
Abstract
Background
The aim of this systematic review and meta-analysis is to evaluate clinical, functional, and anorectal physiology outcomes of the side-to-end vs colonic J-pouch (CJP) anastomosis following anterior resection for rectal cancer.
Methods
A PRISMA-compliant systematic review and meta-analysis was conducted using multiple electronic databases and clinical trial registers and all studies comparing side-to-end vs CJP anastomosis were included. Peri-operative complications, mortality rate, functional bowel, and anorectal outcomes were evaluated.
Results
Eight randomized controlled trials (RCTs) and two observational studies with 1125 patients (side-to-end: n = 557; CJP: n = 568) were included. Of the entire functional bowel outcome parameters analyzed, only the sensation of incomplete bowel evacuation was significant in the CJP group at 6 months [OR: 2.07; 95% CI 1.06 - 4.02, P = .03]. Peri- and post-operative clinical parameters were comparable in both groups (total operative time, intra-operative blood loss, anastomotic leak rate, return to theater, anastomotic stricture formation and mortality). Equally, most of the analyzed anorectal physiology parameters (anorectal volume, anal squeeze pressure, maximum anal volume) were not significantly different between the two groups. However, anal resting pressure (mmHg) 2 years post-operatively was noted to be significantly higher in the side-to-end group than that of the CJP configuration [MD: −8.76; 95% CI - 15.91 - 1.61, P = .02].
Discussion
Clinical and functional outcomes following CJP surgery and side-to-end coloanal anastomosis are comparable. Neither technique appears to proffer solution to low anterior resection syndrome in the short term but future well-designed; high-quality RCTs with long term follow-up are required.
Introduction
Rectal cancer is one of the most common malignancies worldwide. Improvements in the understanding of cancer pathophysiology and surgical technologies have led to a decline in abdominoperineal resections (APR), first described by Miles. 1 Sphincter-preserving approaches, such as low anterior resection and total mesorectal excision (TME) have become increasingly desirable with emphasis on maintaining intestinal continuity, avoiding need for permanent stoma, and preserving anorectal function while maintaining acceptable oncological outcomes as compared with APR.2,3
TME is considered the “gold standard” in rectal cancer surgery. Its increased use has led to a reduction in circumferential resection margin (CRM) positivity and improved survival rates. However, sphincter-sparing procedures involving partial/total rectal excision and a straight (end-to-end) anastomosis may lead to “low anterior resection syndrome” (LARS) as excision of the recto-sigmoid colon often leads to loss of the rectal reservoir function.4,5 LARS is characterized by a collection of symptoms (incontinence, stool frequency/urgency, clustering of bowel motions) with profound adverse effects on patients’ quality of life (QoL). 6
To overcome these, Lazorthes et al 7 and Parc et al 8 independently described the construction of a colonic J-pouch (CJP), created through closing and folding of the distal colon followed by anastomosing the base of the J-pouch with the residual rectum or anal canal.
This serves as a neo-rectal reservoir and studies have demonstrated that compared with a straight anastomosis, the CJP provides better QoL scores, superior functional outcomes, and improved anorectal function.9-13
However, forming the CJP is technically more demanding and stool evacuation problems may persist post-operatively. 12 As a 5-8 cm long colonic segment is considered optimal for CJP construction, anatomical obstacles such as a narrow male pelvis or insufficient colon length means that not all patients are suitable. 14
Therefore, the side-to-end coloanal anastomosis gained attention as this usually requires a shorter colonic segment of 3-5 cm. 15 It offers a smaller reservoir compared with the CJP but retains functional advantages over a straight configuration. This modification may also offer similar functional advantages and benefits as conferred by the CJP 16 but potentially associated with less long-term evacuation difficulties.
Recent meta-analyses have suggested that the CJP and side-to-end anastomosis are comparable in terms of functional outcomes, QoL parameters, and peri-operative outcomes.5,17 We conducted an updated systematic review and meta-analysis using all available data to evaluate clinical, functional bowel, and anorectal physiology outcomes of the side-to-end vs CJP anastomosis.
Methods
This systematic review and meta-analysis was designed, performed, and reported as per the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.18,19
Data Sources and Search Strategy
An online systematic search was conducted on 01/06/2022 using PubMed, Embase, Scopus, Cochrane Database of Systematic Reviews (CENTRAL), clinical trials.gov, ScienceDirect, and the virtual health library (VHL) by two independent authors. Moreover, the same authors independently evaluated the reference lists of included studies to identify relevant articles. Keywords used in the search are outlined in Supplementary file 1.
Design and Study Selection
Two independent authors screened titles, abstracts, or full texts of the selected articles to identify potentially eligible studies. These were carefully assessed against the eligibility criteria. All single-arm studies, case series, case reports, letters to the editor, and review articles were excluded. Disagreements in this process were resolved by discussion between the authors, consulting an independent author if required.
Data Extraction and Collection
Two authors independently performed data extraction from the selected studies including: study-related data; baseline demographic and clinical information of the study populations; and primary and secondary outcome data. A pre-generated standard Microsoft ® Excel (Microsoft Corporation, Redmond, Washington, USA) file was created, pilot-tested in randomly selected articles and adjusted accordingly. Disagreements at this stage were resolved by discussion and consensus with an independent third author consulted if no agreement could be reached.
Outcome Measures
Intra- and peri-operative outcomes (total operative time, intra-operative blood loss, anastomotic leak rate, return to theater, post-operative urinary tract infection, recto-vaginal fistula formation, anastomotic stricture/stenosis occurrence, and mortality rate) were the measured primary parameters. Secondary outcome measures were stool frequency per day and stool urgency (3, 6, and 12 months), tenesmus (6 months), anal resting pressure (2 years), anal resting pressure volume (6 months), anal squeeze pressure (2 years), and maximum anorectal volume (6 months and 2 years).
Risk of Bias Assessment
The Cochrane risk of bias tool was used to appraise the risk of bias for randomized trials. 20 Two investigators independently reviewed all studies and graded the risk as “high,” “low,” or “unclear” in the following categories: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias.
The Newcastle–Ottawa Scale (NOS) was used to assess the risk of bias for observational studies. 21 Studies were considered low, medium, or high-risk if the NOS score was 9, 7/8, ≤6, respectively. Disagreement in this process was resolved through discussion and consulting a third reviewer where required.
Statistical Analysis
Odds ratio (OR) was used as the statistical measure for dichotomous outcomes using the Mantel–Haenszel method. When 25% or more of the included studies reported zero events in both comparison groups, the risk difference (RD) was reported instead of the OR. For continuous outcomes, the mean difference (MD) with 95% confidence interval (CI) was estimated. When mean values were not available for continuous outcomes, data on median and interquartile range (IQR) were extracted and subsequently converted to mean and standard deviation (SD) using the well-practised equation described by Hozo et al. 22
P < .05 was considered statistically significant for all analyses, a 95% CI was used, and random-effects modeling was applied to all outcome analysis.
Between-study heterogeneity was assessed using the I2 and χ2 statistic. High values of I2 and the χ2 statistic signify increasing levels of heterogeneity, with P < .05 or an I2 value exceeding 50% indicating significant heterogeneity. 19 To check possible causes of heterogeneity and evaluate the robustness of the results, sensitivity analysis was performed by calculating the risk ratio (RR) or RD for dichotomous variables. Moreover, leave one-out-analysis was conducted to assess the effect of each study individually. All statistical analysis was performed using Review Manager 5.0 (Nordic Cochrane Centre, Cochrane Collaboration).
Results
A total of 655 studies were identified and following review of titles/abstracts and removal of any duplicates, 525 studies were excluded. Full manuscripts of the remaining 130 were assessed, identifying 12 relevant articles23-34 that were included in our final data synthesis.
PRISMA flow chart is shown in Figure 1. PRISMA flow diagram.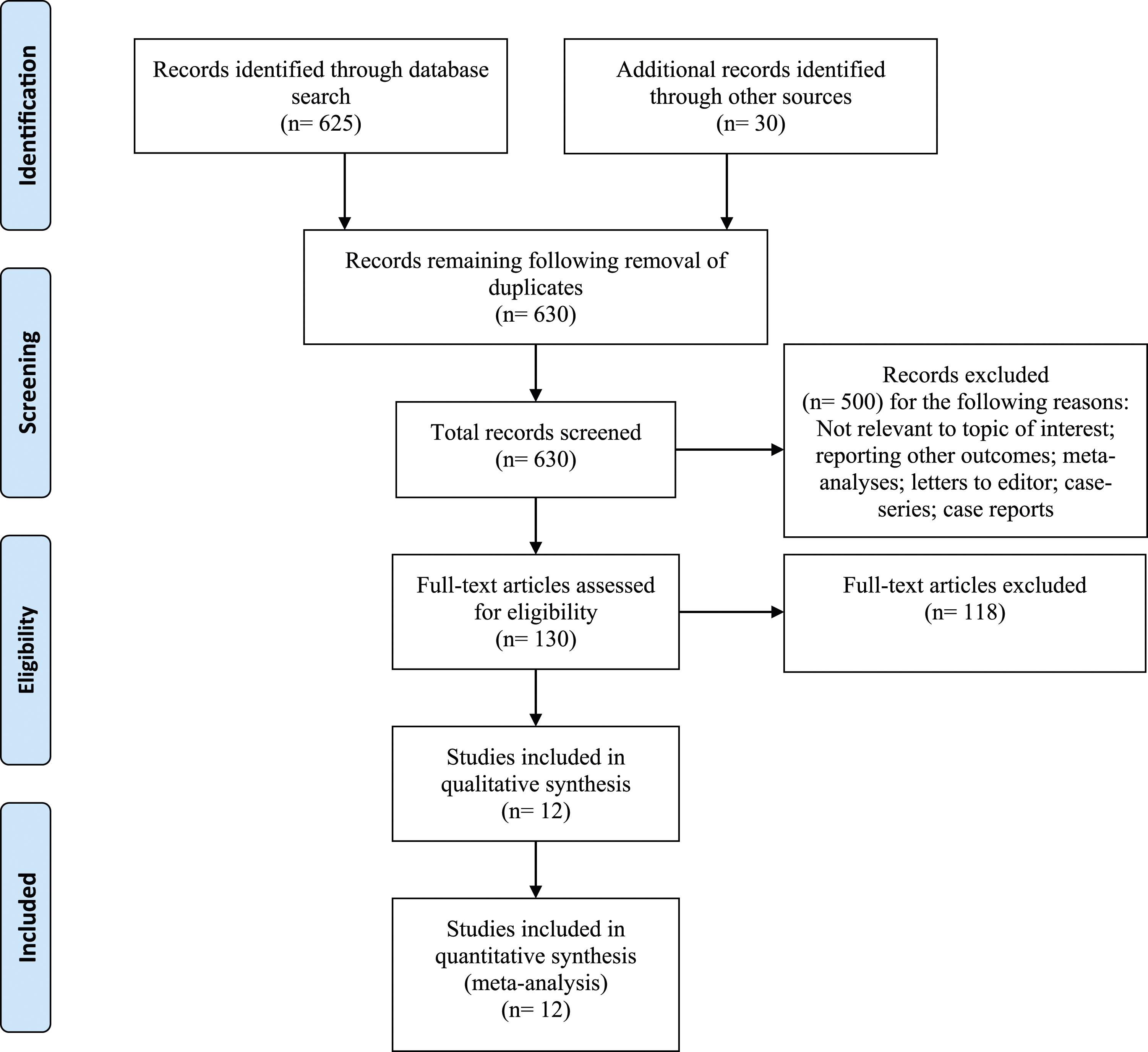
Two were cohort studies and eight randomized controlled trials (RCTs) with a total of 1125 patients divided into a side-to-end (n = 557) and CJP (n = 568) group. Two RCTs reporting different outcomes from the same cohort resulted in two separate publications.
Characteristics of the Included Studies.
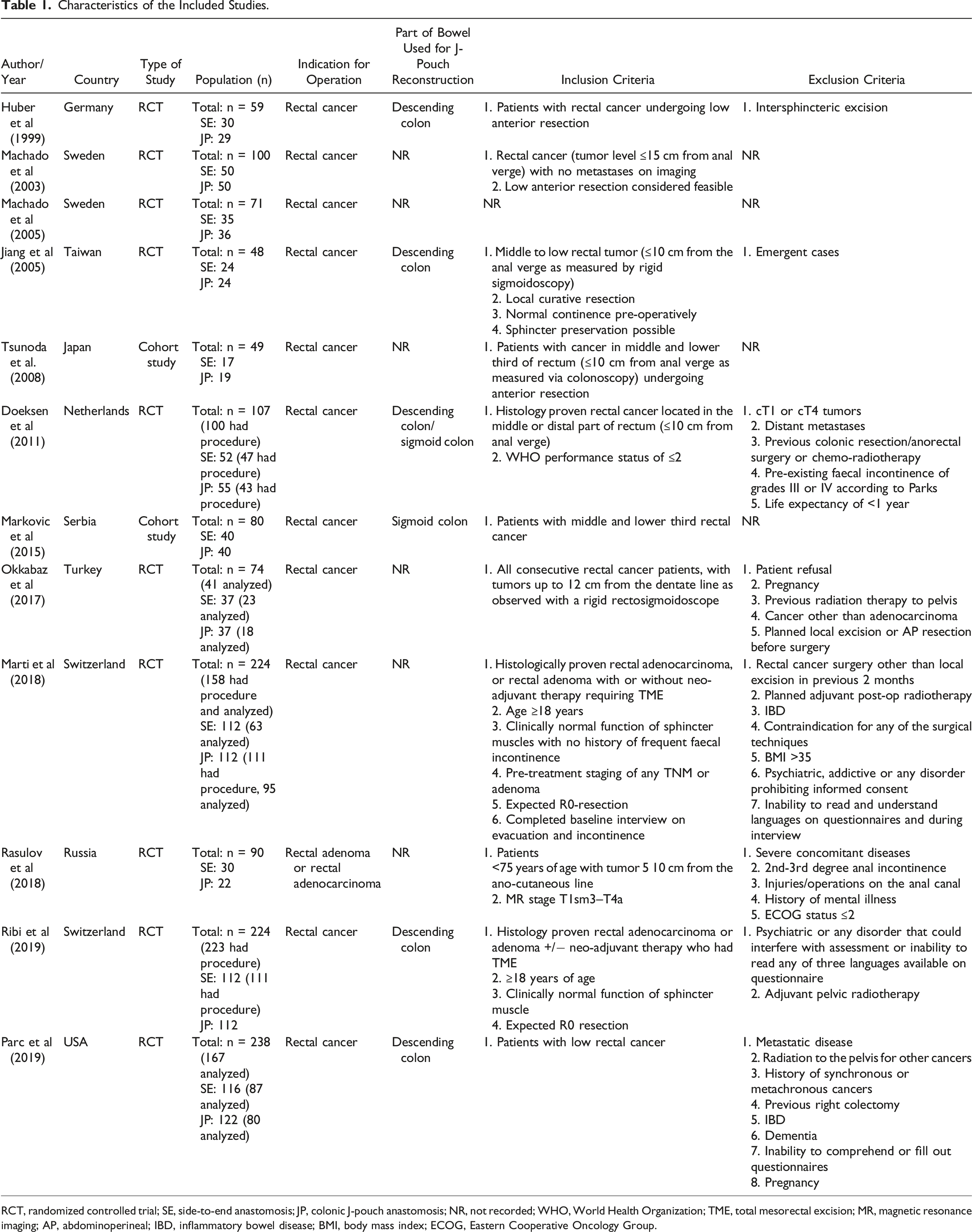
RCT, randomized controlled trial; SE, side-to-end anastomosis; JP, colonic J-pouch anastomosis; NR, not recorded; WHO, World Health Organization; TME, total mesorectal excision; MR, magnetic resonance imaging; AP, abdominoperineal; IBD, inflammatory bowel disease; BMI, body mass index; ECOG, Eastern Cooperative Oncology Group.
Baseline Characteristics of the Study Population.
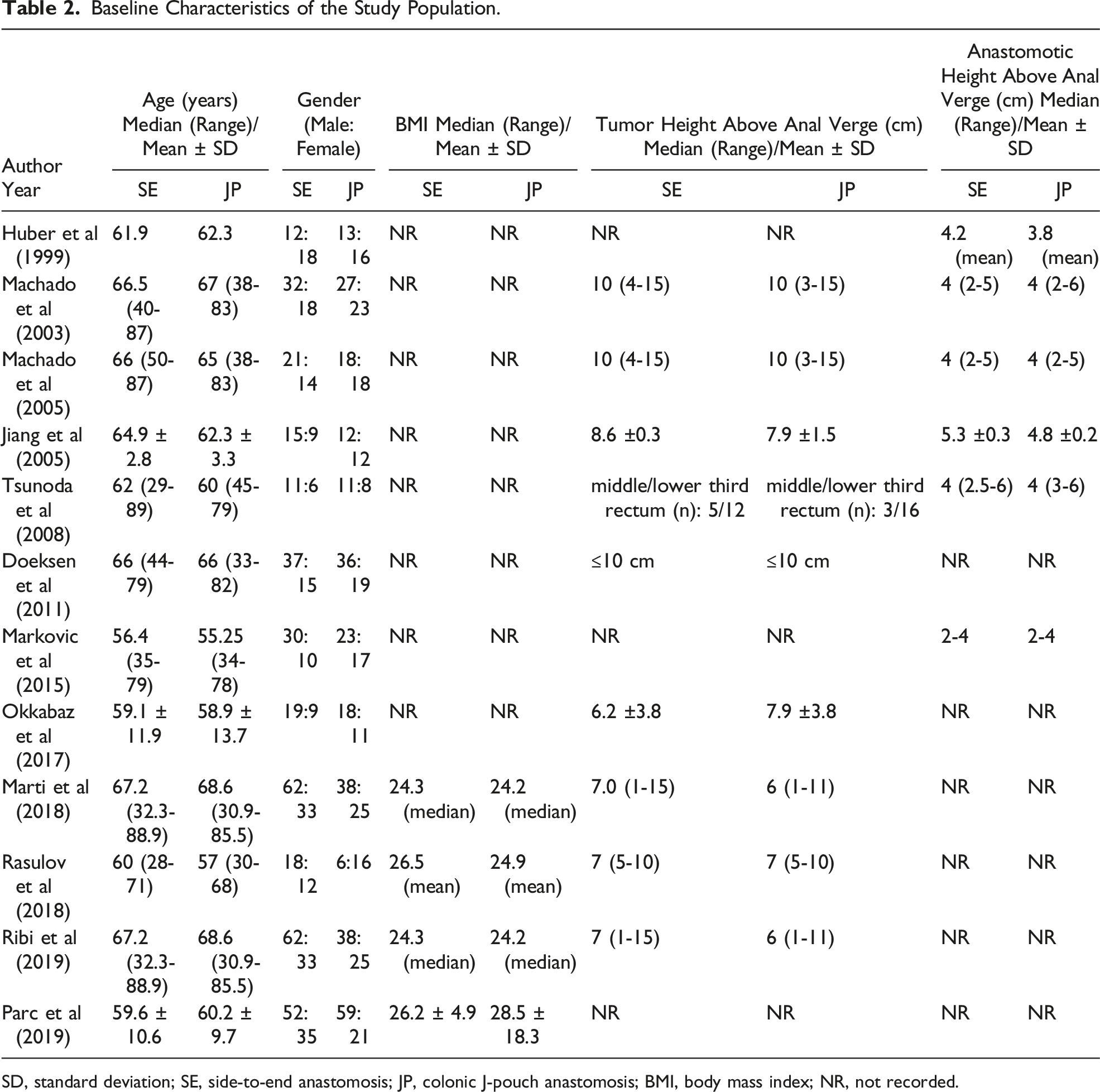
SD, standard deviation; SE, side-to-end anastomosis; JP, colonic J-pouch anastomosis; BMI, body mass index; NR, not recorded.
Risk of bias assessment for the RCTs and observational studies is shown in Figure 2 and Table 3, respectively. Risk of bias assessment of included randomized controlled trials. (A) Risk of bias summary, (B) Risk of bias graph. Methodological Quality of Observational Studies Assessed using the Newcastle–Ottawa Scale (NOS).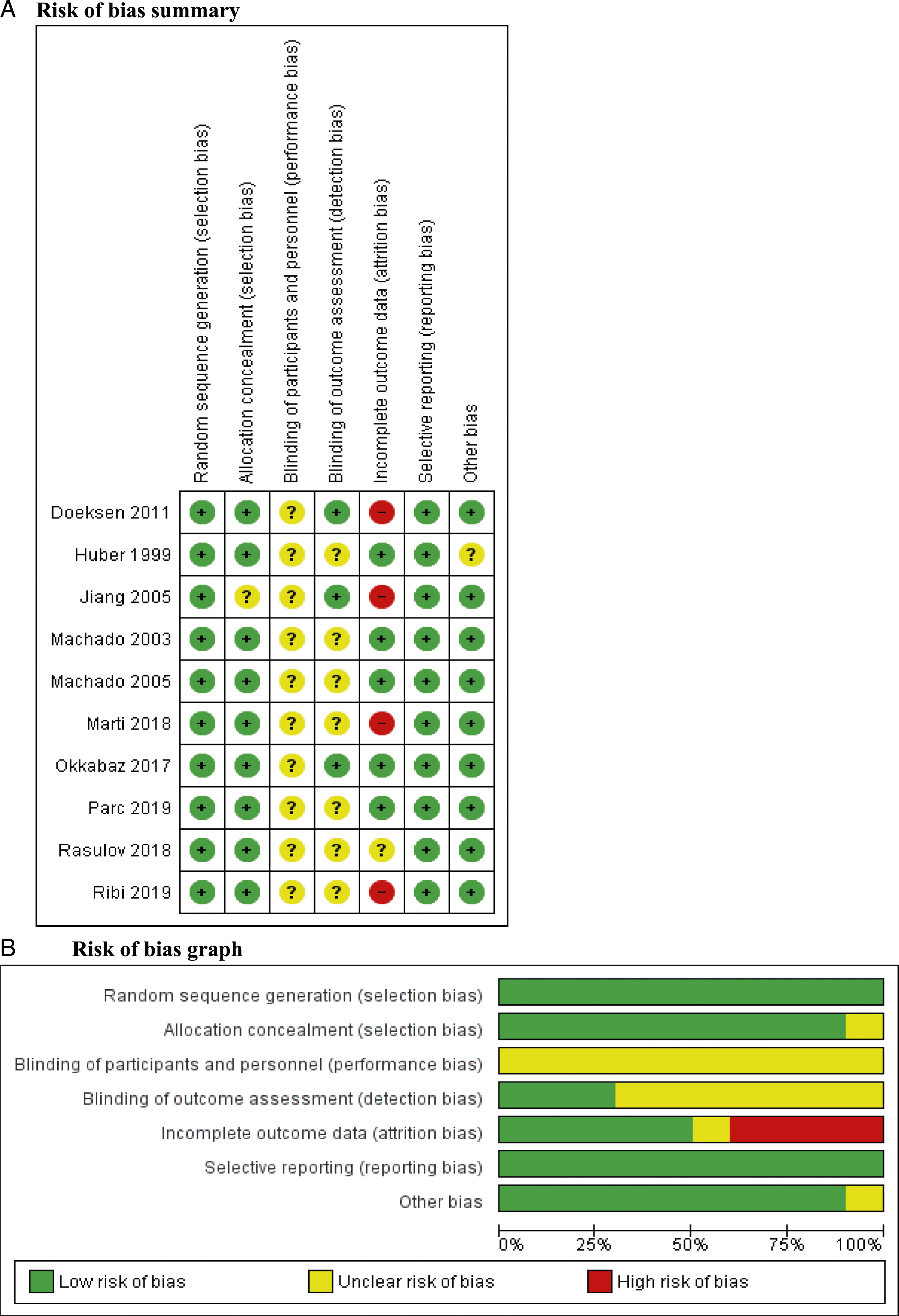
Outcomes
Primary Outcomes
Total operative time (minutes)
Operative time was reported in five studies24,28,30,31,34 (n = 408) with no significant difference between the side-to-end and CJP group [MD: −5.65; 95% CI -33.47, 22.17, P = .69]. The between-study heterogeneity was high (I2 = 87%, P < .00001).
Intra-Operative Blood Loss (mL)
Intra-operative blood loss was reported in four studies24,28,30,34 (n = 257) with no significant difference between the two groups [MD: 6.82; 95% CI -100.14, 113.78, P = .90]. The between-study heterogeneity was high (I2 = 84%, P = .0004).
Anastomotic Leak Rate
Six studies24,26,27,30-32 with 519 patients reported on post-procedure anastomotic leak with rates of 11.7% (CJP group) and 7.3% (side-to-end group), respectively. No significant difference was seen [OR: 1.35; 95% CI .7, 2.62, P = .37] and the level of heterogeneity detected between the included studies was low (I2 = 2%, P = .41).
Return to Theater
Two studies24,30 (n = 157) reported on return to theater with 10.1% and 10.3% in the CJP and side-to-end group, respectively. The results were not statistically significant [OR: 1.14; 95% CI .22, 5.94, P = .88]. Cochran Q test revealed a moderate level of between-study heterogeneity (I2 = 30%, P = .23).
Post-Operative Urinary Tract Infection
Urinary tract infection (UTI) was reported in three studies24,27,28 (n = 255) with a higher rate in the CJP group (6.9%) compared with the side-to-end group (3.9%). However, there was no significant difference [OR: 1.61; 95% CI .52, 5.01, P = .41] and a low level of heterogeneity existed between the studies (I2 = 0%, P = .49).
Recto-Vaginal Fistula Formation
Three studies26,28,31 reported on the incidence of post-operative recto-vaginal fistula formation with no significant difference between the groups [OR: 1.05; 95% CI .21, 5.32, P = .95]. No significant between-study heterogeneity was detected (I2 = 0%, P = .42).
Anastomotic Stricture/Stenosis Occurrence
Anastomotic stricture or stenosis was reported in four studies24,28,30,31 (n = 312) with rates of 3.5% (CJP group) and 2.7% (side-to-end group), respectively. No significant difference was observed [OR: 1.12; 95% CI .31, 4.02, P = .41] and the Cochran Q test revealed a low level of between‐study heterogeneity (I2 = 0%, P = .43).
Mortality Rate
Four studies24,27,28,30 (n = 312) reported on mortality rate, estimated as 1.9% (CJP) and 1.3% (side-to-end group) with no significant difference between them [OR: 1.19; 95% CI .21, 6.82, P = .84]. A low level of between-study heterogeneity was observed (I2 = 0%, P = .47).
Functional Bowel Outcomes
Stool frequency and urgency (3, 6 and 12 months)
Post-operative stool frequency over a 24-hour period and stool urgency were evaluated at 3, 6, and 12 months. Varying number of studies reported on these outcomes at different time intervals. No significant difference was detected for either of these outcomes between the two groups at the various time intervals (Figure 3). Forest plots of comparison of (1) total operative time (minutes), (2) intra-operative blood loss (mL), (3) anastomotic leak rate, (4) return to theater, (5) post-operative urinary tract infection, (6) recto-vaginal fistula formation, (7) anastomotic stricture/stenosis occurrence, (8) mortality rate, (9) stool frequency per day (3 months), (10) stool frequency per day (6 months), (11) stool frequency per day (12 months), (12) stool urgency (3 months), (13) stool urgency (6 months), (14) stool urgency (12 months), (15) tenesmus, (16) anal resting pressure (mmHg) at 2 years, (17) resting pressure volume (mL) at 6 months, (18) anal squeeze pressure (mmHg) at 2 years, (19) maximum anorectal volume (mL) at 6 months, and (20) maximum anorectal volume (mL) at 2 years. The solid squares denote the odds ratio or mean difference. The horizontal lines represent the 95% confidence intervals (CIs), and the diamond denotes the pooled effect size. CJP, colonic J-pouch; M–H, Mantel–Haenszel test.
Tenesmus (6 months)
Tenesmus 6 months post procedure was reported in three studies24,26,28 (n = 70) with 42.7% in the CJP group and 29.3% in the side-to-end group. This was significantly higher in the CJP group [OR: 2.07; 95% CI 1.06, 4.02, P = .03] with no significant heterogeneity detected between studies (I2 = 0%, P = .91).
Anal resting pressure (2 years)
Anal resting pressure (mmHg) 2 years post-operatively was reported by two studies25,28 (n = 119) and was significantly higher in the side-to-end group compared with the CJP configuration [MD: −8.76; 95% CI -15.91, −1.61, P = .02]. Cochran Q test revealed significant between-study heterogeneity (I2 = 90%, P = .002).
Other Functional Bowel Outcomes
Other functional bowel outcomes that were evaluated included resting pressure volume (mL) at 6 months,26,28 anal squeeze pressure (mmHg) at 2 years,25,28 maximum anorectal volume (mL) at 6 months,26,28 and 2 years,25,28 respectively (Figure 3).
These outcomes were reported in two studies and no significant difference was observed between the groups. Cochran Q test revealed significant between-study heterogeneity.
Sub-Group Analysis
Sub-group analysis was performed for the following outcomes: stool frequency (3, 6, and 12 months post-operatively), stool urgency (3, 6 and 12 months post-operatively) and anastomotic leak rate. Conducting sub-group analysis separately for RCTs and observational studies resulted in no change in the direction of the corresponding forest plots (Figure 4). Sub-group analysis forest plots of comparison of (1) stool frequency per day (3 months), (2) stool frequency per day (6 months), (3) stool frequency per day (12 months), (4) stool urgency (3 months), (5) stool urgency (6 months), (6) stool urgency (12 months), and (7) anastomotic leak rate. The solid squares denote the odds ratio or mean difference. The horizontal lines represent the 95% confidence intervals (CIs), and the diamond denotes the pooled effect size. M–H, Mantel–Haenszel test.
Outcome Synthesis
Discussion
Our recent comparative review of outcomes following straight (end-to-end) vs CJP anastomosis after low anterior resections found that the J-pouch was associated with a lower risk for anastomotic leak and re-operation. 35 Furthermore, better functional outcomes such as stool frequency were achieved using the CJP reconstruction over the straight anastomosis. 35 However, not all patients are considered suitable anatomically for creation of a J-pouch. A modified technique such as a side-to-end configuration may help to address/overcome these challenges while maintaining functional advantages over the end-to-end anastomosis.
Two recent meta-analyses of RCTs have suggested that the CJP and side-to-end anastomosis are comparable in terms of functional outcomes, QoL parameters, and peri-operative outcomes.5,17 We conducted an updated review and meta-analysis to include all study types to evaluate clinical, functional, and anorectal physiology outcomes between these two surgical procedures.
The review by Wang 5 included seven trials and 696 patients, whilst Hou et al 17 had 864 patients from ten publications. We add to the existing knowledge base by including results from additional observational studies with a total of 1125 patients.
We found comparable peri- and post-operative clinical outcomes between the two surgical approaches. Of the functional bowel outcomes analyzed, only the sensation of incomplete bowel evacuation (tenesmus) was found to be significantly higher in the CJP group at 6 months. Most of the analyzed anorectal physiology parameters were not significantly different between the two groups. However, anal resting pressure 2 years post-operatively was noted to be significantly higher in the side-to-end group compared with the CJP configuration.
Recent surgical advances have resulted in improved clinical and oncological outcomes with emphasis now on improving QoL parameters and post-operative bowel function. These functional outcomes may be improved with the creation of reservoirs after low anterior resection for rectal cancer. 36 1 such reconfiguration strategy is the side-to-end bowel anastomosis. It may be useful in cases where CJP creation proves difficult due to anatomical limitations and has comparable surgical outcomes. Prospective randomized trials have suggested that a CJP may not be achievable in a quarter of cases of distal rectal cancer surgery.37,38 Moreover, the side-to-end anastomosis is associated with a reduced sensation of incomplete stool evacuation and a higher anal resting pressure long term.
This latter outcome is an important finding as the pressure is indicative of the baseline tonicity of the internal and external anal sphincters. Average resting and anal squeeze pressures are generally low in incontinent patients.
Doeksen et al 27 reported better functional outcomes (stool frequency and incontinence) in the J-pouch group compared with side-to-end anastomosis at 4- and 12 months post reversal of stoma. However, these outcomes were reported as a summary score on the COloREctal Functional Outcome scale and the advantages were present at baseline. A further study (limited by several biases) also showed a significant reduction in stool frequency in favor of the CJP group up to 36-months post procedure. 39
Machado et al24,25 showed no significant difference in incontinence between the two groups at any time point. Similarly, studies have also suggested no significant differences in faecal urgency24,26 and anti-diarrheal use between the two groups.25,28 Overall, in keeping with the literature4,40 our findings (other than sensation of complete stool evacuation and anal resting pressure) failed to reveal any significant differences in functional endpoints during the early, intermediate, or late post-operative phase.
Doeksen et al 27 also compared QoL parameters between the two groups. Using the EORTC QLQ-CR38 and Short Form 36 (SF-36) questionnaires, they found no significant differences at any time points.
The superiority of the CJP in terms of functional outcomes over the end-to-end anastomosis has already been demonstrated. Functional and anorectal physiology outcomes following a side-to-end anastomosis seem to be comparable to J-pouch formation. Therefore, it can be inferred that the side-to-end technique may be advantageous in terms of post-operative bowel function compared to the straight configuration. However, long-term data is lacking to make robust conclusions about the superiority of any of the reconstruction techniques. Additionally, complicating factors such as the use of chemo-radiotherapy need to be considered as they may potentially impact long-term bowel function. 41 Nevertheless, the technically less demanding side-to-end anastomosis (in selected cases) offers a suitable alternative in sphincter-saving surgery.
This meta-analysis is not without its limitations. High levels of heterogeneity existed between the included studies for some of the outcome parameters and sensitivity analysis was unable to reduce this. Moreover, we included a mixture of RCTs and observational data. Two of our RCTs reported different outcomes from the same cohort resulting in two separate publications potentially introducing bias in our analysis. Anorectal physiology was inconsistently reported making it challenging to analyze and interpret these parameters. To ensure universality and standardization amongst authors and researchers the International Anorectal Physiology Working Group (IAPWG) recently released a position paper on its recommendations. 42
Other factors such as female sex, advanced age, and parity are associated with a deleterious effect on sphincter and rectal sensory function and these need to be considered when interpreting data.
In this study we did not analyze outcomes such as nocturnal stool incontinence, stool deferment and fragmentation, and differentiation between flatus and faeces. Additionally, the use of anti-diarrheal agents was inconsistently reported and the data insufficient to allow meaningful analysis. These are important elements of bowel dysfunction associated with LARS.
Conclusion
Clinical and functional outcomes from CJP surgery and side-to-end coloanal anastomosis are comparable. Neither technique appears to proffer solution to LARS in the short term but future well-designed, high-quality randomized trials with long term follow-up are required.
Supplemental Material
Supplemental Material - Comparison of the Colonic J-Pouch Versus Side-to-end Anastomosis Following Low Anterior Resection: A Systematic Review and Meta-Analysis
Supplemental Material for Comparison of the Colonic J-Pouch Versus Side-to-end Anastomosis Following Low Anterior Resection: A Systematic Review and Meta-Analysis by Shafquat Zaman, Elizabeth Peterknecht, Pratik Bhattacharya, Adewale A. Ayeni, Helen Gilbody, Adil N. Ahmad, Ali Y.-Y. Mohamedahmed, and Akinfemi Akingboye in The American Surgeon
Footnotes
Author Contributions
Study conceptualization: AYYM, AA & AA
Methodology: SZ, AYYM, AA
Data curation: EP, PB, AA, HG
Formal data analysis: PB, AYYM
Writing of original draft: SZ, EP, PB
Review and editing of manuscript: ANA, AA
Final approval: All authors
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Mr Akinfemi Akingboye
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.