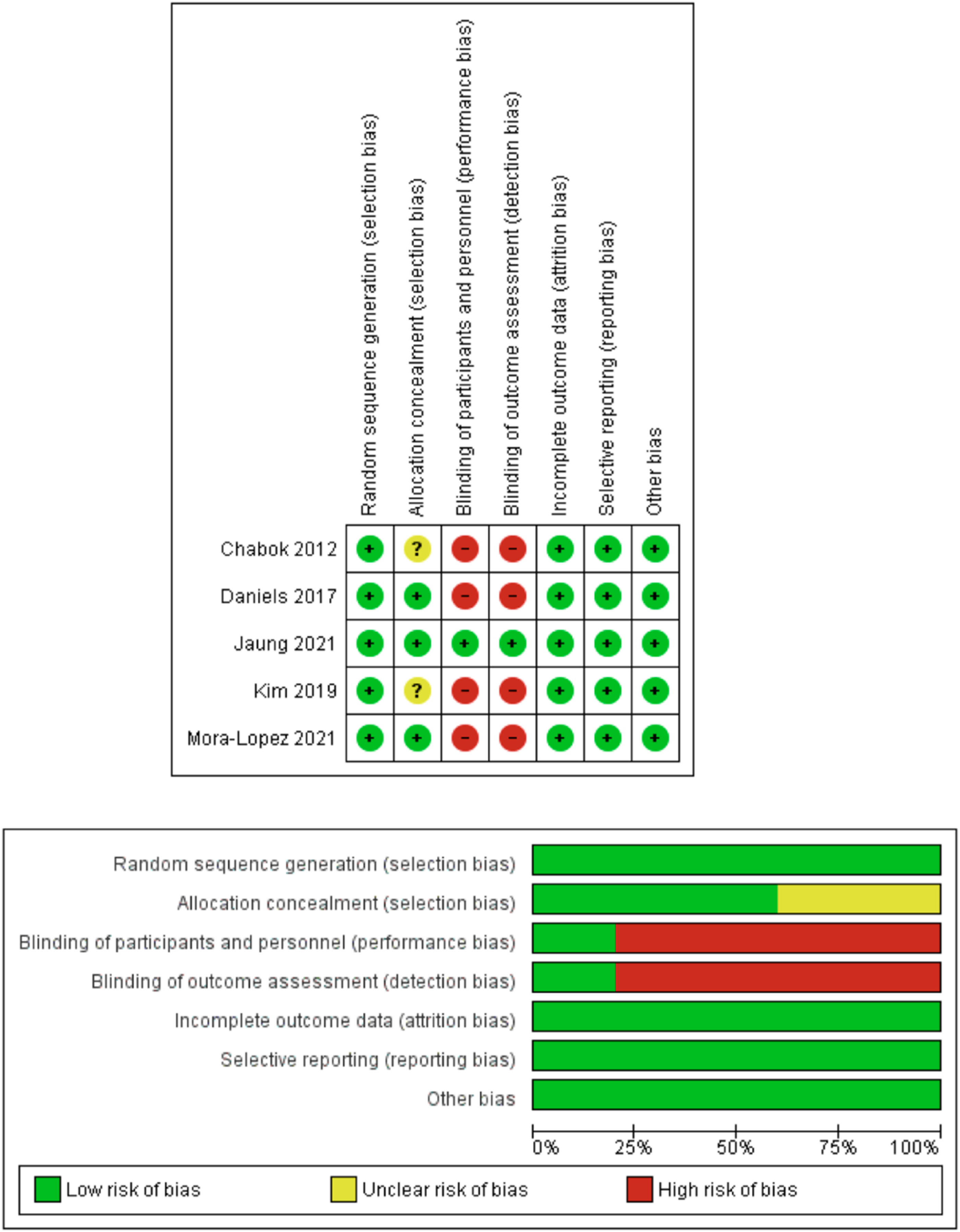
Outcome Synthesis
Outcomes are summarized in Figure 3. Forest plots of comparison of (A) complicated diverticulitis, (B) diverticular perforation, (C) abscess, (D) fistula, (E) need for surgery, (F) recurrence, (G) mortality, (H) length of stay, and (I) overall readmission rates. The solid squares denote the odds ratios (ORs) or risk difference (RD). The horizontal lines represent the 95% confidence intervals (CIs), and the diamond denotes the pooled effect size. M-H, Mantel Haenszel test.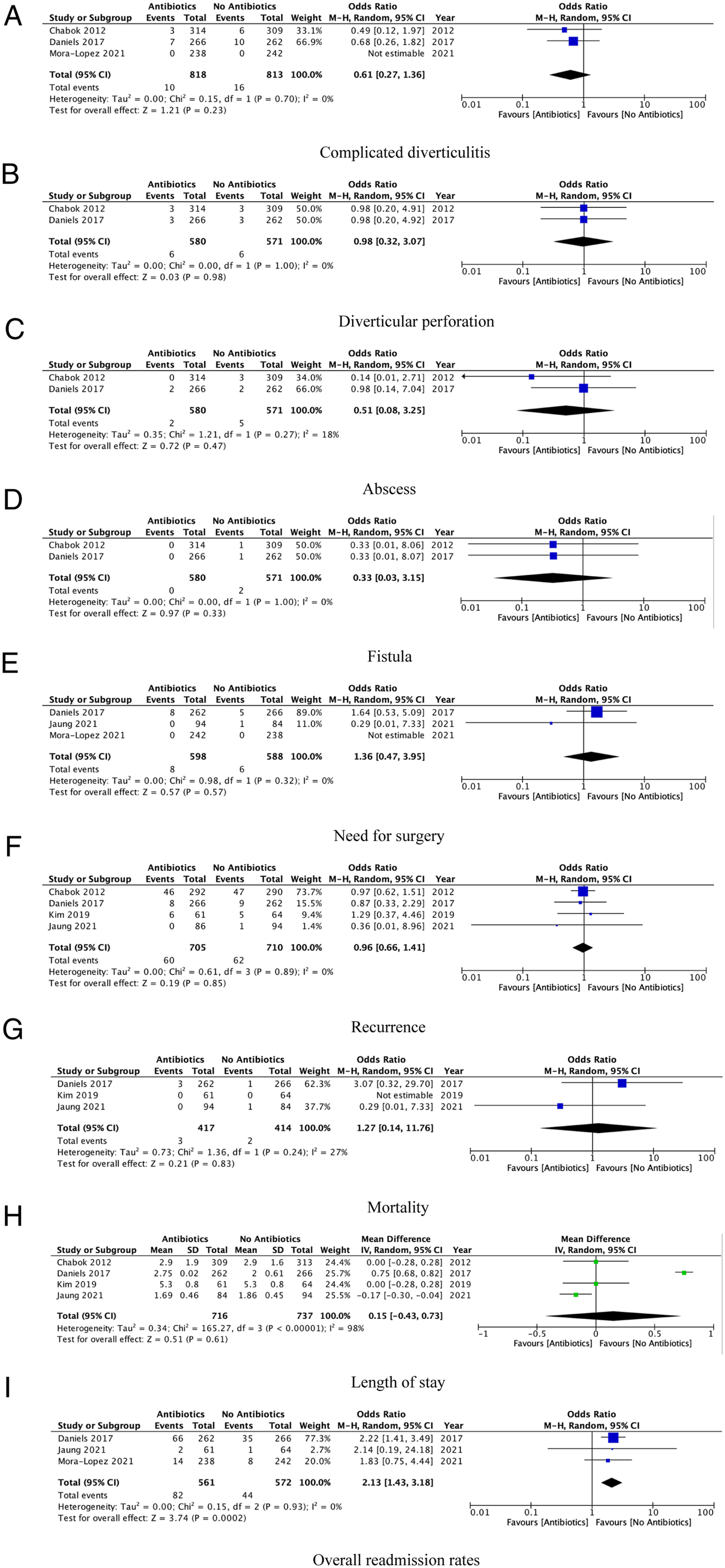
Complicated Diverticulitis
Three studies reported complicated diverticulitis as an outcome.12,13,16 The rate of complicated diverticulitis was 1.97% in the no antibiotic group and 1.22% in the antibiotic group. There was no significant difference in rate of complicated diverticulitis between the 2 groups (OR: .61, 95% CI: 0.27-1.36, P = .23). There was low between-study heterogeneity (I2 = 0%, P = .70).
Diverticular Perforation
Two studies reported diverticular perforation as an outcome.12,13 The rate of perforation was 1.05% in the no antibiotic group and 1.03% in the antibiotic group. Both groups had a comparable risk of diverticular perforation (OR: .98, 95% CI: .32-3.07, P = .98). There was low between-study heterogeneity (I2 = 0%, P = 1.00).
Abscess
Two studies reported abscess formation as an outcome.12,13 The rate of abscess formation was .88% in the no antibiotic group and .34% in the antibiotic group. There was no significant difference in rate of abscess between the no antibiotic and antibiotic groups (OR: .51, 95% CI: .08-3.25, P = .47). There was low between-study heterogeneity (I2 = 18%, P = .27).
Fistula
Two studies reported fistula formation as an outcome.12,13 The rate of fistula formation was .35% in the no antibiotic group while no patients in the antibiotic group developed a fistula. There was no significant difference between the no antibiotic and antibiotic groups (OR: .33, 95% CI: .03-3.15, P = .33). There was low between-study heterogeneity (I2 = 18%, P = 1.00).
Need for Surgery
3 studies reported the need for a surgical intervention as an outcome.13,15,16 A surgical intervention was required in .99% of patients who did not receive antibiotic therapy while 1.02% of the patients in the antibiotic group needed a surgical intervention. There was no significant difference between both groups (OR: 1.36, 95% CI: .47-3.95, P = .37). There was low between-study heterogeneity (I2 = 0%, P = .32).
Recurrence
Four studies reported recurrence of acute diverticulitis as an outcome.12-15 The rate of recurrence was 8.73% in the no antibiotic group and 8.51% in the antibiotic group. Both the no antibiotic group and antibiotic group were comparable (OR: .96, 95% CI: .66-1.41, P = .85). There was low between-study heterogeneity (I2 = 0%, P = .89).
Mortality
3 studies reported mortality as an outcome.13-15 The rate of mortality was .48% in the no antibiotic group and .72% in the antibiotic group. Both groups had a similar rate of perioperative mortality (OR: 1.27, 95% CI: .14-11.76, P = .82). There was moderate between-study heterogeneity (I2 = 27%, P = .24).
Length of Stay
4 studies reported length of stay of their included patients.12–15 The mean length of stay in days was 2.65 in the no antibiotic group and 2.91 days in the antibiotic group. There was no significant difference between each group (MD: .215, 95% CI: −.43-.73, P = .61). There was high between-study heterogeneity (I2 = 98%, P < .001).
Overall Readmission Rates
3 studies reported readmission to hospital as an outcome.13,15,16 The rate of readmission to hospital was 7.69% in the no antibiotic group and 14.62% in the antibiotic group. The use of antibiotics was associated with significantly higher rate of readmission to hospital than no use of antibiotics (OR: 2.13, 95% CI: 1.43-3.18, P = .0002). There was low between-study heterogeneity (I2 = 0%, P = .93).
Sensitivity Analysis
The direction of pooled effect size remained unchanged when the risk ratio (RR) or risk difference (RD) was calculated. During leave-one-out sensitivity analysis, removal of study of Daniels et al 13 in the analysis of length of stay made the results in favor of the antibiotic group (MD: −.12, 95% CI: −.23-.01, P = .04).
Discussion
This systematic review and meta-analysis of randomized studies comparing antibiotics vs non-antibiotic therapy in management of AUD has important findings. Firstly, there were no significant differences in the baseline characteristics and presentation on admission for the 2 groups. Secondly, there were no significant differences in complication rates between the 2 groups. Overall, our findings suggest that antibiotics may not be needed for the treatment of AUD in the absence of complications or clinical features of sepsis or peritonitis. The presence of low between-study heterogeneity in the analyses of all outcomes, except length of stay, indicates that our findings about these outcomes should be considered robust. This study, therefore, presents the need for a paradigm shift in the treatment of AUD away from the routine utilization of antibiotics.
Antibiotics were the guideline-indicated treatment for AUD for a number of years. Recently however, the routine use of antibiotics for AUD has been debated, which has led to updates in guidelines.5,17 Guidelines now state that antibiotics should be given to AUD patients on a case-by-case basis or if the patient is at a risk of complications, advising against routine use.6,17
A meta-analysis of individual patient data from 2 trials with patients with AUD demonstrated that several risk factors are associated with a complicated course of AUD, yet a lack of antibiotic prescription was not associated with an increased risk of complications. 18 Furthermore, this study demonstrated that there was not a significant difference in long-term outcomes at 6 and 12 months between groups, despite previous studies speculating a potential benefit of antibiotics on longer-term outcomes, which is in agreement with the present study. 18 Another meta-analysis investigating different treatment strategies for AUD demonstrated that conservative treatment was not significantly inferior to antibiotic therapy as well at rates of recurrence of diverticulitis and rates of emergency surgery. 19 The primary outcome of this study was failure of treatment requiring surgery and secondary outcome was recurrence in the form of readmission 19 for the non-antibiotic group vs the antibiotic group. 1.4% in the no antibiotic group vs .7% in the antibiotic group required emergency surgery and 12% in the no antibiotic vs 11% in the antibiotic group were readmitted with AUD (P = .3). 19
The findings from the study were corroborated by a meta-analysis of similar studies by Desai et al, where there was also no difference in complicated diverticulitis, colonic resection, and recurrence. 20 It has been speculated that antibiotic prescription could decrease colonic inflammation, preventing obstruction, recurrence, or persistent diverticulitis. 21 The present meta-analysis demonstrated that antibiotics conserved no additional benefit in these patients. In fact, patients receiving antibiotics had higher crude and adjusted odds of readmission, with no other significant differences in other outcome measures. Furthermore, to the best of our knowledge, this meta-analysis is the first meta-analysis which demonstrated comparability of baseline characteristics of the study populations in antibiotic and no antibiotic groups which further enhances the robustness of the conclusions made.
There are limited data about the risk factors for the occurrence of complications in AUD, meaning guidelines are vague as to what patient groups constitute antibiotic prescription. Multiple studies have identified several risk factors for complications such as CRP over 170 mg/dL on admission or multimorbidity.18,22 However, the likelihood of complications did not appear to be mediated by antibiotic prescription in the index admission. 18 The present study of RCTs did not find any statistically significant difference in the rates of complications (abscess formation, fistula, perforation, and complicated diverticulitis) between the 2 groups.
This study has important clinical implications. Selective use of antibiotics for cases of clinical need is imperative to improve the current antibiotic resistance crisis. 23 Overuse of antibiotics and inappropriate prescribing are major contributors. 23 Antibiotic treatment incurs a significant economic cost, risk of adverse reactions, and superinfection due to overprescribing. 4 A systematic review and meta-analysis of 21 studies for outpatient management of AUD found that ambulatory treatment was associated with daily savings of between €600 and €1900 with a 4.3% failure rate. 24 Therefore, contemporary guidelines in countries such as Italy, Germany, and America have advised careful consideration of antibiotics in AUD patients given their minimal benefit, as proven in the present study. This study demonstrates that in cases of AUD only, outcomes of patients treated without antibiotics do not differ from the outcomes of patients treated with antibiotics.
There are several areas for future research. Firstly, given the number of RCTs and the total number of included patients were low, there is less statistical power to this meta-analysis and a higher risk of type 2 error. More RCTs could be conducted with larger sample sizes to minimize the uncertainty of findings. Furthermore, these trials should be more robust in design to minimize the risk of bias through blinding. Secondly, there is a paucity of data relating to the location of AUD. Only 1 study has investigated right-sided diverticulitis, with the majority of studies investigating left-sided diverticulitis. Future studies could consider stratifying patients by the location of diverticulitis. Thirdly, 1 included RCT focused on radiological evidence of AUD only, whereas some others did not provide clear criteria for identification. Future studies could describe clear definitions for the diagnosis and categorization of AUD, improving reproducibility and repeatability of findings in subsequent studies, reducing heterogeneity. Finally, there was a lack of data on long-term outcomes. Future studies could investigate the longer-term prognosis of patients, especially in regards to readmission rates.
There are limitations associated with this study which should be considered when interpreting its findings. The number of eligible RCTs and the included patients were low, which may subject our findings to risk of type 2 error. There were 5 RCTs and not all studies reported all outcome measures. Furthermore, the risk of performance bias and detection bias were high in 4 studies due to lack of blinding of the patients and outcome assessors. Finally, there was varied reporting in baseline characteristics of patients between studies, with some reporting continuous data as median and IQR. Using a widely acceptable equation described by Hozo et al, we calculated mean and SD from the data which could have introduced bias in our results. 10
Conclusions
The meta-analysis of randomized evidence (level 1a) demonstrated that the outcomes of patients with AUD treated without antibiotics did not differ significantly compared to patients treated with antibiotics. Therefore, a conservative approach can be considered in patients with AUD not at risk of complications. Future high-quality RCTs with adequate power should deploy a more robust concealment process to provide stronger evidence in favor or against use of antibiotics in AUD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.