
Abstract
Introduction
The identification and treatment of traumatic pneumothorax (PTX) has long been a focus of bedside imaging in the trauma patient. While the emergence of bedside ultrasound (BUS) provides an opportunity for earlier detection, the need for tube thoracostomy (TT) based on bedside imaging, including BUS and supine AP chest X-ray (CXR) is less established in the medical literature.
Methods
Retrospective data from 2017 to 2020 were collected of all adult trauma activations at a level 1 rural trauma facility. Every adult patient included in this study received a CXR and BUS (eFast) upon arrival. The need for TT was determined by the emergency medicine attending or the trauma surgery attending evaluating the patient. McNemar’s chi-squared test and conditional logistic regression analysis were performed comparing BUS, CXR, and the combination of BUS and CXR findings for the need for TT. Subgroup analyses were performed comparing BUS, CXR, and the combination of BUS and CXR for the detection of PTX compared to CT scan.
Results
Of the 12,244 patients who underwent trauma activation during this timeframe, 602 were included in the study. 74.9% were males with an age range of 36-63 years. Of the 602 patients, 210 received TT. Positive PTX was recorded with BUS in 128 (21%) patients with 16 false negatives (FNs) and 98 false positives (FPs), 100 (17%) PTX were identified with CXR with 114 FNs and 4 FPs, and 72 (11.9%) were noted on both CXR and BUS with 140 FNs and 2 FPs. The odds ratio of TT placement was 22 times with positive BUS alone (P < .0001, 95% CI: 10.9-43.47), 47 times with positive CXR alone (P < .0001, 95% CI: 16.99-127.5), and 70 times with both positive CXR and BUS (P < .0001, 95% CI: 17.08-288.4).
Conclusion
A positive finding of PTX on BUS combined with CXR is more indicative of the need for TT in the trauma patient when compared with BUS or CXR alone.
Keywords
Introduction
Traumatic thoracic injury is a common cause of morbidity and mortality seen in the acute care setting. It is estimated that 20%-25% of all deaths related to traumatic injury are secondary to chest trauma and 15%-50% of chest traumas result in traumatic pneumothorax (PTX).1,2 The PTX is a common, serious injury that occurs when there is disruption between the parietal and visceral pleura of the lungs, causing air to collect in the pleural space. 3 A small PTX is considered to occupy less than 15% of the pleural cavity, moderate is between 15% and 60%, and large is greater than 60%. 2
The identification of and treatment for pneumothoraces has become a topic of focus as bedside ultrasound (BUS) has enabled earlier, and increased, detection. A recent meta-analysis using data from 13 studies to compare the accuracy of chest ultrasound vs supine chest X-ray (CXR) found a significantly higher detection rate of PTX with chest ultrasound. In this analysis, the sensitivity and specificity of chest ultrasound performed in the emergency department (ED) were 91% and 99%, respectively. CXR in the same setting provided a sensitivity and specificity of 47% and 100%, respectively. 4 Studies have consistently shown higher sensitivity with BUS than with CXR. While this leads to an increase in PTX detection, the clinical significance of these PTX remains subject to debate.
The 2 main factors in determining the management of traumatic PTX are a patient’s clinical status and the size of the PTX. The current standard of care for clinically significant PTX is tube thoracostomy (TT), because clinical deterioration occurs as PTX size increases, ultimately leading to tension PTX and cardiopulmonary collapse. Positive pressure ventilation, such as occurs with intubation, continuous positive pressure ventilation, or air transport may expedite this process. 3 Occult PTX refers to a PTX that is not suspected clinically or detected with CXR. 5 Traditionally, these were only detected with computed tomography (CT) imaging but now are also being discovered with ultrasound.2,5
There is no debate that patients with deteriorating clinical status (ie, hypoxia, hypotension, or severe dyspnea) with PTX seen with any imaging modality require TT. However, asymptomatic patients or patients with occult pneumothoraces may not always benefit from invasive intervention. This study examined how bedside imaging correlated with the need for tube thoracostomy in the trauma patient. The authors hypothesized that the combination of a positive BUS and CXR for PTX would be the most predictive of TT placement.
Methods
We performed a retrospective study from a single American College of Surgeons–verified level 1 trauma facility. With approval from the Institutional Review Board, the trauma registry was queried for all adult patients who were assigned trauma team activation status between 2017 and 2020. Patients were excluded for the following: penetrating trauma, TT placement prior to supine CXR and BUS, age less than 18 years, needle decompression performed prior to ED arrival, or a traumatic arrest prior to arrival. The electronic health record was reviewed for relevant diagnoses, procedural details and interventions, and imaging reports including BUS, CXR, and CT scans.
During each trauma activation, BUS, commonly referred to as eFAST, was performed by an emergency medicine or surgical resident, attending emergency medicine physician, or attending trauma surgeon. All resident BUS are reviewed by emergency medicine or trauma attendings. The BUS was performed using a 5.0 MHz curvilinear-array transducer on a GE or Sonosite ultrasound machine. The BUS evaluation uses 6 standard views including anterior views of each hemithorax while in the supine position. Ultrasonographers viewed the lung windows to evaluate for lung slide. All imaging was evaluated in real time by the ultrasonographer performing the exam.
Additional data collected included age, sex, location of TT placement, and time of TT placement. Location of TT placement included right, left, or bilateral. Time of TT placement was categorized as before CT scan, after CT scan, on admission, or delayed (8-72 hours post-admission). Patients with TT placement more than 72 hours post-admission were excluded. Placement of TT was directed by the attending trauma surgeon based on the size of the PTX, need for drainage of concomitant hemothorax, and patients vital signs.
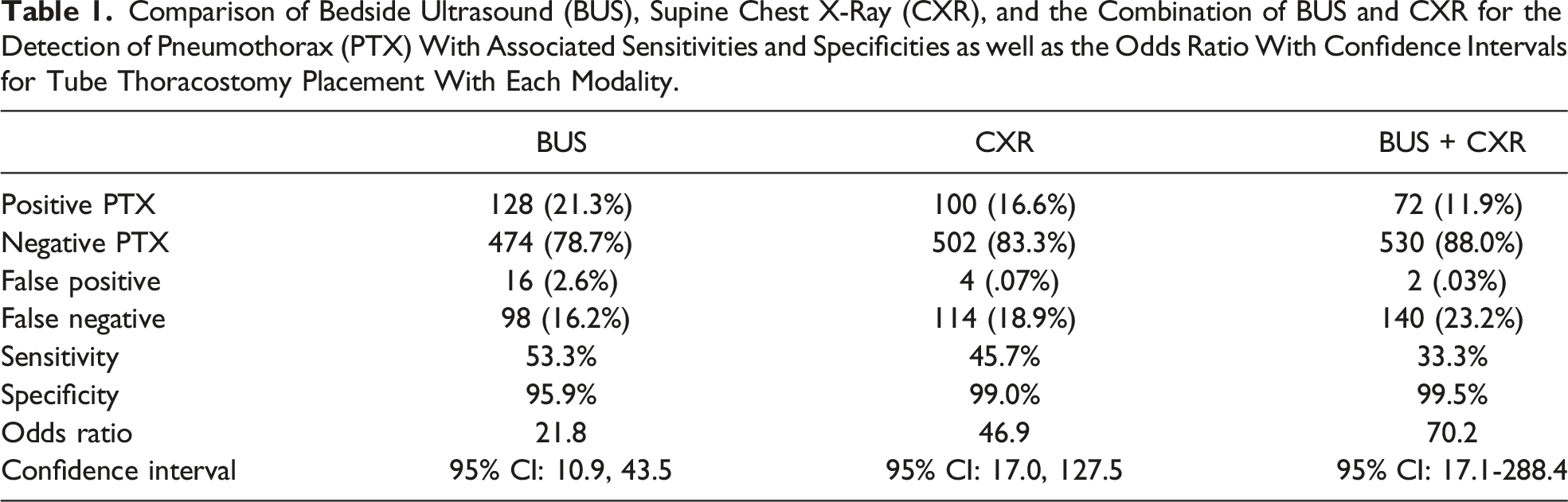
Comparison of Bedside Ultrasound (BUS), Supine Chest X-Ray (CXR), and the Combination of BUS and CXR for the Detection of Pneumothorax (PTX) With Associated Sensitivities and Specificities as well as the Odds Ratio With Confidence Intervals for Tube Thoracostomy Placement With Each Modality.
Results
A total of 12,244 patients underwent trauma activation during the timeframe of the study. Of these patients, 602 were included in the study and received both a CXR and BUS (Figure 1). The study population was 74.9% male, with a mean age of 52 years and a range of 36-63 years. Study design and distribution of patients for tube thoracostomy with associated imaging modalities. Abbreviations: (BUS) bedside ultrasound; (CXR) chest X-ray; (CT) computed tomography.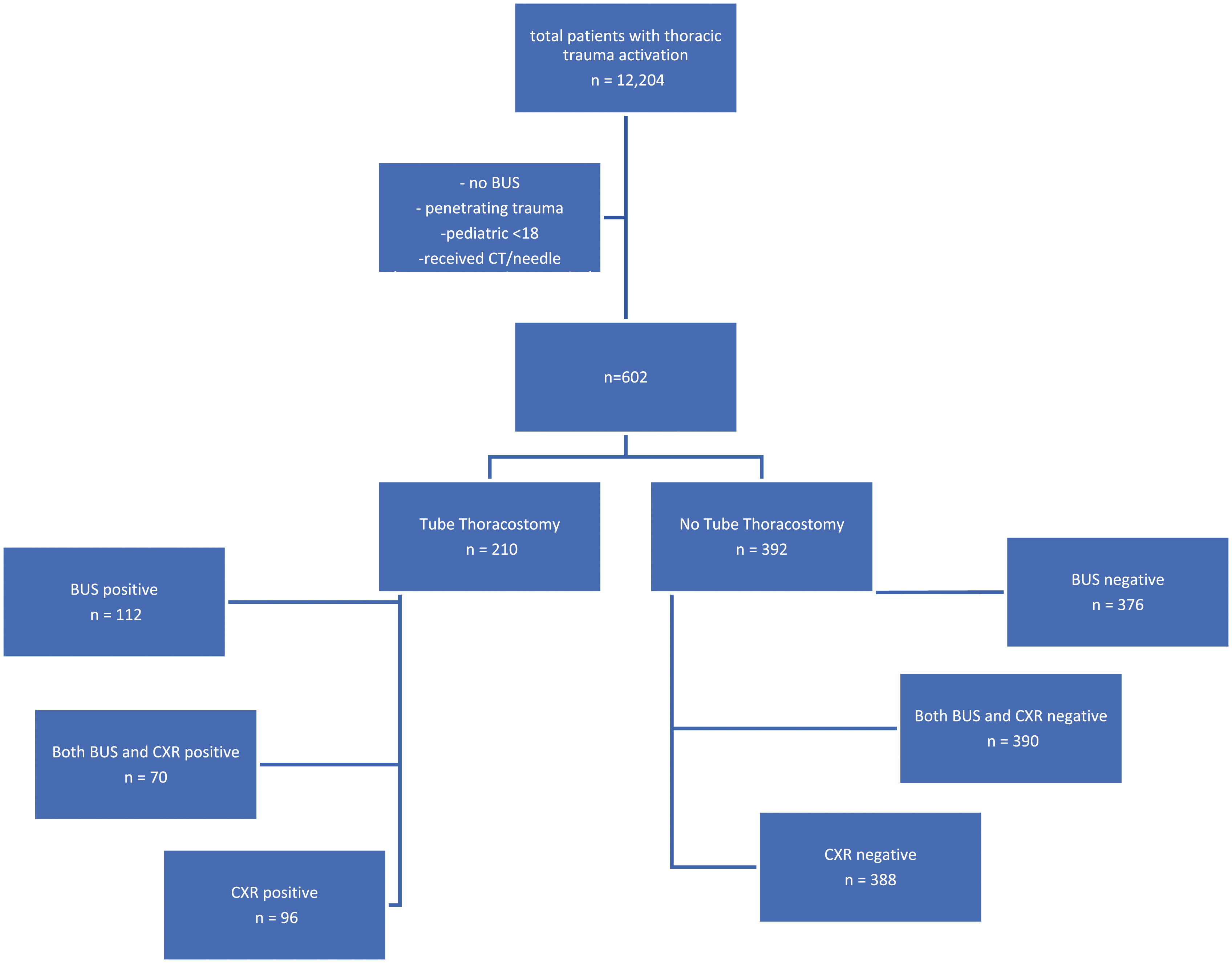
A positive finding of PTX was recorded with BUS in 128 (21%) patients and negative findings were recorded in 474 (79%) patients. There were 16 patients who had a negative BUS exam for PTX and still received a TT, whereas 98 patients with a positive finding for PTX on BUS did not receive a TT. This indicates that the sensitivity and specificity of BUS evaluation for determining the need for TT placement were 53.3% and 95.9%, respectively. Conditional logistic regression analysis showed a statistically significant relationship between positive PTX on BUS and TT placement (P < .0001). In particular, the odds of TT placement with positive BUS were 22 times those of TT placement with negative BUS (95% CI: 10.9-43.47).
With CXR, a positive finding of PTX was recorded in 100 (17%) patients and a negative finding was recorded in 502 (83%) patients. There were 4 patients who had a positive CXR for PTX without TT placement and 114 with a negative CXR who received TT placement. The sensitivity of positive CXR associated with TT placement was 45.7% and specificity was 99.0%. Logistic regression analysis showed a statistically significant relationship between positive CXR for PTX and TT placement (P < .0001). The odds of TT placement after positive CXR for PTX were 47 times those of TT placement with a negative CXR for PTX (95% CI: 16.99-127.5).
Finally, we combined the data to evaluate patients with positive findings for PTX on both CXR and BUS with TT placement. There were 72 (11.9%) patients with positive findings for PTX on both BUS and CXR, including 2 patients who did not receive TT placement despite the double-positive findings. There were 530 (88%) patients without positive findings on both BUS and CXR, of which 140 received TT placement. The sensitivity of positive findings on both BUS and CXR for determining the need for TT placement was 33.3%, with a specificity of 99.5%. The results of logistical regression analysis showed a statistically significant relationship between TT placement and positive findings of PTX on both BUS and CXR (P < .0001). The odds of TT placement with positive findings for PTX on both BUS and CXR were 70 times those of TT placement without a positive finding for PTX on both BUS and CXR (95% CI: 17.1, 288.4) (Table 1).
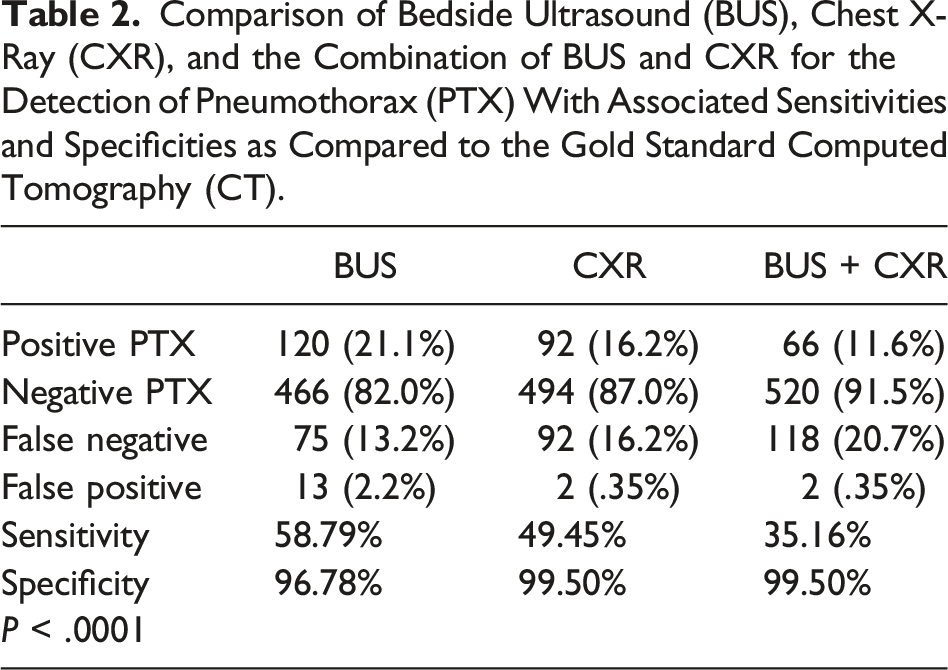
Comparison of Bedside Ultrasound (BUS), Chest X-Ray (CXR), and the Combination of BUS and CXR for the Detection of Pneumothorax (PTX) With Associated Sensitivities and Specificities as Compared to the Gold Standard Computed Tomography (CT).
Discussion
Many studies have compared the accuracy of BUS to that of CXR for detection of PTX. Additional data is needed to compare the detection of PTX by BUS, CXR, or both combined, and to assess the impact of these findings on clinical interventions such as TT. Our study compares the utility of BUS alone with that of CXR alone and CXR and BUS combined in determining a clinical need for TT. We demonstrated that a positive finding for PTX on BUS and CXR combined was associated with a higher likelihood for the placement of TT compared with a positive result on either BUS or CXR alone. Although the data showed a higher sensitivity for TT placement with a positive BUS, the odds of TT placement were much lower than when PTX was identified on CXR or when CXR and BUS were both positive for PTX. These data indicate that using BUS in conjunction with CXR can aid the physician at the bedside in determining who will require TT and furthermore, demonstrates that a supine CXR remains a significant component of the trauma patient evaluation.
In our study, there were 98 (16.2%) recorded positive findings for PTX with BUS alone that did not receive a TT, compared with only 4 (<1%) positive findings with CXR alone that did not receive a TT. These data support the hypothesis that BUS detects occult pneumothoraces that would otherwise only be found with CT scan. A similar systematic review of 4 prospective observational studies involving 606 patients with blunt thoracic trauma compared the accuracy of chest ultrasound vs CXR for detecting PTX. 6 That study found a significantly higher PTX detection rate with chest ultrasound than with CXR. The results showed that the sensitivity and specificity of chest ultrasound performed in the ED ranged from 86% to 98% and 97% to 100%, respectively. CXR in the same setting revealed a sensitivity range of 28%–75% and a specificity of 100%. Studies have consistently shown greater accuracy of PTX detection with BUS as compared with CXR, but our study suggests that earlier detection may not demonstrate a need for intervention.
Several studies have shown that TT for traumatic pneumothoraces is associated with numerous complications and is unnecessary in many circumstances.7–11 For the management of traumatic occult PTX, evidence from a systematic review comparing 3 randomized controlled trials showed no significant differences in the progression of PTX, hospital length of stay, or mortality between the TT and observation groups. 12 That review concluded that observation of occult PTX was at least as safe and effective for management as TT placement. One concern is that the introduction of positive pressure ventilation, whether through positive pressure mask ventilation, laryngeal mechanical assistive device, or intubation will cause a PTX to progress, leading to higher morbidity and mortality. A 2013 randomized controlled trial involving 95 ventilated patients showed that although 20% of the observation group eventually required a TT secondary to progression, the risks of respiratory compromise and mortality were the same in both groups. 13
Ultimately, the most significant factors in determining the need for TT in traumatic PTX appear to be size of the PTX and clinical status. One large retrospective study suggested that patients with traumatic PTX less than 35 mm (distance on CT between pleura and mediastinum) had a 9% observation failure rate, requiring TT, as compared with a 41% failure rate for those with PTX greater than 35 mm. 14 While independent physicians may intervene for PTX of different sizes, there is a correlation between PTX size and clinical status. Patients presenting with hypoxia, hypotension, and severe dyspnea with positive PTX findings on BUS, CXR, or CT require intervention with TT.
Recently, a study by Santorelli et al (2022) 15 suggested that chest ultrasonography may not offer an advantage at diagnosing pneumothorax over CXR. This large, retrospective, single-center study included 362 patients with CT-confirmed PTX after chest trauma who received a diagnostic CXR and complete ultrasonography of trauma (CUST) assessment upon initial evaluation. The CUST examinations include the standard BUS views plus 4 thoracic views, including 2 anterior and 2 lateral views in each hemithorax. Results of this study showed an initial sensitivity of 43% for CXR and 35% for CUST for detection of PTX. When occult PTX, defined as PTX seen only on CT, was excluded from the results, the sensitivity of CXR was 78% and that of CUST was 65%. There was a false-negative rate of 36% in the CUST group. This study’s findings suggest that CUST may not provide an advantage over CXR in determining clinically significant PTX.
Limitations
This study has the usual limitations of a retrospective study. To minimize the effect of incomplete registry data, charts were reviewed for accuracy. The study included patients with delayed TT placed >8 hours from time of presentation, which may have been unrelated to the initial BUS and CXR taken while in the ED. Also, the decision to place a TT while in the ED often occurred before the official radiology evaluation of CXR or BUS, based on a preliminary evaluation by the trauma surgeon or emergency physician. Another important limitation is that the need for TT was not defined by any objective measures recorded in our study. We assumed that patients who received TT needed them based on expert opinion, with clinical status, patient stability, size of PTX seen with CXR or CT scan, and comfort of the attending provider likely all playing a role. To our knowledge, however, this is an accepted practice and may be an area for future research.
Conclusion
Historically, BUS and CXR have been essential components of the bedside imaging of the trauma patient. Our study continues to support the use of both BUS and CXR in the workup of these patients and demonstrates that each plays a vital role in the workup of the trauma patient. Our study further shows that BUS and CXR are best utilized in conjunction rather than independently when predicting which patient will require TT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research reported in this publication was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 5U54GM104942-04. Grant funding provided protected research time for James Bardes.