
Abstract
Objective
To analyze the risk and benefit of bowel preparations in elective colo-rectal surgery.
Background
Mechanical bowel preparations (MBPs) have been popularized in colo-rectal surgery since studies in the 1970s, but recent data has called their use into question and examined complication rates between patients with and without bowel preparations.
Methods
A retrospective case-review was performed consisting of 1237 elective colo-rectal surgeries performed by two surgeons between 2008 and 2021. Patients received either a MBP, a mechanical bowel preparation with oral antibiotics (OAMBP), oral antibiotics alone (OA), or no bowel preparation; some patients across all categories received an enema.
Results
Bowel preparations combined (MBP and OAMBP) totaled 436 patients and showed no statistically significant difference (P > .05) in primary outcomes of wound infection and anastomotic leak when compared to the 636 patients without a bowel preparation and 165 patients with OA. The analysis controlled for comorbidities and presence of enema. Of secondary outcomes, urinary tract infections (UTIs) were significantly more common in patients who received a bowel preparation (P = .047). All other outcomes showed no significant difference between groups, including complications on day of surgery; complications, readmission with and without surgery, and ileus formation within 30 days of surgery; sepsis; pneumonia; and length of stay (LOS). The presence of enemas did not have a statistically significant effect on outcomes.
Conclusions
This study’s data does not support the routine use of MBPs in elective colo-rectal surgery and draws into further question whether MBPs should remain standard of care.
Key Takeaways
• Bowel preparations, despite being standard of care in elective colo-rectal surgeries with anastomoses, did not show any benefit to use and were associated with a significantly higher rate of urinary tract infections in n = 1237 patients. • The use of enemas and oral antibiotics had no significant effect on patient outcomes, but enemas trended towards significance with increased rates of post-operative urinary tract infections and oral antibiotics trended towards significance with increased rates of post-operative pneumonia. • The use of routine bowel preparations is not supported by this data.
Introduction
Mechanical bowel preparations (MBPs), which facilitate the mechanical removal of intestinal contents, were first suggested by Sir William Halstead in the 1880s to address high infection rates in colo-rectal surgery. 1 Even today, literature finds a weighted mean of 11.4% of colo-rectal surgeries result in surgical site infection (SSIs), 2 along with 8.1% of anastomoses resulting in anastomotic leak. 3 Historically, these issues were addressed in the 1970s by two landmark studies that examined oral antibiotics (OA) alone and mechanical bowel preparations with oral antibiotics (OAMBPs). In 1973, Nichols’ study indicated that pre-operative neomycin and erythromycin reduced surgical site infections (SSIs). 4 Four years later, Clarke combined the erythromycin-neomycin with MBPs and found reduced SSIs and anastomotic leak. 5 Following these publications, BPs became standard of care and have since been supported by a significant body of work.6–11 The most recent (2019) American Society of Colon and Rectal Surgeons’ clinical practice guidelines for bowel preparation in elective colo-rectal surgeries still recommends OAMBPs as standard of care. 2
Though some early studies questioned the colo-rectal surgical field’s adherence to bowel preps—notably Hughes’ 1972 analysis 12 which concluded that the “omission of enemas and bowel washes from the pre-operative procedures will be welcomed by both patients and nursing staff”—the bulk of the data questioning MBPs has been in the last fifteen years.13–20 Of particular note, the most recent Cochrane review examined 18 studies totaling over 5000 patients and found no benefit to MBPs or enemas. 13 Another meta-analysis of seven studies totaling 1454 patients found a significantly higher rate of anastomotic leak in patients that had received MBPs. 14
Given the conflicting literature, in addition to poor patient tolerance and adherence, we aimed to evaluate the use of BPs in elective colo-rectal surgery and its effect on several post-surgical outcomes following a retrospective review of patients at one center over 13 years.
Methods
This study was reviewed and approved by the Institutional Review Board at Essentia Health Duluth with no reported considerations. We performed a retrospective review of 1237 elective colo-rectal surgeries with anastomoses performed by two surgeons at the same center using similar techniques between 2008 and 2021. The same surgical techniques were used between surgeons and the post-operative protocols were identical. We examined outcomes between three primary variables: patients who received a bowel preparation (either an MBP or an OAMBP), patients without a bowel preparation, and patients who received OA only. Some patients from all categories, though primarily rectal and sigmoid resections, also received an enema, which became a secondary variable of analysis along with comparing open and minimally invasive surgeries (MIS).
The surgeries we examined included partial colectomy with primary colocolonic, ileocolic, rectal, or low colo-rectal anastomoses; total proctocolectomy with ileoanal pouch; total abdominal colectomy with ileorectal anastomosis; subtotal colectomy with anastomosis; and colostomy reversals with anastomosis. Enemas given to patients examined in this study were self-administered fleets enemas, in the pre-operative area the morning of surgery. Data involving the methods of surgery, both open and MIS (laparoscopic and robotic combined) were collected.
The primary outcomes measured were SSI and anastomotic leak. Secondary outcomes included urinary tract infection (UTI), Clostridium difficile (C. difficile) infection, ileus formation, complications within 30 days, readmission for any reason, sepsis, pneumonia, and length of stay (LOS).
The data were analyzed using a general estimating equation (GEE), with a GEE mean for the quantitative variable (LOS) and a GEE binary logistic model for the remaining outcome variables. Length of stay was analyzed by ranking, with median considered to be a ranked score of 619; for example, scores above 619 indicate a cohort of patients that stayed longer than the mean of 5.9 days (with two significant outliers excluded). A standard 95% confidence interval (CI) was considered significant. A multivariate analysis was conducted and we controlled for influential covariates including age, gender, and patient comorbidities. Comorbidities included congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), and renal disease (any stage of CKD).
Results
The cohort was 51.1% female; 43.6% of patients had renal disease; 22.6% had CAD; and 13.5% had CHF. Specific data were unable to be collected on race, but the patient cohort had an overwhelming majority of Caucasian patients. For context, per the US census, St. Louis County, where Duluth, MN is located, is demographically 88.0% White, 4.8% two or more races, 2.2% Native American, 2.0% Black or African American, 1.8% Hispanic or Latino, .9% Asian, and .3% other. 21 The study population came from a majority rural area, with a catchment area that extends from the upper peninsula of Michigan to North Dakota, covering primarily rural northern Minnesota and Wisconsin. 22
Bowel preparation type cohorts by method of surgery and percent with enema.
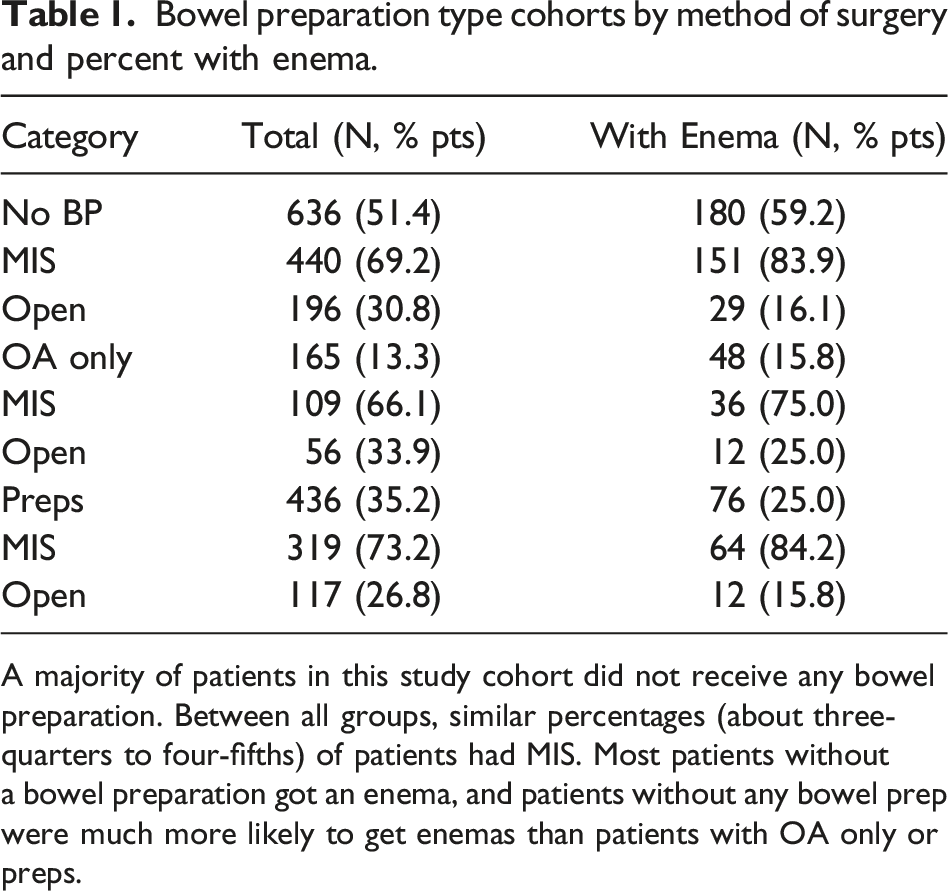
A majority of patients in this study cohort did not receive any bowel preparation. Between all groups, similar percentages (about three-quarters to four-fifths) of patients had MIS. Most patients without a bowel preparation got an enema, and patients without any bowel prep were much more likely to get enemas than patients with OA only or preps.
Multivariate analysis: Significance of bowel preparations, OA, Enemas, and Open surgery by secondary outcomes.
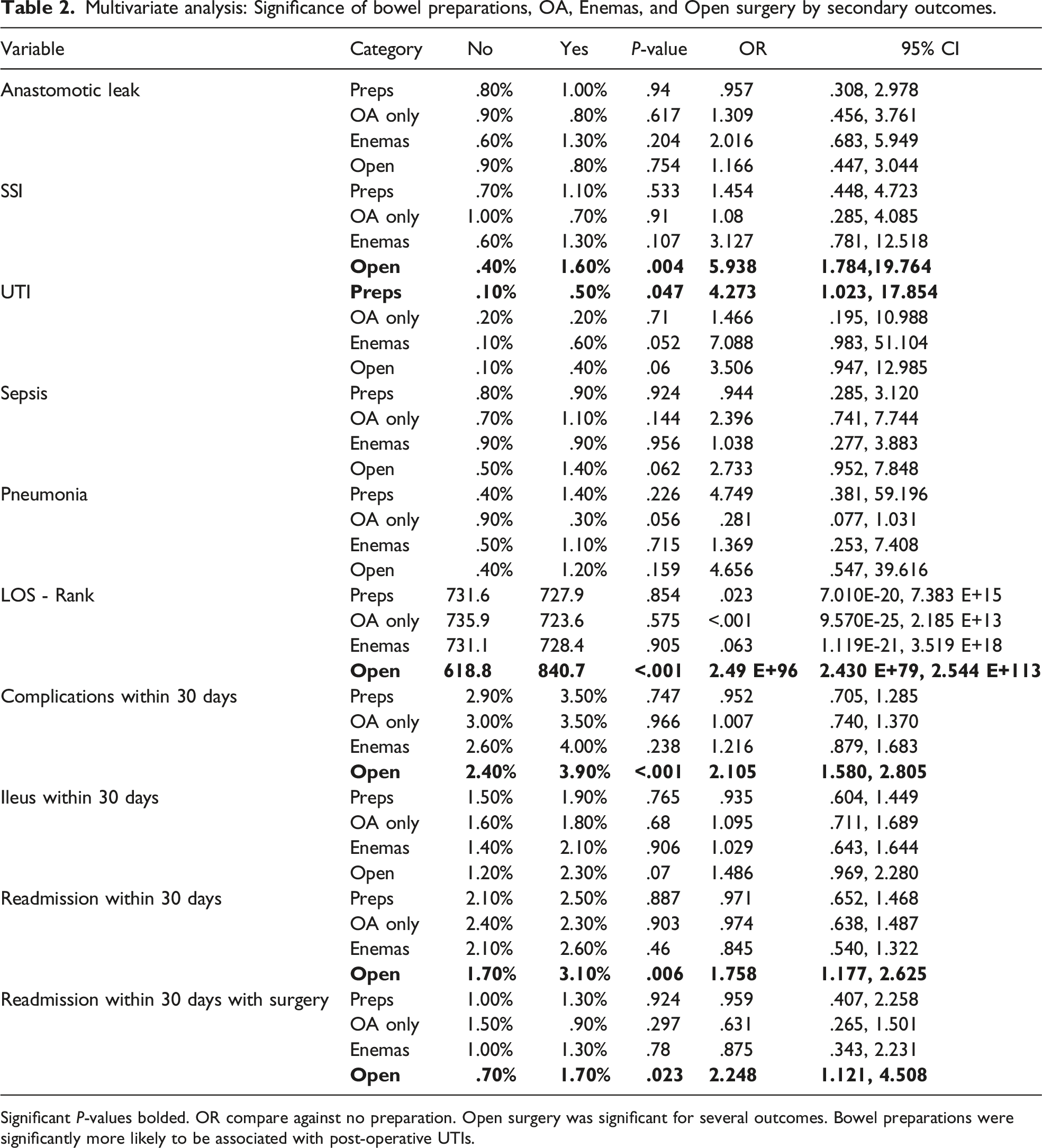
Significant P-values bolded. OR compare against no preparation. Open surgery was significant for several outcomes. Bowel preparations were significantly more likely to be associated with post-operative UTIs.
Statistical significance of influence of covariates on secondary outcomes.
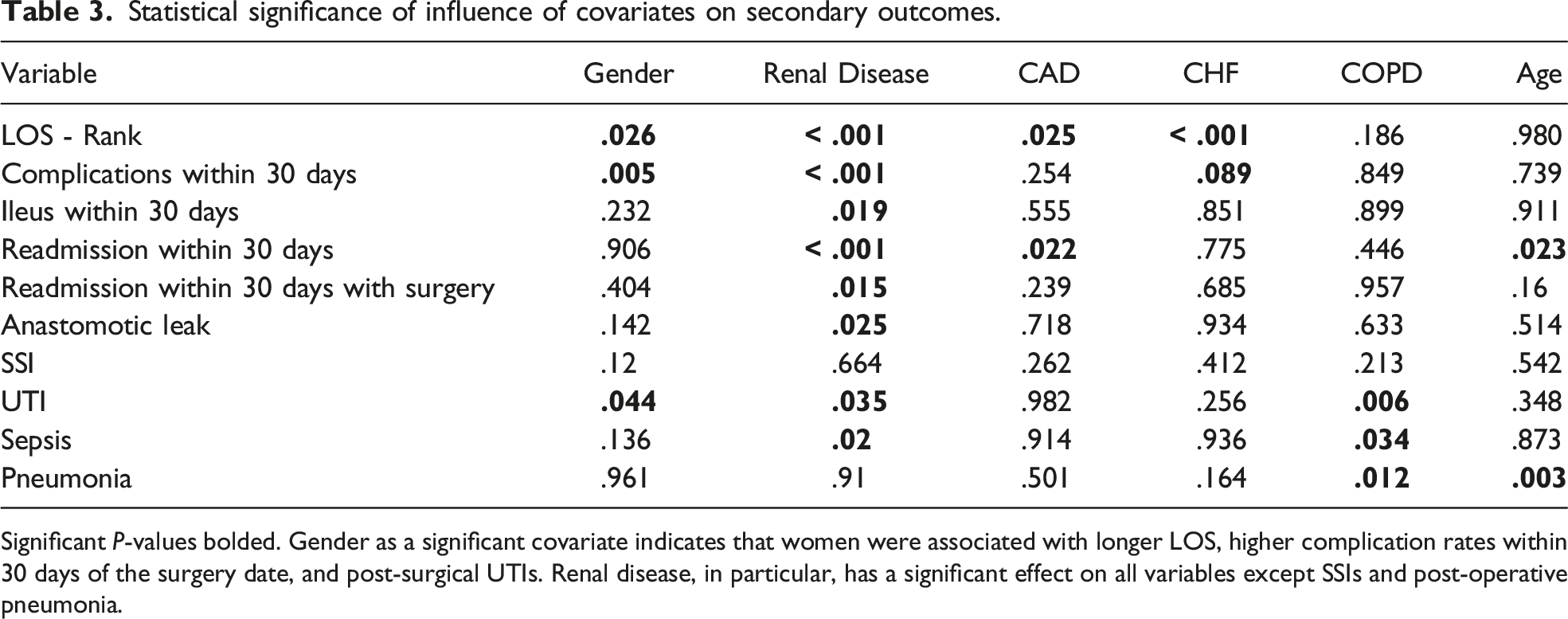
Significant P-values bolded. Gender as a significant covariate indicates that women were associated with longer LOS, higher complication rates within 30 days of the surgery date, and post-surgical UTIs. Renal disease, in particular, has a significant effect on all variables except SSIs and post-operative pneumonia.
The incidence of C. difficile infection was too low during the study period to analyze C. difficile infection with regards to bowel preparations.
Discussion
Our study data did not show any significant benefit to MBPs, OAMBPs, or OA use and showed a statistically significant association between bowel preparations and increased post-operative UTIs (Table 2). Additionally, there were no associations with negative outcomes found in not performing bowel preparations prior to these elective colo-rectal procedures.
Six significant covariates were found in multivariate analysis: gender, renal disease, CAD, CHF, COPD, and patient age. The latter five are known risk factors, but further research is warranted into why gender was a significant covariate for LOS, complication rate within 30 days of surgery, and post-operative UTIs. One potential explanation is that women are more likely to develop UTIs, thus raising the rate of post-operative complications and potentially increasing LOS. The effect of gender may therefore also influence the association noted between bowel preparations and increased post-operative UTIs, though gender did not affect when Foley catheters were removed. However, other confounding factors may influence the gender differences found in this data. While the other covariates are unsurprising in their influence, it is noteworthy that renal disease was found to be a significant association with so many negative outcomes, especially compared to the other covariates.
The data showed several correlations between open surgeries and negative outcomes, along with a few trends towards significance. While there is likely merit to the correlations, the confounding variable is that the cases that were performed open were likely done due to increased complexity and were more likely to develop complications. Though we have attempted to control for this in our analysis, it is possible that this confounder is still influencing the data.
There are several limitations to this study. Our data is retrospective and does not differentiate between MBPs and OAMBPs. Further, incidence of the outcomes of interest was low enough that many of the secondary outcomes were relatively underpowered, with large confidence intervals, despite a large sample size (N = 1237). This meant that some of our data trended towards significance, rather than being more definitively significant or not significant (P-values between .05 and .10). Open surgery trended towards significance in several outcomes. Additionally, enemas trended towards a significant association with increased rates of post-operative UTIs and oral antibiotics trended towards a significant association with increased incidence of post-operative pneumonia. These issues warrant further research to distinguish between MBPs and OAMBPs along with greater study size values to better examine the data trends and the effect of preps and OA on C. difficile infection.
Sir William Halsted, the original proponent of bowel preparations nearly a century and a half ago, attributed infection as “manifestly from the contents of the intestine.” 1 Despite Dr. Halsted’s warning against anastomotic leak, we found that anastomotic leak and SSI rates, our primary outcomes, were not statistically significant with regards to bowel preparations. Though much of Sir Halstead’s work has become foundational material to the surgical field, and bowel preparations are currently regarded as a standard of care, the null hypothesis that outcomes were not influenced by bowel preparations was upheld and our data does not support the use of bowel preparations in elective colo-rectal surgery.
Footnotes
Acknowledgments
Special thanks to Colleen Renier, biostatistician at Essentia Health, for performing the statistical analyses, and to the Northern Rural Plains Surgical Society for allowing this study to be presented at the annual meeting and supporting this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.