
Abstract
Background
Recent evidence suggests that routine intubation upon arrival for adults with isolated head trauma and a depressed Glasgow Coma Scale (GCS) score is associated with increased risk of morbidity and mortality. Whether these outcomes are similar within an adolescent trauma population has not been previously investigated. We hypothesized intubation upon arrival for adolescent trauma patients with isolated head trauma to be associated with a higher risk of death and prolonged length of stay (LOS).
Methods
The 2017-2019 TQIP was queried for adolescents (age 12-16) presenting after isolated blunt head trauma (abbreviated injury scale [AIS]
Results
From 141 patients, 73 (51.8%) were intubated upon arrival. Intubated patients had a low complication rate (5.6%). Intubated and non-intubated patients had a similar rate and mortality risk (6.8% vs 1.5%, P = .11) (OR 1.84, CI .08-43.69, P = .71) and median length of stay (LOS) (2 days vs 2 days, P = .13).
Discussion
Unlike adult patients, adolescents with isolated head trauma and a depressed GCS have similar outcomes if they are intubated upon arrival. Utilizing initial GCS score to determine which adolescent trauma patients with isolated head trauma should be intubated appears to be a safe practice.
Key Takeaways
• In contrast to in adults, immediate intubation upon arrival in adolescent trauma patients with isolated blunt head trauma was not associated with a higher risk of mortality. • Complication rate with routine intubation is lower in adolescent blunt head trauma patients than in adults. • GCS-based intubation guidelines may be reliable in adolescent blunt head trauma patients.
Introduction
Out of 150 million patients presenting to the hospital annually, less than 1% require endotracheal intubation. 1 Trauma patients tend to have more serious injuries requiring airway protection including those with traumatic brain injury (TBI). 2 One of the primary reasons to protect the airway in a TBI patient lies in decreasing the aspiration risk related to a depressed neurologic status.3,4 Aspiration events can occur in up to 40% of TBI patients and lead to significant complications including aspiration pneumonitis, pneumonia, and acute respiratory distress syndrome (ARDS). 4 Although endotracheal intubation can protect the airway, it can lead to complications including esophageal intubation, hypoxia, airway injury, and ventilator-associated pneumonia (VAP).5,6 In addition, complications directly related to endotracheal intubation can reach as high as 40% when occurring outside of the controlled conditions of the operating room (OR) such as the emergency department. 7
The American College of Surgeons Committee on Trauma (ASC-COT) and the Eastern Association for the Surgery of Trauma (EAST) both recommend protocolized endotracheal intubation for trauma patients with a Glasgow Coma Scale (GCS) score of ≤8.8,9 Although these guidelines have been widely accepted, there are few scientific studies supporting routine intubations for all patients with a GCS ≤8. More recent reports in adult trauma patients with blunt head trauma suggest that routine intubation may be harmful for some patients with GCS
The adolescent trauma population is of particular interest in determining the effectiveness of routine intubation as there are conflicting reports as to why intubation may be better tolerated by adolescent patients or associated with increased complications. For example, while adolescents have better cardiopulmonary reserve compared to adults, they also possess smaller airway anatomy, increasing the risk for and difficulty of intubation. 12
Therefore, this study aimed to evaluate the impact of routine intubation for adolescent patients with isolated blunt head trauma and GCS 6-8. We sought to describe the complications seen in adolescent trauma patients who are immediately intubated upon arrival with isolated head trauma and GCS 6-8, hypothesizing an increased risk of mortality, complications, and hospital length of stay (LOS) compared to patients not undergoing immediate intubation.
Methods
This retrospective cohort study was deemed exempt by our local Institutional Review Board and a waiver of consent was granted as the study utilizes a deidentified national database. The American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) database was queried (2017-2019) to identify adolescent patients (age 12-16) presenting after isolated blunt head trauma with a GCS 6-8 on arrival. Isolated head trauma was defined with an abbreviated injury scale (AIS) ≤1 for the spine, chest, abdomen, upper extremity, and lower extremity. Severe head trauma was defined as an AIS-grade ≥3 for the head. All patients with a penetrating mechanism of injury, transferred from another hospital, dead-on-arrival or who underwent an emergent operation from the emergency department were excluded. The latter population was excluded as these patients would require intubation for surgery. Patients intubated within 1 hour of presentation were compared to those not intubated within 1 hour.
The primary outcome was mortality. Demographic data collected include age, sex, mechanism of injury, and vitals upon arrival. Notable vitals upon arrival included hypotension (systolic blood pressure <90 mmHg), tachypnea (respiratory rate >22 breaths/min), and tachycardia (heart rate >120 bpm). Clinical outcomes measured included total hospital length of stay (LOS) for all patients and intensive care unit (ICU) LOS only for those admitted to the ICU. Other clinical outcomes measured included in-hospital complications including deep vein thrombosis, pulmonary embolism, myocardial infarction, cardiac arrest, ARDS, VAP, sepsis, acute kidney injury, catheter-associated urinary tract infection (UTI), intra-abdominal abscess, superficial surgical site infection (SSI), and deep SSI.
Frequency statistics were performed for all variables of interest. A chi-square test and Mann-Whitney-U test were used to compare categorical and continuous variables, respectively. Categorical data were reported as percentages, and continuous data were reported as medians with interquartile range or as means with standard deviation. To report an associated risk of mortality, we used a multivariable logistic regression model adjusting for age, sex, GCS, and AIS-grade for the head. These variables were selected after discussion among the coauthors and review of the literature selecting variables that may be associated with an increased risk of mortality. 3 We first performed a univariable logistic regression analysis and selected covariates with a P < .20 to enter our multivariable model. The adjusted risk for mortality was reported with an odds ratio (OR) and 95% confidence intervals (CI). All P-values were two-sided, with a statistical significance level of <.05. All analyses were performed with IBM SPSS Statistics for Windows (Version 28, IBM Corp., Armonk, NY).
Results
From 141 adolescent patients, 73 (51.8%) were intubated upon arrival. The median age for both cohorts was 15 years old. Both groups were predominantly male (75.0% vs 80.8%, P = .40). The non-intubated patient cohort had similar vital signs upon arrival to the hospital compared to the intubated cohort (all P > .05). Additionally, there were no differences in distribution of GCS scores between the 2 cohorts (P = .09).
Demographics, Comorbidities, and Injury Profile of Adolescent Blunt Head Trauma Patients on Arrival.
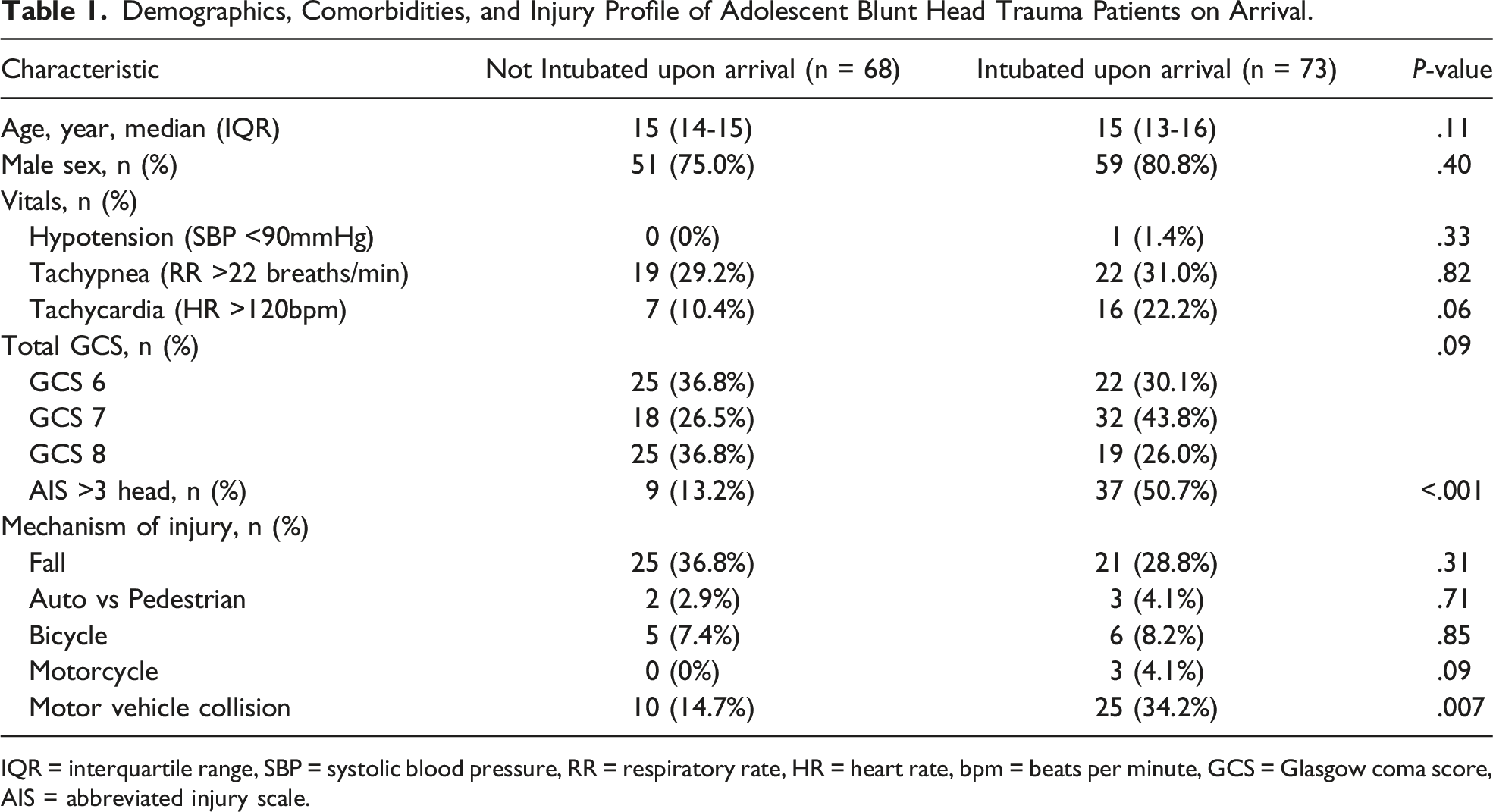
IQR = interquartile range, SBP = systolic blood pressure, RR = respiratory rate, HR = heart rate, bpm = beats per minute, GCS = Glasgow coma score, AIS = abbreviated injury scale.
Alcohol use and substance use are also important factors to consider in the setting of depressed GCS. Of the patients who presented with alcohol screening data upon admission, 45 were intubated upon arrival and 41 were not intubated upon arrival. There was no difference in number of patients who screened positive for alcohol between groups (22.2% vs 34.1%, P = .23). Of the patients who presented with substance use screening data, 32 underwent routine intubation and 29 did not. Like with alcohol, there was no difference in number of patients who screened positive for substance use between groups (43.8% vs 41.4%, P = .85).
Clinical Outcomes and Complications of Adolescent Blunt Head Trauma Patients Intubated and Not Intubated Upon Arrival.
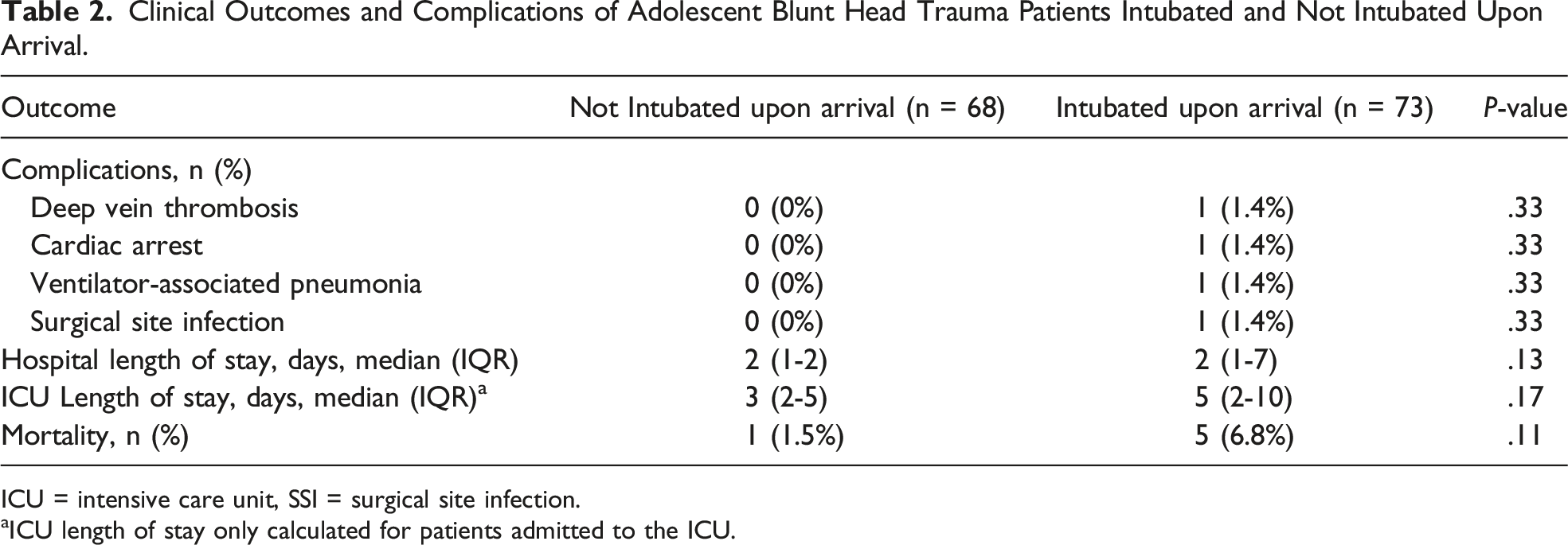
ICU = intensive care unit, SSI = surgical site infection.
aICU length of stay only calculated for patients admitted to the ICU.
Discussion
In this national database analysis of adolescent trauma patients with isolated blunt head trauma, immediate intubation upon arrival was not associated with a higher risk of mortality. This is in direct contrast from prior reports on adult TBI patients where there was increased risk of complications and death when patients with GCS 6-8 were routinely intubated upon arrival.3,10 In addition, this current study of adolescent trauma patients found no differences in hospital or ICU LOS between intubated and non-intubated adolescents.
A depressed GCS can be a marker of significant TBI, and intubation of the trauma patient is associated with significant risk. As such, Jakob et al reported on adult patients with isolated head trauma and a GCS 7-8 on admission and demonstrated that intubation shortly after arrival was associated with a 2-fold higher risk of death. The discrepancy in mortality between adolescents and adults could be attributed to several factors. Successful intubation is dependent on the expertise of the provider who initially attempts intubation, particularly in patients with TBI or reduced GCS because of their increased risk for aspiration and hypoxia. 13 In a study concerning adolescent intubations performed in an adult urban emergency department, Hale et al noted that initial intubation attempts were more likely to be performed by an anesthetist or airway professional of similar level compared to intubations of adult patients. 14 Furthermore, children and adolescents are reported to have a lower incidence of unexpected difficult airway management compared to adults. 15 Difficult airway management and multiple intubation attempts are associated with significantly higher life-threatening complication rates in adult patients, specifically cardiopulmonary collapse. 16 The incidence of a difficult airway in children may be higher as children have smaller airways. It is particularly of note to mention that the incidence of difficult airways in adults and children does not consider field versus in-hospital intubations, so this may be an area for further investigation.
By virtue of their age, adolescent trauma patients are generally healthier with less comorbidities compared to their adult counterparts. In addition, the rate of VAP and ARDS in adolescent trauma patients is far less than that of adults, which may further explain why their outcomes are similar with or without immediate intubation. 16 VAP is one of the most common complications associated with increased mortality in studies examining the outcomes related to immediate intubation in adult patients with TBI and is closely associated with increased injury severity.3,17 The low incidence of VAP in adolescents is confirmed in our study as we only identified one patient in the intubated group that developed VAP.
The rate of most complications are lower in adolescent vs adult trauma patients. Our study demonstrated that adolescent trauma patients with isolated blunt head trauma that were intubated upon arrival had a similar total hospital and ICU LOS compared to their non-intubated counterparts. This is in direct contrast to adult patients, for whom early intubation is associated with longer ICU and overall LOS.3,10 Generally, pediatric trauma patients have a reported complication rate of approximately 4%. 18 This is substantially lower than adult patients (around 10%) even when they present with similar injury severity. 19 The lower complication rates could be attributed to the previously described resilience to inflammatory processes in the pediatric population, which is especially notable because while the most common complications in adult trauma patients are pneumonia, acute respiratory distress syndrome, and sepsis, the most frequent complication in pediatric trauma patients was found to be cardiac arrest. 18 Our study confirms a low overall complication rate among all pediatric patients with isolated head trauma (.02%). The longer LOS in adult patients could be due to the increased risk of complications after intubation, which adolescent and pediatric patients seem to be more resilient towards.
There are several limitations to this study including those that are inherent to database studies such as coding errors and selection bias. Additionally, the TQIP database does not include information on if intubations were performed pre-hospital. Thus, we were not able to elucidate whether attempted intubations performed in the field had any effects on outcomes. Another limitation to our study was the absence of longitudinal data in the database, such as changes in GCS or vital signs from arrival, which were not accounted for despite their potential pertinence as confounding variables. The TQIP database only provided data on admission, which made it challenging to monitor changes in GCS or vital signs over the hospitalization period. The exact reasons for intubation were also not elucidated in the database, so it is unclear whether all patients in the cohort were intubated purely based on GCS alone. Additionally, although we acknowledged potential factors influencing depressed GCS, the TQIP dataset did not offer exhaustive alcohol or substance use screening for pediatric trauma patients. Despite our limitations, our study is strengthened by the fact that it is the first national study to examine the outcomes of immediate intubation based on GCS in adolescents. Studies specifically on the adolescent population are sparse, and greater focus on TBI and intubation outcomes in this population are greatly necessary because TBI is often described as the leading cause of death and disability in youth in the US. 20
In contrast to adults, this national database analysis of adolescent trauma patients with isolated blunt head trauma demonstrated that immediate intubation upon arrival was not associated with a higher risk of mortality. The lack of difference in mortality and hospital/ICU LOS between immediately intubated and non-intubated adolescent patients indicates that current intubation guidelines based on GCS may be upheld in this patient population without marked risks. Additional studies are warranted to corroborate our findings and to further analyze the impacts of provider skill and pathophysiological factors in adolescent routine intubation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.