
Abstract
Background
It remains controversial whether mesh should be fixed during laparoscopic inguinal hernia repair. A systematic review and meta-analysis of randomized-controlled trials (RCTs) was conducted to compare fixation and nonfixation in laparoscopic groin hernia repair.
Methods
A registration was listed with PROSPERO (International Prospective Register of Systematic Reviews; registration no. CRD42022350469). Databases including PubMed, Embase, Cochrane Library, and ClinicalTrials.gov were searched to identify RCTs comparing fixation with nonfixation in laparoscopic groin hernia repair. The primary outcomes were postoperative pain at 24 hours and recurrence. Secondary outcomes were mean operative time, urinary retention, and postoperative pain at 6 months.
Results
A total of 18 trials, including 2617 patients with 2878 hernias, were included in this meta-analysis. In contrast to the fixation group, the nonfixation group was associated with lower postoperative pain scores at 24 hours and 6 months, a shorter mean operative time, and a lower incidence of urinary retention. There were no significant differences between the 2 types of procedures in terms of the rate of recurrence for patients with an inguinal hernia orifice smaller than 4 cm in size.
Conclusions
The nonfixation technique is an effective method to reduce urinary retention, mean operative time, and postoperative pain at 24 hours and at 6 months; however, the rate of recurrence was comparable to that of the fixation method.
Introduction
The first known record of inguinal hernia was made by the Egyptians, who referred to it as “a swelling on the surface of a belly.” Over the centuries, many treatment methods for inguinal hernia have been attempted, including hernia truss, testicular excision, repair with tension, and repair without tension. 1 The invention of the laparoscope facilitated repair from behind the floor of the inguinal canal via the total extraperitoneal approach (TEP) or the transabdominal preperitoneal approach (TAPP). Approximately 27% of men and 3% of women will develop a groin hernia during their life time, with surgery being the only cure. 2 Therefore, optimizing the surgical procedure is of great importance. Compared with the open surgery approach, laparoscopy may be associated with less postoperative pain, shorter hospital stays, and a quicker return to baseline activities, and thus this technique has steadily gained popularity. Sehultz et al were first to report the use of a piece of mesh to cover the inguinal area in the preperitoneal space and the application of a plug insertion in the inner ring. 1 This technique was subsequently improved by removing the plug, increasing the mesh size, and fixing the mesh, resulting in a 2-year recurrence rate of 25%. However, fixation, such as that with staplers or tackers, has been associated with complications of nerve injury and chronic pain. While some reports have suggested that fixation reduces recurrence by immobilizing the mesh, the associated chronic pain may warrant further repeated surgery, with yet uncertain effects. A previous meta-analysis in 2012 comprising 8 randomized-controlled trials (RCTs) showed no statistical difference between patients who had undergone fixation and those with no fixation in terms of chronic groin pain, recurrence, operating time, postoperative pain, postoperative complications, or hospital stay. 3 Since then, numerous related RCTs have been published with conflicting results. We thus conducted an updated comprehensive systematic review and meta-analysis that compared mesh fixation and nonfixation during laparoscopic inguinal hernia repair.
Methods
This systematic review and meta-analysis were performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020) checklist. 4 A research protocol was created and registered with PROSPERO (International Prospective Register of Systematic Reviews; registration no. CRD42022350469).
Eligibility Criteria
Only RCTs comparing the outcomes of mesh fixation and nonfixation during the laparoscopic procedure were included in this study. Male or female patients, aged 18 years or older, who underwent laparoscopic inguinal repair, either TEP or TAPP, were included. Patients who treated with the fixation technique were considered the control cohort, while patients treated with the nonfixation technique were consider the trial cohort. Randomized-controlled trials that evaluated fixation via tackers or staplers were included, and studies that assessed other forms of fixation, such as glue, suture, or sealant, were excluded. Participants with a hernia orifice bigger than 4 cm and those with strangulated hernias were excluded. Duplicate articles, review articles, case reports, and animal trials were excluded. Data regarding postoperative pain at 24 hours and 6 months, recurrence, mean operation time, and urinary retention were collated.
Search Strategy
A comprehensive literature search was conducted on May 6, 2022, of the following online databases: PubMed, Embase, Cochrane (CENTRAL), Web of Knowledge, Google Scholar, and ClinicalTrials.gov. There was no language restriction. The lists of references in the retrieved literature were also screened for possibly eligible trials. The following terms were searched: the medical subject heading (MeSH) terms “inguinal hernia,” “laparoscopy,” and “groin”; and the text terms “fix*” and “non-fix*.”
Data Extraction
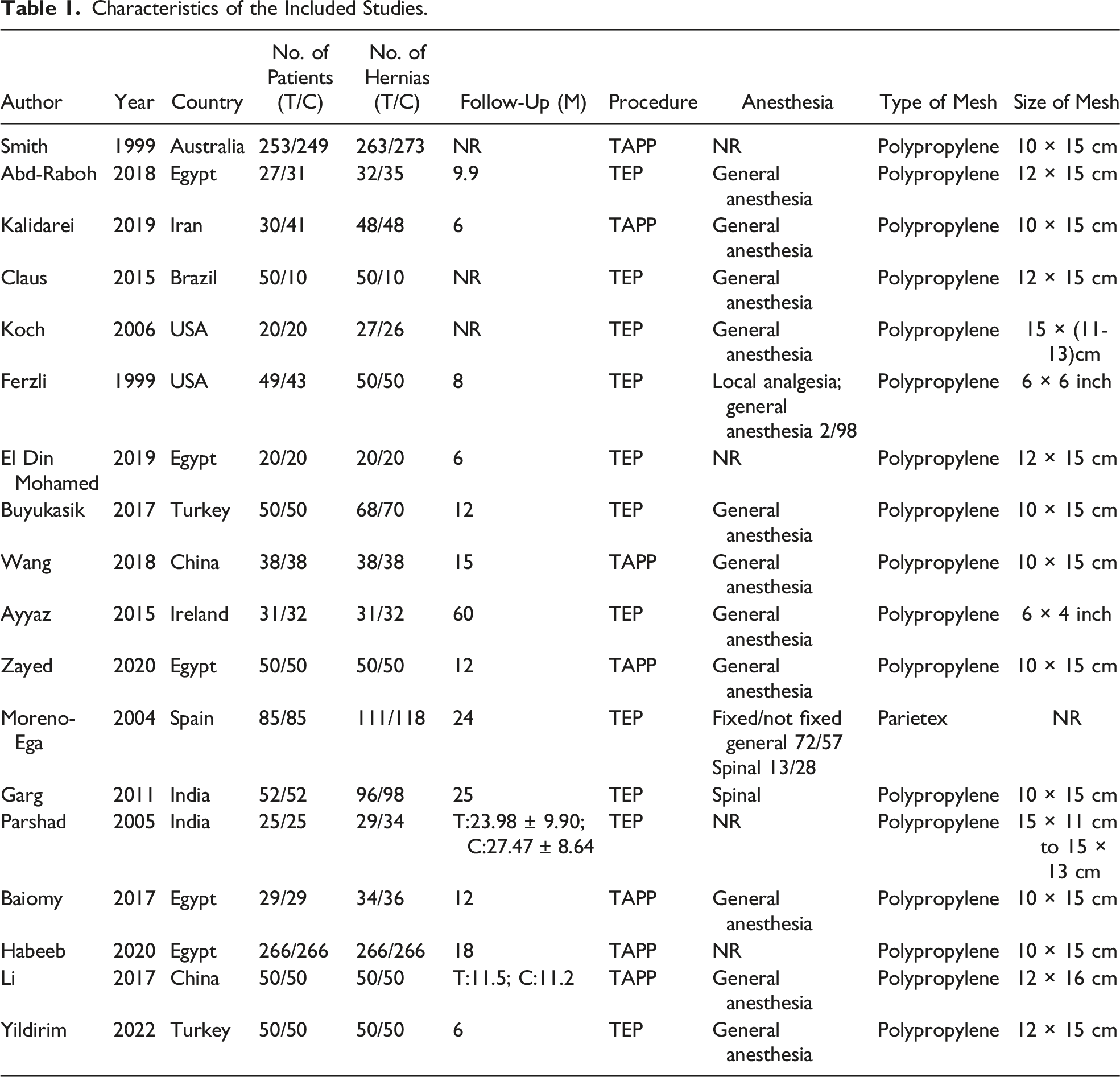
Two independent researchers (Bo Yang and Gaopeng Hao) reviewed the titles and abstracts. If eligible, the full text was obtained for further assessment. Any disagreements were resolved through discussion, and if agreement still could not be reached, a third reviewer (Yinquan Wang) was consulted to reach a consensus. Two reviewers (Bo Yang and Gaopeng Hao) performed the data extraction and recorded the information onto a Microsoft Excel sheet with passwords. The following information from eligible trials was collated: first author, country, publication year, number of patients, number of hernias, mean follow-up time, weight or body mass index (BMI), procedure, anesthesia, mesh type, mesh size, postoperative pain at 24 hours, postoperative pain at 6 months, mean operative time, urinary retention, and recurrence.
Quality Assessment
Two independent reviewers used the Cochrane Collaboration tool to assess the risk of bias, including selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias. 5 Any discrepancies were resolved via discussion with a third reviewer (Yinquan Wang).
Statistical Analysis
Postoperative pain at 24 hours (assessed using the visual analog scale [VAS]), mean operative time, and postoperative pain at 6 months (VAS) were considered continuous variables. The mean difference was calculated with 95% confidence intervals (CIs) between 2 groups. The relative risk, with 95% CIs, was calculated for dichotomous outcomes, including urinary retention and recurrence.
All extracted data from eligible trials were recorded in Review Manager software (version 5.4, Cochrane) for construction of forest plots and funnel plots, and some data were subjected to the Egger’s test via an independent assessor using Stata software (StataCorp). For outcomes with significant heterogeneity between groups, the random-effects model was used, while the fixed-effects model was applied for cases of insignificant inconsistency. Interestingly, there was always heterogeneity between studies for 1 identical outcome. Therefore, the Cochran Q test and I2 test were used to evaluate these data. 6 The numerical value of I2 represents the magnitude of the inconsistency. According to Higgins, an I2 greater than 50% suggests moderate-to-high heterogeneity. 7 For any outcomes included in more than 10 studies, funnel plots were constructed and the Egger test was performed to estimate publication bias graphically and quantitatively. Sensitivity analyses were performed where heterogeneity was substantial and statistics appeared significant. We resynthesized the data after eliminating one study at a time to examine the robustness of the results.
Results
Study Selection
A total of 1112 articles were retrieved from the initial literature search (Figure 1). After the exclusion of 431 duplicate records, 11 animal trials, 540 irrelevant articles, 22 case reports, and 31 reviews, a total of 64 potential studies remained. The full articles were reviewed, and a total of 46 articles were removed in accordance with the exclusion criteria. Finally, 18 trials, including 2617 patients with 2878 hernias, satisfied the inclusion criteria and were included in the meta-analysis. PRISMA flowchart of the literature selection process.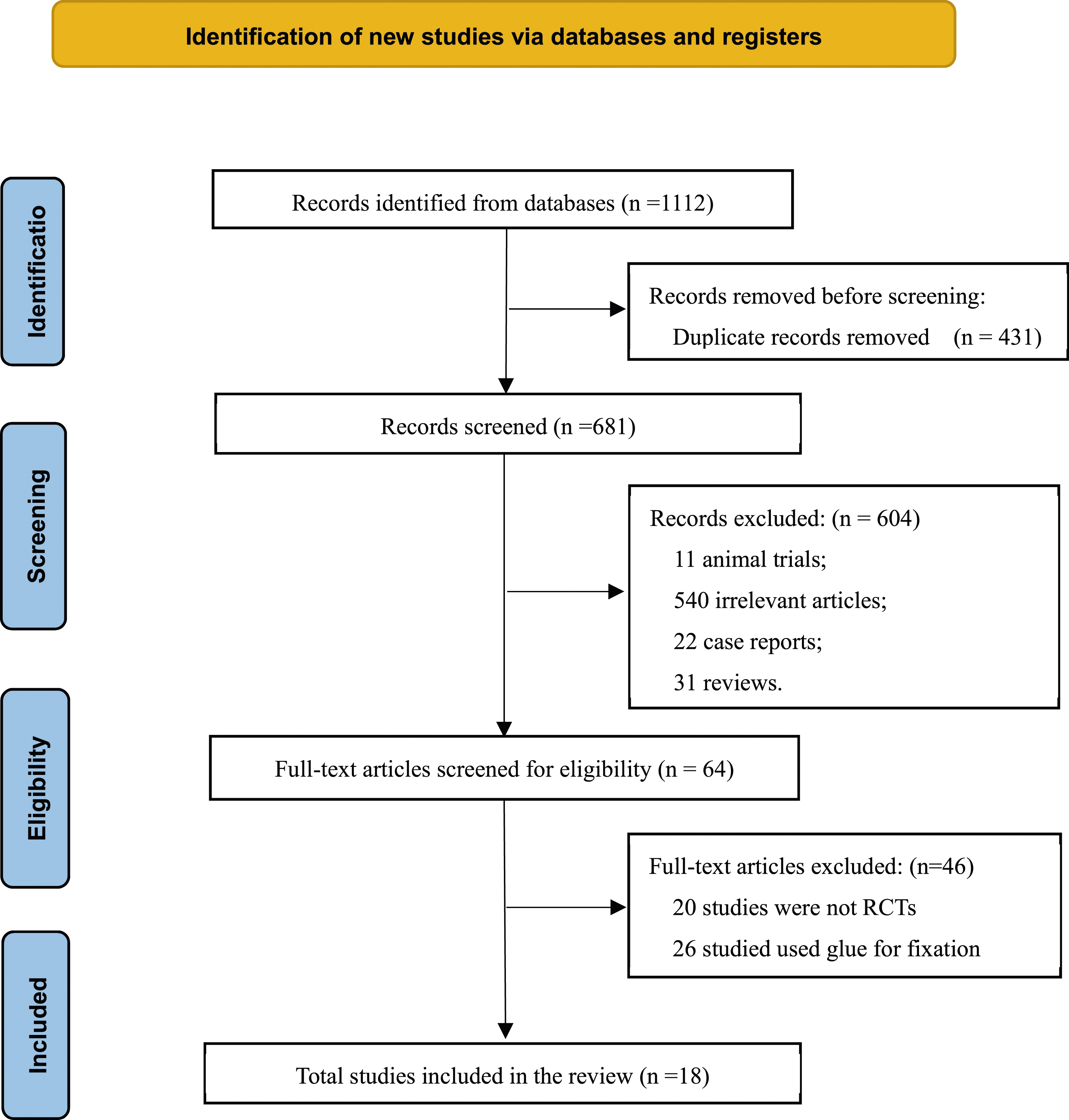
Study Characteristics
Characteristics of the Included Studies.
Risk of Bias
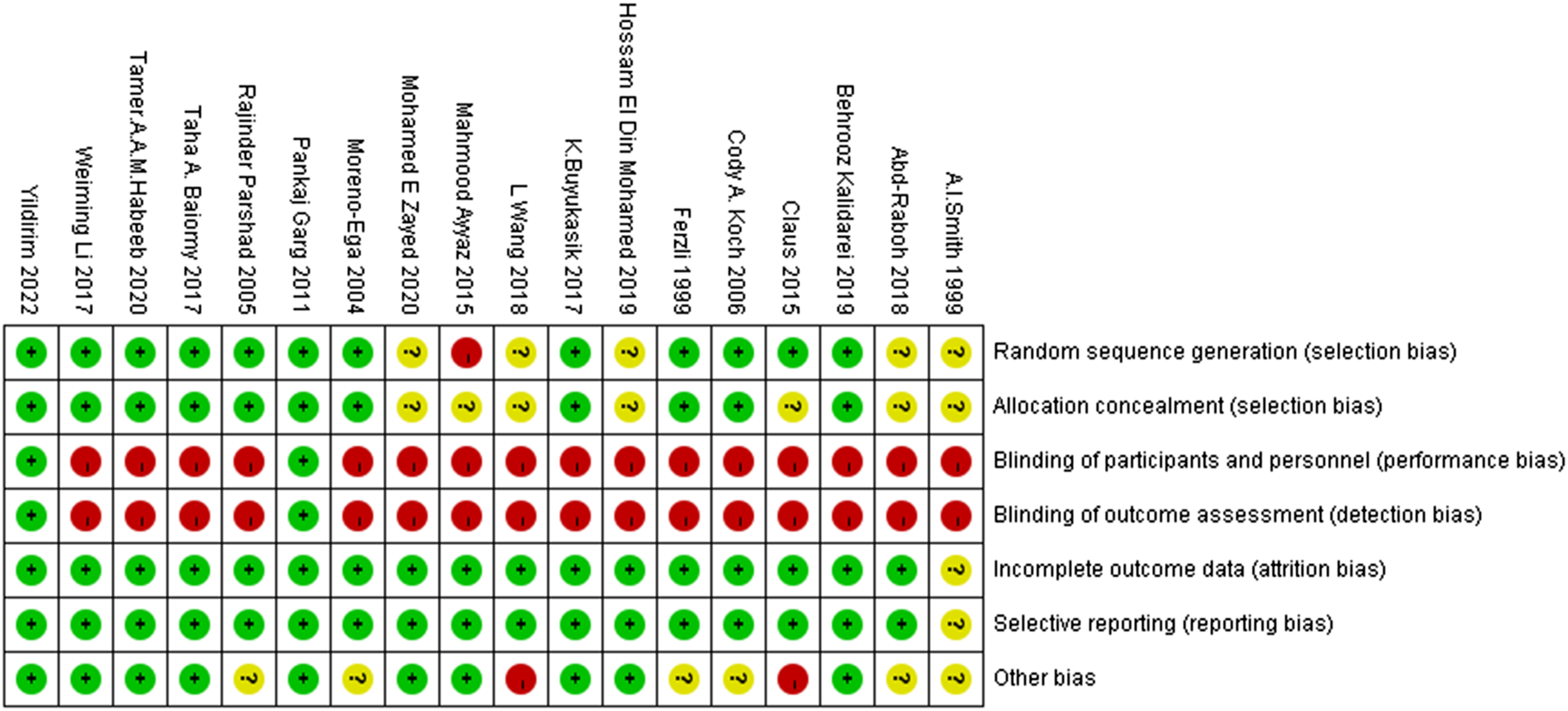
Figures 2 and 3 display the results of the quality assessment. Attrition bias and reporting bias were high in all 18 studies except in the study by Smith et al.
9
The blinding of both participants and personnel and that of outcome assessors were only fully described by Garg et al
15
and Yildirim et al.
17
Ayyaz et al
18
divided participants using the lottery method into even and odd which was considered to involve a high risk of selection bias, whereas proper random sequence generation was explicitly described in 12 articles and omitted in 5 studies. Allocation concealment was conducted appropriately in 11 reports and unclear in the remaining records. Risk of bias summary. Risk of bias graph. +, low risk of bias; −, high risk of bias; ?, uncertain risk of bias.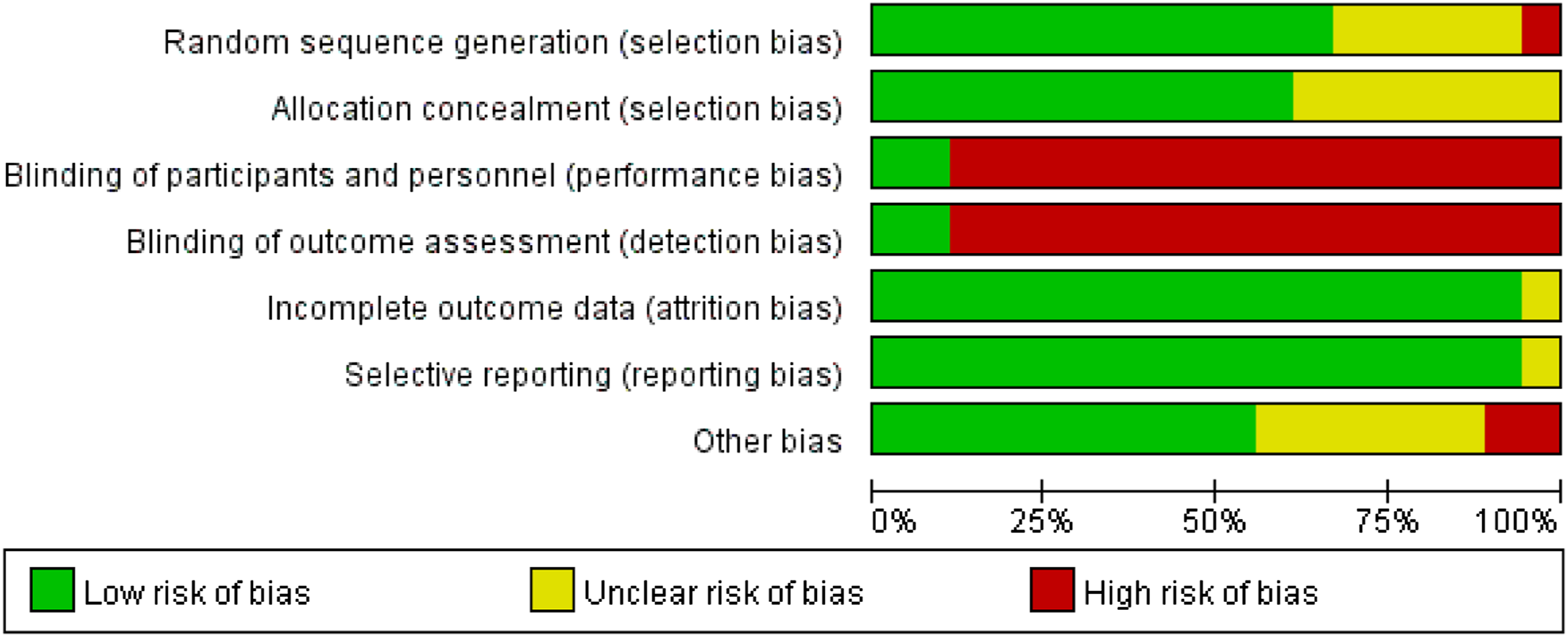
Meta-Analysis of Outcomes
Postoperative Pain at 24 Hours
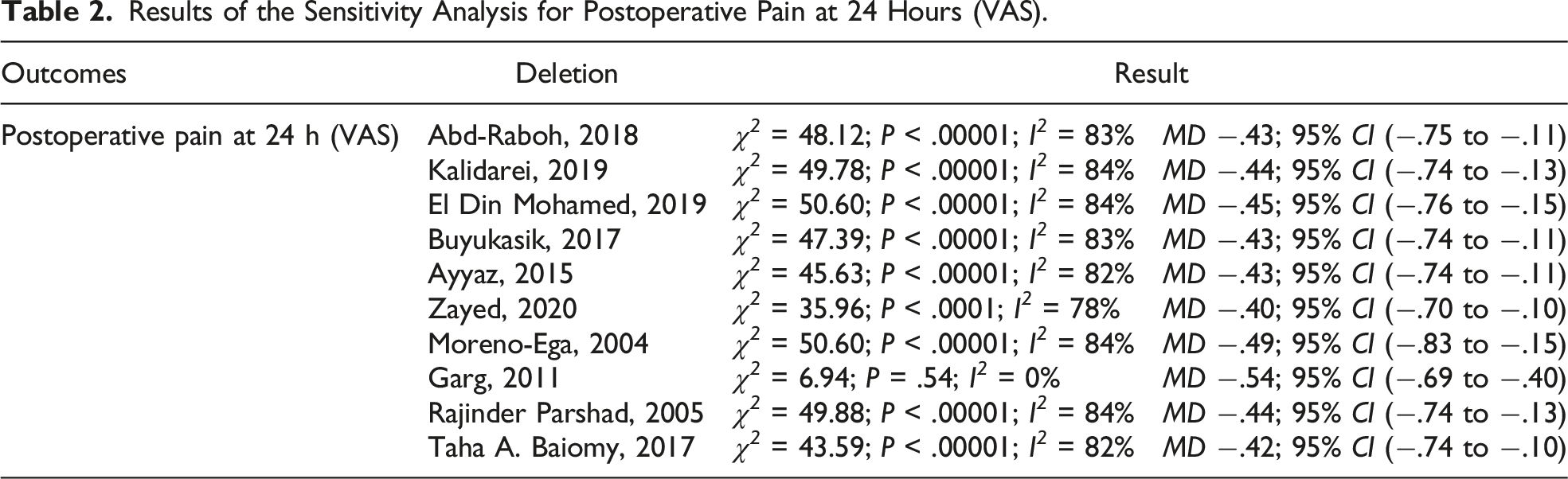
Data regarding postoperative pain at 24 hours were recorded in 10 trials. Analysis revealed that the nonfixation group had lower pain scores at 24 hours than the fixation group (mean difference [MD] −.45; 95% CI −.74 to −.15; I2 = 82%; P = .003; Figure 4). The level of between-study heterogeneity was high, and sensitivity analysis (Table 2) corroborated the robustness of consequences. Postoperative pain at 24 hours. Results of the Sensitivity Analysis for Postoperative Pain at 24 Hours (VAS).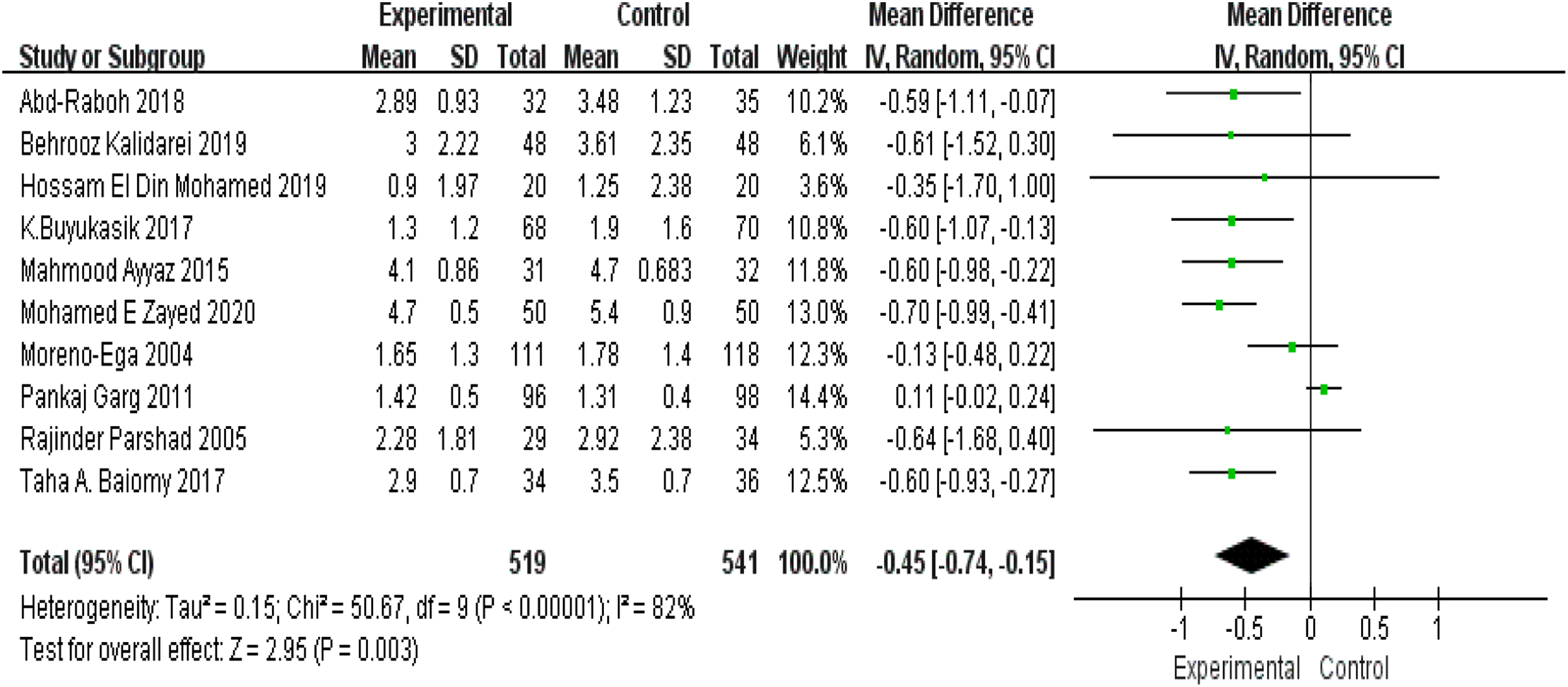
Recurrence Rate
A total of 13 studies provided data on recurrence. Analysis indicated that the difference in the rate of recurrence between the 2 groups was nonsignificant (risk ratio [RR] 1.68; 95% CI 0.75-3.76; I2 = 0%; P = .20; Figure 5). Rate of hernia recurrence.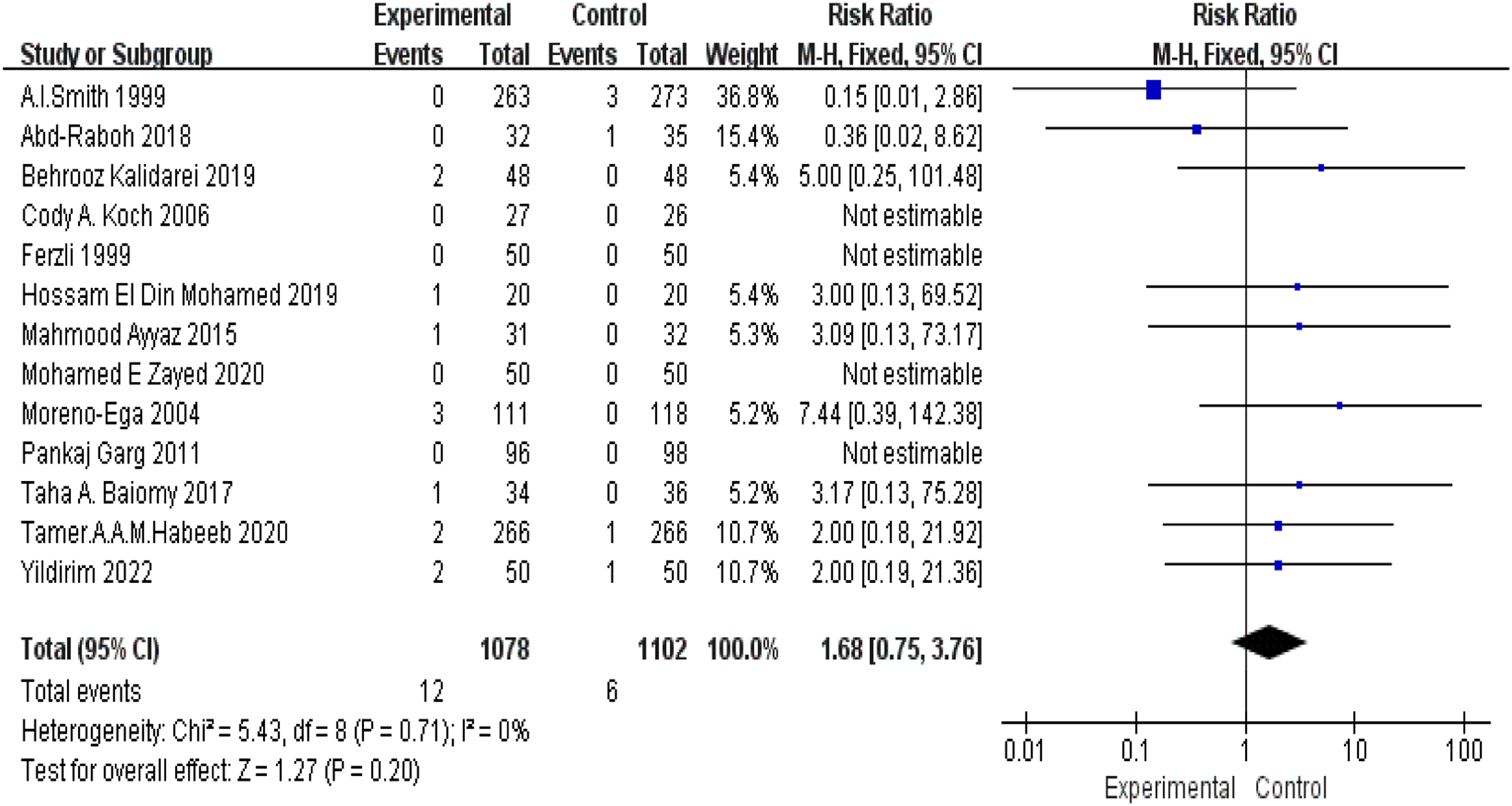
Mean Operative Time
A total of 10 articles, including 924 hernias, reported the mean operative time. Pooled statistics showed that the nonfixation method was associated with less procedural time compared to the fixation method (MD −3.53; 95% CI −5.97 to −1.10; I2 = 89%; P = .004; Figure 6). Mean operative time.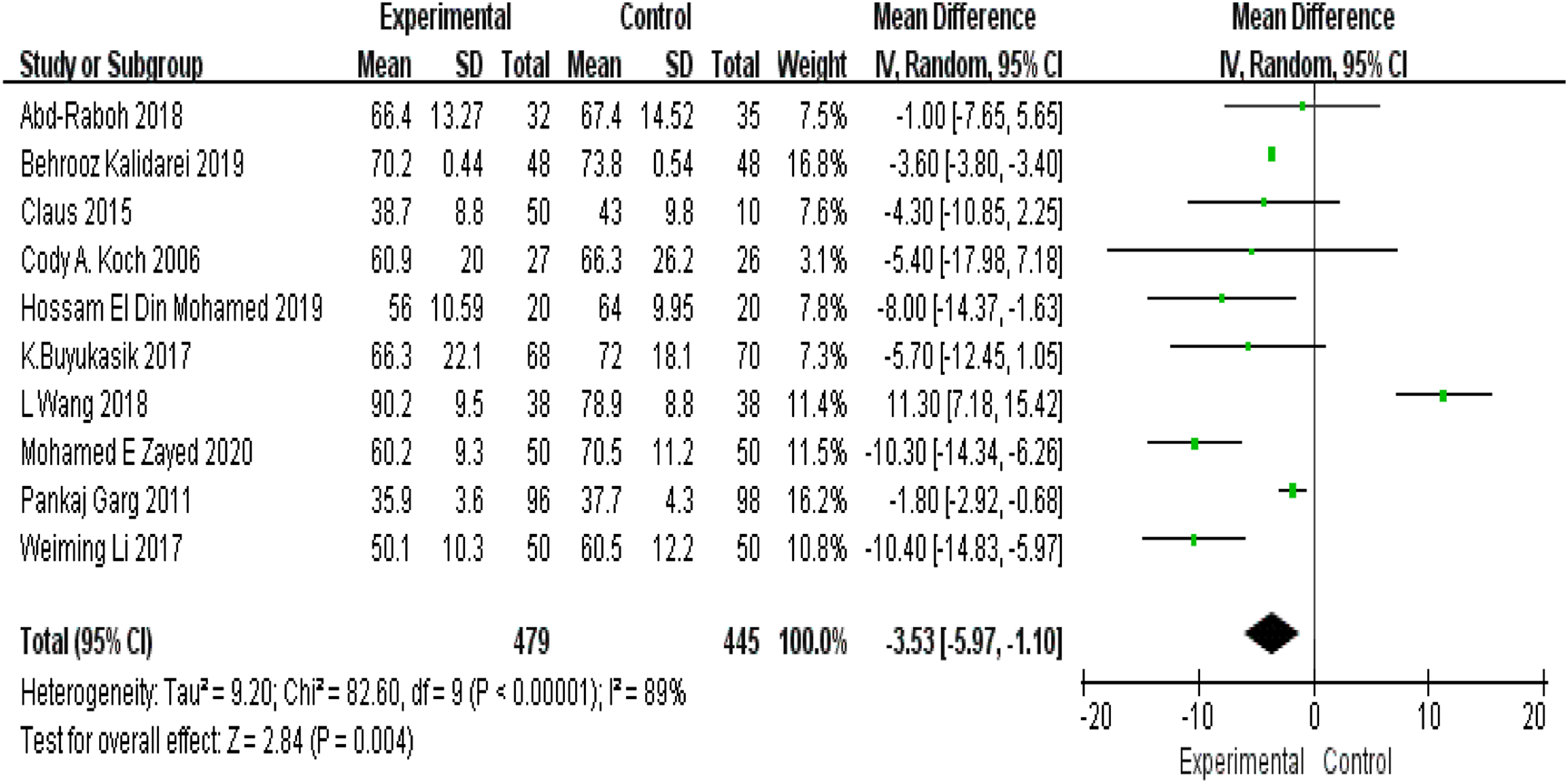
Urinary Retention
A total of 58 urinary retentions were recorded in 5 reports, comprising 387 patients. There was a low level of heterogeneity among the studies, and the synthesized statistics indicated that the fixation group had higher urinary retention rates than the nonfixation group (RR .38; 95%CI .23-.63; I2 = 0%; P = .0002; Figure 7). Urinary retention.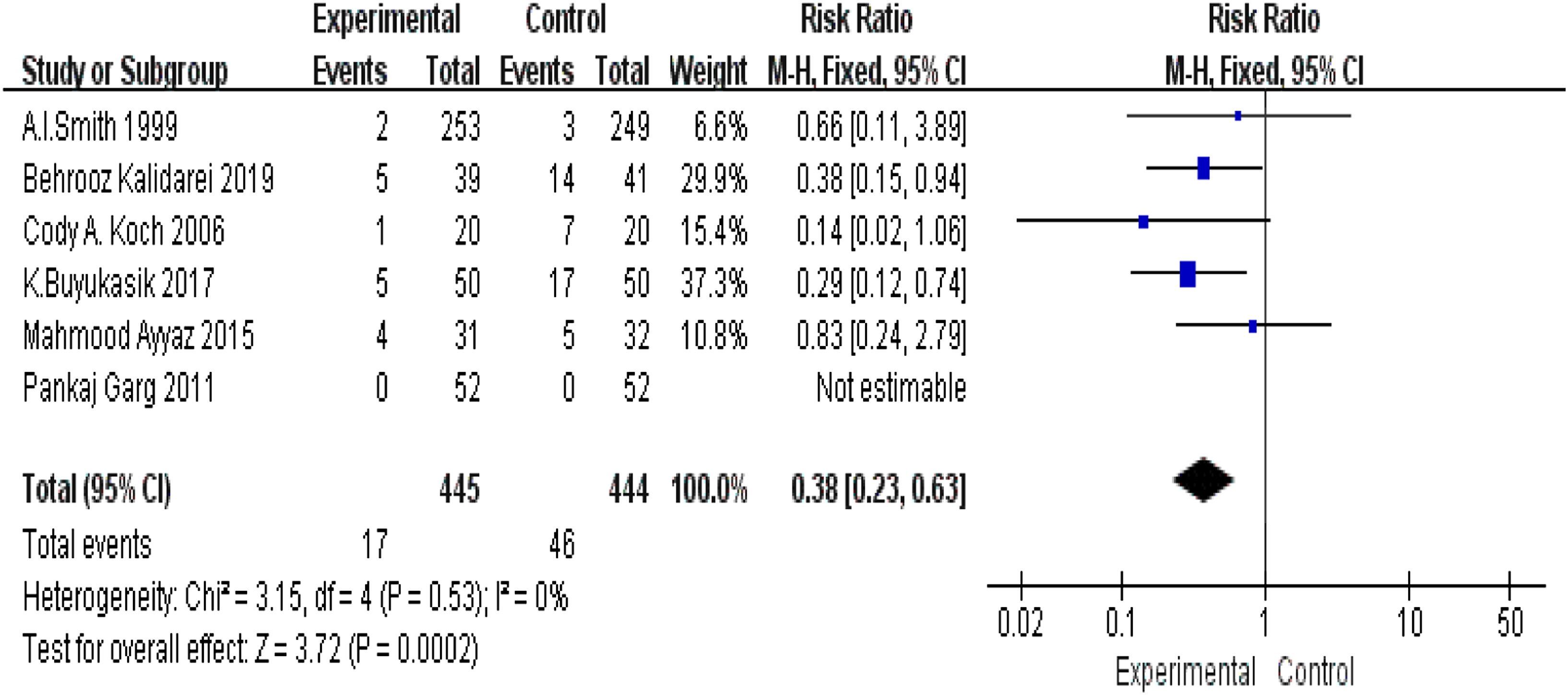
Postoperative Pain at 6 Months
Postoperative pain at 6 months was reported in 4 studies containing 434 hernias. There was no significant heterogeneity among the studies, and the fixed-effects model was used. Meta-analysis demonstrated that patients in the nonfixation group were less likely to experience pain at 6 months postoperatively compared to patients in the fixation group (MD −.21; 95% CI −.27 to −.15; I2 = 0%; P < .00001; Figure 8). Postoperative pain at 6 months (VAS).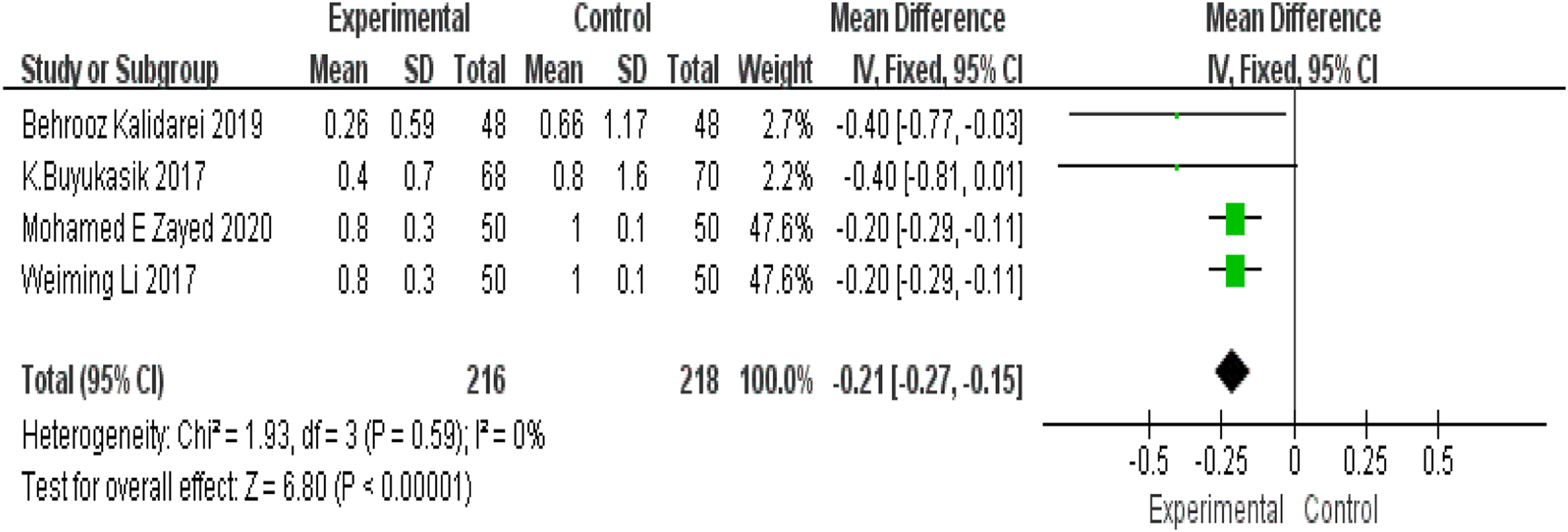
Publication Bias
For the analysis of postoperative pain at 24 hours, a funnel plot was constructed to visually assess publication bias (Figure 9), and the Egger test was performed to quantify the bias. The results (P < .05) showed that there might be publication bias. Therefore, the trim-and-fill method was used to further analyze and revise the results (Figure 9). Funnel plot for postoperative pain at 24 hours (visual analog scale). WMD, weighted mean difference.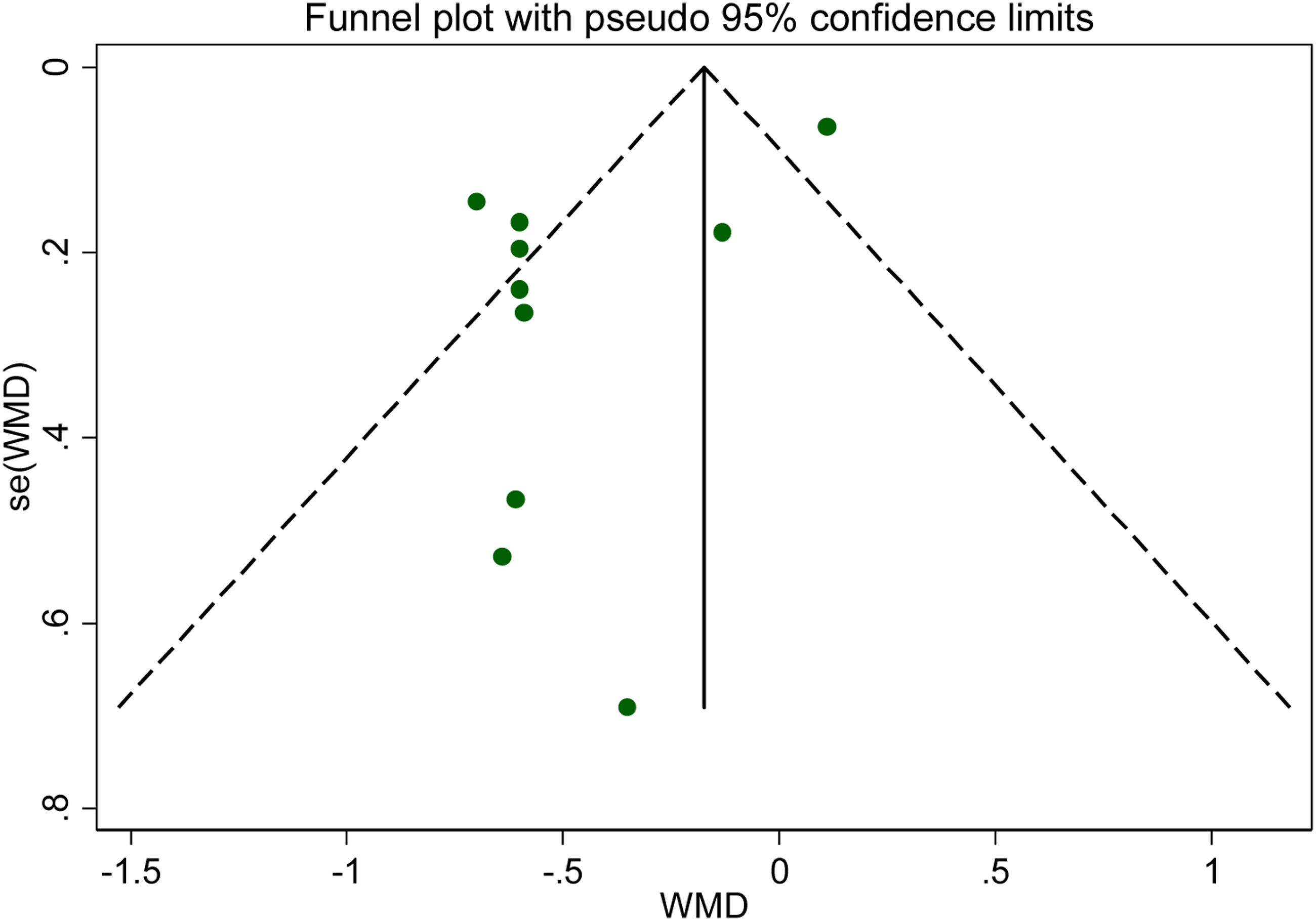
Discussion
Principal Findings
This comprehensive and systematic meta-analysis reviewed 18 RCTs published from 1999 to 2022 that evaluated the fixation and nonfixation of mesh in laparoscopic inguinal hernia repair. Our statistical results indicated that the nonfixation technique provides the 4 following advantages over the fixation method: lower postoperative pain scores at 24 hours, shorter mean operative time, less urinary retention, and lower postoperative pain scores at 6 months. Nonetheless, there was no statistical difference in recurrence between the 2 techniques.
Comparison With Previous Studies
Other studies comparing the fixation method with the nonfixation method have been conducted.3,19–23 Eltair et al, 19 Sahebally et al, 20 and Lo et al 23 all reported lower postoperative pain scores at 24 hours or 1 day in the nonfixation cohort, which is consistent with our findings (MD −.45; 95% CI −.74 to −.15; P = .003; I2 = 82%; Figure 4). However, Tam et al 21 and Teng et al 22 concluded that both techniques had similar scores for the aforementioned outcomes. In their research, Tam et al 21 included 4 participants and Teng et al 22 included 3 participants to assess postoperative pain at 1 day. Sajid et al 3 also concluded that both groups had comparable scores of postoperative pains yet did not mention a specific time point. Although chronic pain after the hernia repair surgery is a major concern among all surgeons and researchers, its definition varies across the literature. The studies by Sajid et al 3 and Lo et al 23 did not provide a definition of chronic pain. According to the International Association for the Study of Pain, 24 the most common definition of chronic pain is pain lasting beyond the normal tissue healing time, which is assumed to be 3 months. However, there are numerous articles recording pain beyond 6 months postoperatively. 25 Therefore, we chose to analyze the precise time point of 6 months postoperatively, which has not been previously examined in a meta-analysis. The results suggested that the nonfixation technique was more favorable, with little heterogeneity among studies, and was associated with less operative time compared to the fixation method, aligning with the results of Eltair et al, 19 Tam et al, 21 Teng et al, 22 and Lo et al. 23 All previously published meta-analyses mentioned above arrived at the same conclusion: the rate of recurrence is comparable between the fixation technique and the nonfixation technique. Our synthesized data of recurrence comprising both kinds of procedures (TEP and TAPP), with the most comprehensive and updated information, added more statistical weight (from a minimum of 300 participants) to strengthen the results. The findings herein regarding urinary retention included, by far, the greatest number of cases and the most recent data. We found that urinary retention occurred more often in patients with fixation than nonfixation patients. This was in contrast to the findings of Sahebally et al 20 and Tam et al 21 but concurred with the report of Lo et al 23 (4 cases).
Clinical Implications
Laparoscopic hernia repair has become increasingly popular worldwide in recent years. In our institution, approximately 80% of hernias are repaired under laparoscopy. For hernia repair, together with other functional operations, patient satisfaction and quality of life are ultimate parameters to define success. From our clinical experience, postoperative pain and urinary retention are the most common ailments besetting patients. Although the cause of postoperative pain is still under investigation, 26 our research indicated that the nonfixation technique is associated with less postoperative pain at 24 hours and at 6 months. Amid et al found that neural damage or trap by fixation of any kind could lead to postoperative pain. 27 While the nonfixation technique is an ideal way to avoid harm to the nerves, mesh fixation is a good method to reduce mesh slippage and therefore decrease the incidence of recurrence. 28 An in vitro study, sponsored by a company, verified the mesh displacement hypothesis 28 ; on the contrary, several in vivo trials8,17 have refuted it. Nonetheless, all agree that a mesh of appropriate size to obtain sufficient periorifice overlap is of vital significance. This is in line with our results showing that both techniques have a comparable rate of recurrence. All our included participants with hernia orifices less than 4 cm in size were given meshes with a diameter of more than 10 cm, and the nonfixation procedure may benefit these patients most.
Another complication of hernia repair is urinary retention, with an incidence of 2%-30% after laparoscopic groin hernia repair 29 compared to an incidence of .4%-3% in patients with open procedures. 30 Several studies have reported that age ≥60 years, history of benign prostatic hyperplasia, anesthesia ≥2 hours, and decreased BMI are risk factors for urinary retention.28,31 Our findings lend support to the nonfixation technique during operations, under the assumption that omitting fixation reduces the mean operative time and anesthesia period, thus, leading to less urinary retention compared to the fixation technique. However, the etiology of urinary retention warrants further research.
Limitations
There are some limitations to this study. First, there was a limited number of participants with data related to postoperative pain at 6 months and urinary retention, and this might have influenced the synthesized results. Further research with a larger cohort is warranted. Second, most of our included trials did not provide the weight of the mesh. Some reports have indicated that light weight mesh can reduce the incidence of chronic pain. 32 Thus, more studies concerning mesh weight and chronic pain are needed. Third, the performance and detection bias were high in most of our eligible studies due to the dissatisfactory blinding, which is quite challenging for clinical interventions such as operations. Fourth, as we only included patients with hernia orifices <4 cm in size, it is unclear whether our results are applicable for inguinal hernias bigger than 4 cm, and thus further investigation is required.
Conclusions
The nonfixation technique is superior to the fixation method during laparoscopic hernia repair in terms of postoperative pain at 24 hours and at 6 months, mean operative time, and urinary retention. Interestingly, the 2 procedures were comparable with regard to the rate of recurrence in patients with inguinal hernia orifices less than 4 cm in size.
Footnotes
Author Contributions
Yuxing Lv and Yinquan Wang developed, conducted, and reported the main data/outcomes. Bo Yang and Gaopeng Hao supported writing the discussion section. All authors have made substantial contributions to the final manuscript. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Shanxi Province 136 Revitalization Medical Project Construction Funds.