
Abstract
Background
Central venous line (CVL) placement in children is often necessary for treatment and may be complicated by central line-associated bloodstream infection (CLABSI). We hypothesize that line type and clinical and demographic factors at line placement impact CLABSI rates.
Methods
This is a single-institution case-control study of pediatric patients (≤18 years old) admitted between January 1, 2015, and December 31, 2019. Case patients had a documented CLABSI. Control patients had a CVL placed during the study period and were matched by sex and age in a 2:1 ratio. Bivariate and multivariate logistic regression analysis was performed.
Results
We identified 78 patients with a CLABSI and 140 patients without a CLABSI. After controlling for pertinent covariates, patients undergoing tunneled or non-tunneled CVL had higher odds of CLABSI than those undergoing PICC (OR 2.51, CI 1.12-5.64 and OR 3.88, CI 1.06-14.20 respectively), and patients undergoing port placement had decreased odds of CLABSI compared to PICC (OR .05, CI 0.01-.51). There were lower odds of CLABSI when lines were placed for intravenous medications compared to those placed for solid tumor malignancy (OR .15, CI .03-.79). Race and age were not statistically significant risk factors.
Discussion
Central lines placed for medication administration compared to solid tumors, PICC compared to tunneled and non-tunneled central lines, and ports compared to PICC were associated with lower odds of CLABSI. Future improvement efforts should focus on PICC and port placement in appropriate patients to decrease CLABSI rates.
Key Takeaways
• There is a difference in CLABSI rates depending on line type and key clinical factors. • Line selection in the setting of primary diagnosis leading to central access need has the potential to improve CLABSI rates in a pediatric population. • For short-term access, PICCs are preferred over non-tunneled or tunneled central lines and for long term not requiring daily access, ports are preferred.
Introduction
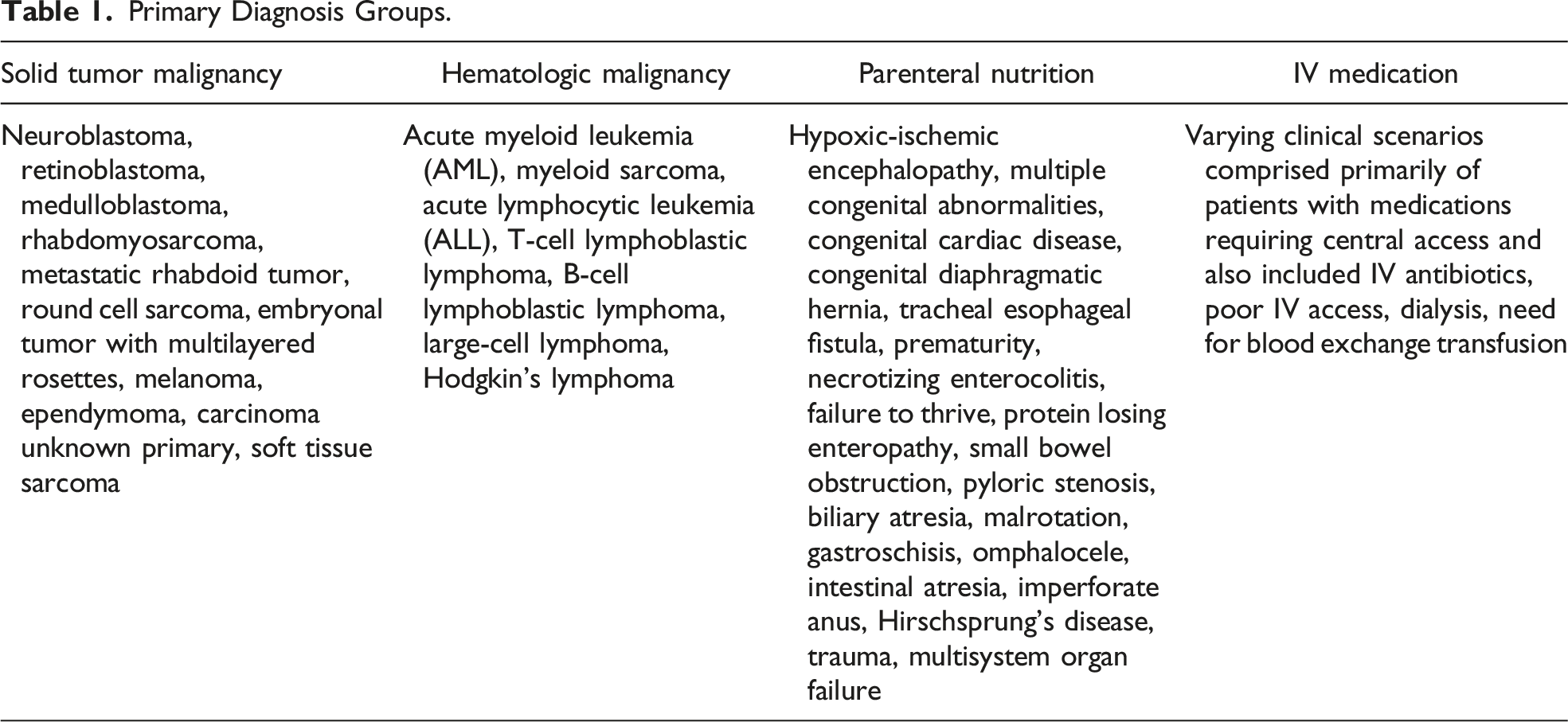
Central venous line (CVL) placement in children is necessary for a multitude of diagnoses, including cancer, infection, and malnutrition. Previous studies have estimated that 5 million pediatric CVLs are placed yearly. 1 However, CVL placement can be associated with infectious complications. These central line-associated bloodstream infections (CLABSIs) are a significant cause of increased morbidity and mortality.2–4 Central line-associated bloodstream infections are among the most costly hospital-acquired infections. 5
There are 4 main types of CVLs, and each can be used depending on the treatment and duration needed. 6 These include completely implantable CVLs with a subcutaneous access port that can be used intermittently, also known as a “port.” Tunneled CVLs have an exposed hub and can be utilized when frequent or daily access is required. Both ports and tunneled CVLs can be used for long-term access. Non-tunneled CVLs can be used temporarily, as can peripherally inserted central catheters (PICCs). However, there is little consensus on the definition of temporary and long term; additionally, the effect size of line selection on CLABSI rates is unknown.
Decreasing CLABSI rates is an active area of quality improvement and research efforts. 3 Implementation of CLABSI-prevention bundles have been shown to effectively decrease CLABSI rates.7,8 These bundles vary from institution but typically consist of maximum sterile barrier precautions during insertion, properly cleaning the skin with chlorhexidine, application of sterile dressings, regular maintenance of lines with aseptic technique while in place, and promptly removing the line when no longer clinically indicated. 9 While bundles have proven effective for reducing the risk of CLABSI, there are little data on CLABSI rates based on CVL type, clinical indication, and patient factors to assist with targeted improvement efforts.
We hypothesize that pre-operative clinical factors, line site, and type of CVL are associated with CLABSI rates.
Methods
Data Collection
This study was reviewed and approved by the University of North Carolina (UNC) Institutional Review Board (IRB# 20-0569). This was a retrospective single-institution case-control study conducted at UNC Children’s Hospital from January 1, 2015, to December 31, 2019. Patients were included in the study if they were ≤18 years old and had a central line placed at our institution during the study period. Hospital epidemiology database were queried for case patients (positive CLABSI) during the study period. The Carolina Data Warehouse for Health at UNC was queried for CPT codes for central line placement during the study period, and then we generated a list of matched controls in a 2:1 ratio by sex and age.
Primary Diagnosis Groups.
Statistical Analysis
Differences in demographic and clinical covariates by CLABSI status were assessed using descriptive statistics. Statistical comparisons of differences were generated using Wald chi-square tests for categorical variables and differences in means were generated using student’s t test. Demographic and clinical factors were also examined during multivariate logistic regression analysis. Akaike information criterion (AIC) and likelihood ratio tests (LRTs) were used to determine which covariates should be included in the final model. The final model included primary diagnosis (categorized as solid tumor, AML/ALL, malnutrition, or other IV antibiotics and/or medications), race (categorized as white, black or others), age (continuous), and line type (categorized as PICC, tunneled, non-tunneled, or port). Statistical significance was set at a P-value of <.05. All analyses were performed using SAS software version 9.4 (SAS Inc., Cary, NC, USA).
Results
Patient Demographic and Clinical Characteristics.
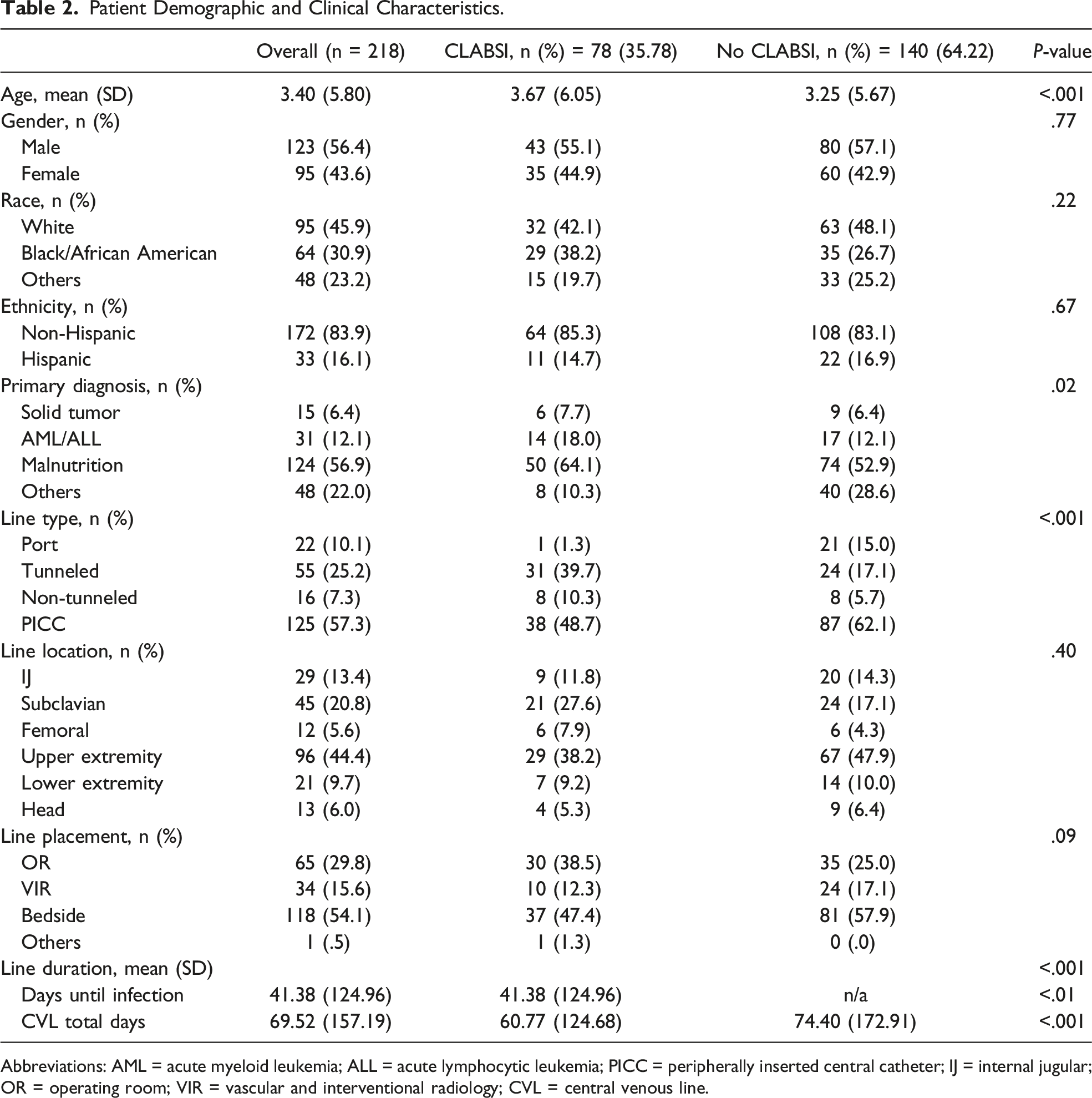
Abbreviations: AML = acute myeloid leukemia; ALL = acute lymphocytic leukemia; PICC = peripherally inserted central catheter; IJ = internal jugular; OR = operating room; VIR = vascular and interventional radiology; CVL = central venous line.
Risk Factors Associated With Pediatric (≤18 years) CLABSIs.
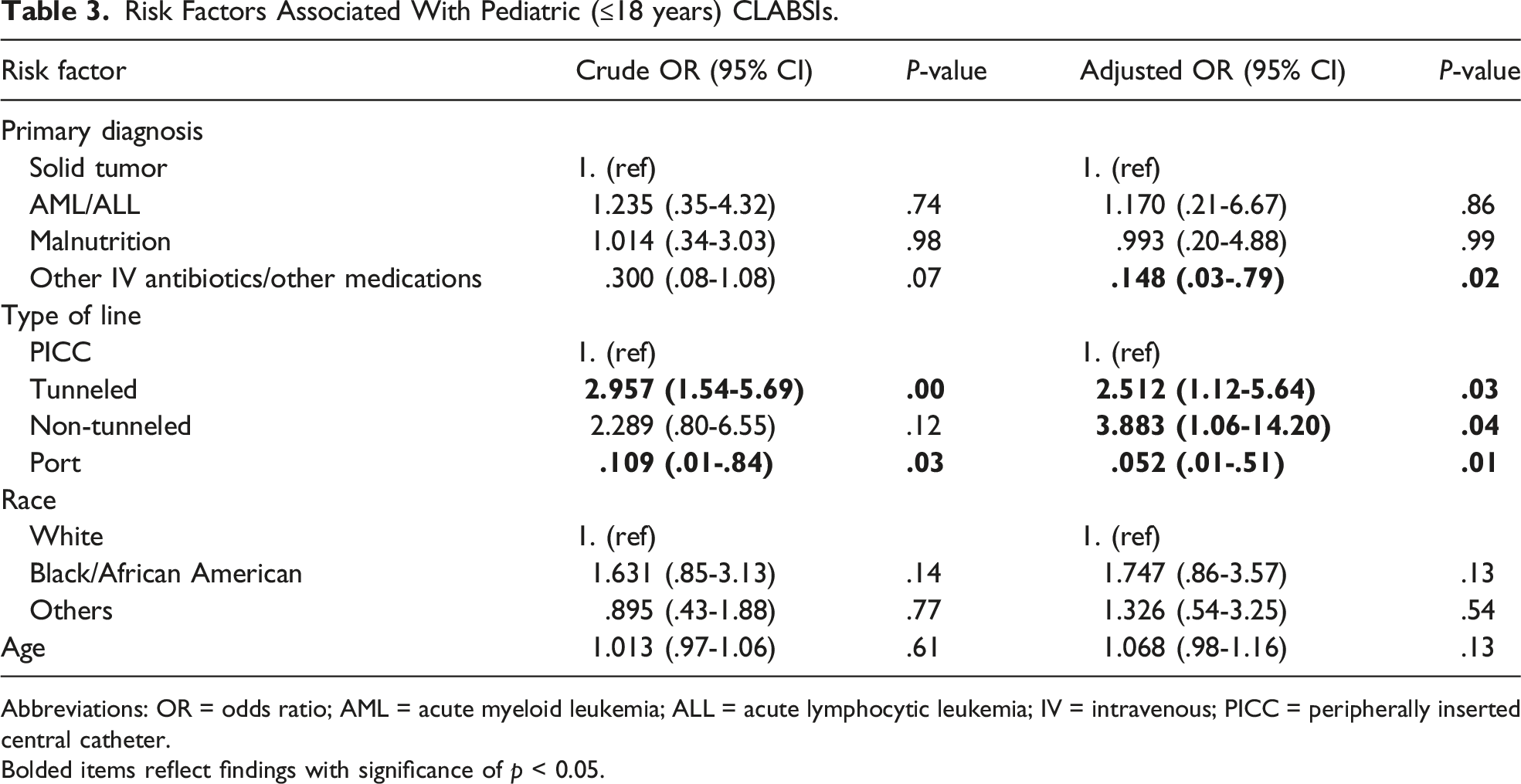
Abbreviations: OR = odds ratio; AML = acute myeloid leukemia; ALL = acute lymphocytic leukemia; IV = intravenous; PICC = peripherally inserted central catheter.
Bolded items reflect findings with significance of p < 0.05.
Discussion
We found that after controlling for pertinent covariates, tunneled and non-tunneled CVLs have higher odds of CLABSI than PICCs, ports have lower odds of CLABSI than PICCs, and lines placed for IV medication administration are safer with lower odds of CLABSI than when placed for solid tumors. The results of this study show that there is a difference in CLABSI rates depending on line type and key clinical factors, and we also demonstrate the effect size of line selection. Line selection in the setting of primary diagnosis leading to central access need has the potential to improve CLABSI rates in a pediatric population, and to guide patient and parental counseling about risks associated with needed procedures.
The use of PICCs has been increasing over the past several decades,10–12 and there are many benefits of PICC placement in children including easier placement and reduced need for general anesthesia. 13 Previous data regarding the safety of PICC lines raised concerns about their safety profile;14,15 however, there have been many studies and a recent systematic review that have shown PICCs to be a safe option for central access in the pediatric population.13,16,17 In our participants, we found a decreased odds of CLABSIs in PICCs compared to both tunneled and non-tunneled CVLs. Our incidence rate of CLABSI with PICC placement was 30.4%, and this is slightly higher than the average reported incidence in Bahoush et al 16 of 16.4% to 28.8%. Our finding has clinical implications when surgeons are making line selection decisions for short term and intermediate central access. Given PICC’s lower odds of CLABSI compared to both tunneled and non-tunneled CVLs, they should be used preferentially for patients not requiring long-term access (additional studies are still needed to define long vs intermediate vs short term).
Our study showed that ports have lower odds of CLABSI compared to PICCs, regardless of primary diagnosis. This is fitting with other studies that have shown lower rates of CLABSIs in patients with port access.6,18,19 Some institutions place PICCs at the time of diagnosis of malignancy with a plan to transition to port placement after induction chemotherapy, but our data do not support this practice, and randomized trials examining this practice are needed. Additionally, we did not find a difference in the rates of CLABSI in neutropenic patients with ports. A recent study by Elgarten et al 20 found no difference in CLABSI rates by CVL type in neutropenic patients. Hence, our data support the selection of port as the preferred long-term central access in pediatric patients that do not require daily access. This is in agreement with prior studies suggesting preferential selection of port for central line access in patients with malignancy and stem cell transplantation, even in the presence of neutropenia.19–21
Our finding of decreased odds of CLABSI in children requiring line placement for medication administration compared to those with solid tumor malignancy is consistent with the published literature and supports the validity of findings and the generalizability of our approach. While primary diagnosis is not a modifiable risk factor, our data support the development of diagnosis-specific CLABSI bundles as a future improvement project for high-risk groups. 22
Our study has limitations. First, the retrospective nature of this study makes causality difficult to confirm. Our line type groups were not equally distributed with significantly more in the PICC group and few in the port group; this likely reflects clinical practice with PICCs being one of the most common central lines in pediatric inpatients. 23 We did not control for the presence of pre-existing antibiotics within the line type groups. The study uses administrative data to assign patients to either case or control study groups; this can be associated with misclassification or other biases. We believe that in this case, this misclassification was ameliorated by supplemental manual chart review and correction of errors; however, patients who have CLABSIs at an outside institution or who were not included in our administrative databases at selection may potentially bias our results.
In conclusion, our study supports PICC utilization compared to tunneled and non-tunneled CVLs in patients with short-term need for central venous access. In patients with long-term CVL needs who do not require daily access, port is preferred, regardless of diagnosis or neutropenia. Patients requiring CVL placement for chemotherapy have a higher odds of CLABSI than those needing CVL for medication administration and should be a focus of future improvement efforts. Finally, we highlight that the timing and placement of CVL in pediatric patients should be an individualized decision based on patient needs and clinical factors.
Supplemental Material
Supplemental Material - Central Line-Associated BloodstreamInfection Risk Factors in a PediatricPopulation
Supplemental Material for Central Line-Associated BloodstreamInfection Risk Factors in a PediatricPopulation by Hannah E. Trembath, Deanna M. Caruso, Sean E. McLean, Adesola C. Akinkuotu, Andrea A. Hayes Dixon, and Michael R. Phillips in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.