
Abstract
Background
Ostomy reversal is a common surgical procedure; however, it is not without associated risks. Patient selection for this elective procedure is therefore critically important. Elderly patients represent a growing population and a substantial proportion of patients that present for evaluation after ostomy creation due to the most common etiologies. This study aims to assess the impact of frailty on the outcomes of ostomy reversal among older adults.
Methods
Patients ≥65 years who underwent ostomy reversal from 2015 to 2019 were identified in the NSQIP database. Frailty was calculated using the 5-item Modified Frailty Index (MFI). Multivariate regression was performed to evaluate the association of frailty with post-operative 30-day mortality, 30-day serious complications, discharge to a facility, and 30-day readmission.
Results
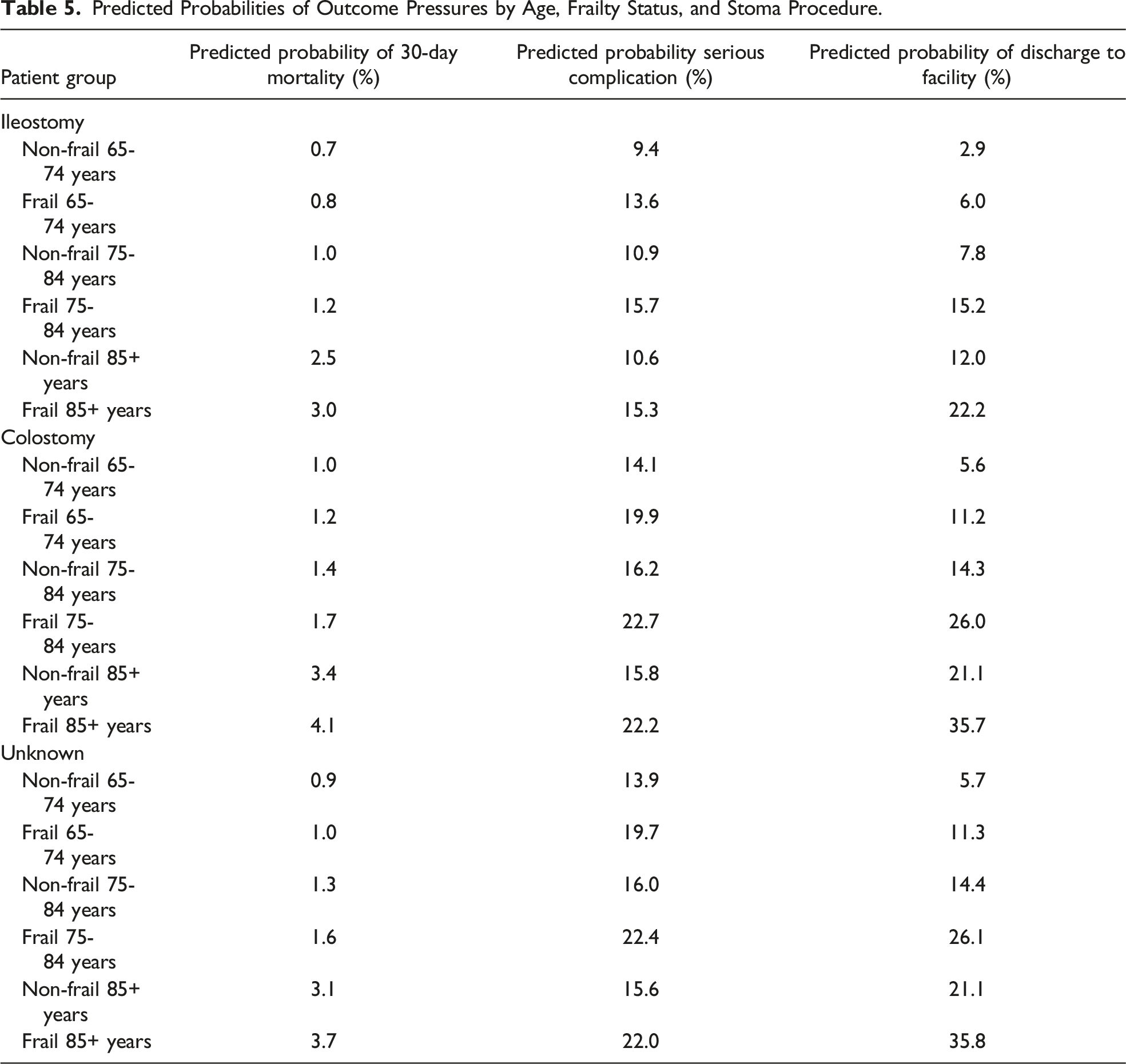
A total of 13,053 patients were included, of which 18.7% were frail (MFI ≥ 2). Patients who underwent colostomy reversal had higher rates of serious complications (P < .0001) and discharge to facility (P < .0001) compared to other reversals. In multivariate analysis, frailty was associated with increased odds of serious complications (OR 1.52, 95% CI 1.31-1.77), discharge to facility (OR 2.14, 95% CI 1.79-2.57), and readmission (OR 1.23, 95% CI 1.04-1.46), but not mortality. Frail patients had predicted probabilities 1.4 times higher for serious complications and 1.7-2.2 times greater for discharge to facility than non-frail patients.
Conclusions
Among older adults undergoing elective ostomy reversal, frailty is independently associated with increased odds of 30-day serious complications, discharge to facility, and 30-day readmission. As a potentially modifiable risk factor, identification of frailty offers the opportunity for shared decision-making and prehabilitation.
Introduction
In an aging US population, patient selection for elective surgery has become increasingly important since advanced age is a risk factor for increased post-operative morbidity and mortality. Older adults have worse outcomes than younger patients across surgical specialties, which is partially due to burden of comorbidities. Therefore, the decision to offer elective surgery to older adults can be complex, and the risks and benefits of the procedure must be taken into account. There is growing awareness, however, that age alone is not always a reliable predictor of post-operative outcomes. The concept of frailty has seen increasing attention in the literature, as this factor incorporates health parameters beyond chronological age such as physiologic reserve, social support, and psychological status.1,2 Multiple frailty metrics have been developed with significant variation in the complexity of different instruments.3–6 The 5-item Modified Frailty Index (MFI), which accounts for comorbidities and functional status, has been shown to predict outcomes in both general7–9 and colorectal surgery.10–12
Ostomy creation is common in general and colorectal surgery and can be performed in both the elective and emergent setting. Common indications for ostomy creation include diverticular disease and colorectal cancer, which are each seen with increasing frequency in older populations.13,14 While ostomy creation is often necessary at the time of the original procedure to reduce perioperative complications, the presence of an ostomy can be associated with decreased quality of life which may prompt discussions about ostomy reversal. 15 Elective ostomy reversal is highly desired by most patients; 16 however, it is not without associated morbidity, and therefore, careful evaluation of the risk/benefit ratio is needed in vulnerable older adults. 17 Prior studies examining the outcomes of ostomy closure have included a general population,18–21 but few have focused on older adults.22,23 Few prior studies have specifically evaluated the role of frailty in predicting outcomes of ostomy closure in older adults. 24
Therefore, the aim of this study is to assess the impact of frailty on post-operative outcomes of older adults undergoing elective ostomy reversal. Specifically, the study identifies the impact of frailty, as measured by the 5-item MFI, on the perioperative outcomes of 30-day mortality, 30-day serious complications, discharge to skilled nursing facility, and 30-day readmission. We hypothesize that frailty is associated with increased negative outcomes among older adults undergoing elective ostomy reversal.
Methods
Data Source
This was a cohort study of patients undergoing elective ostomy reversal using the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database. The NSQIP registry includes prospectively collected surgical patient data from over 700 hospitals including demographics, perioperative variables, and 30-day outcomes. This study was deemed exempt by the Institutional Review Board of the University of California Los Angeles.
Patient Selection
CPT Codes for Ostomy Reversal Used as Inclusion Criteria for Study Population and ICD Codes for Ileostomy and Colostomy Subgroups.
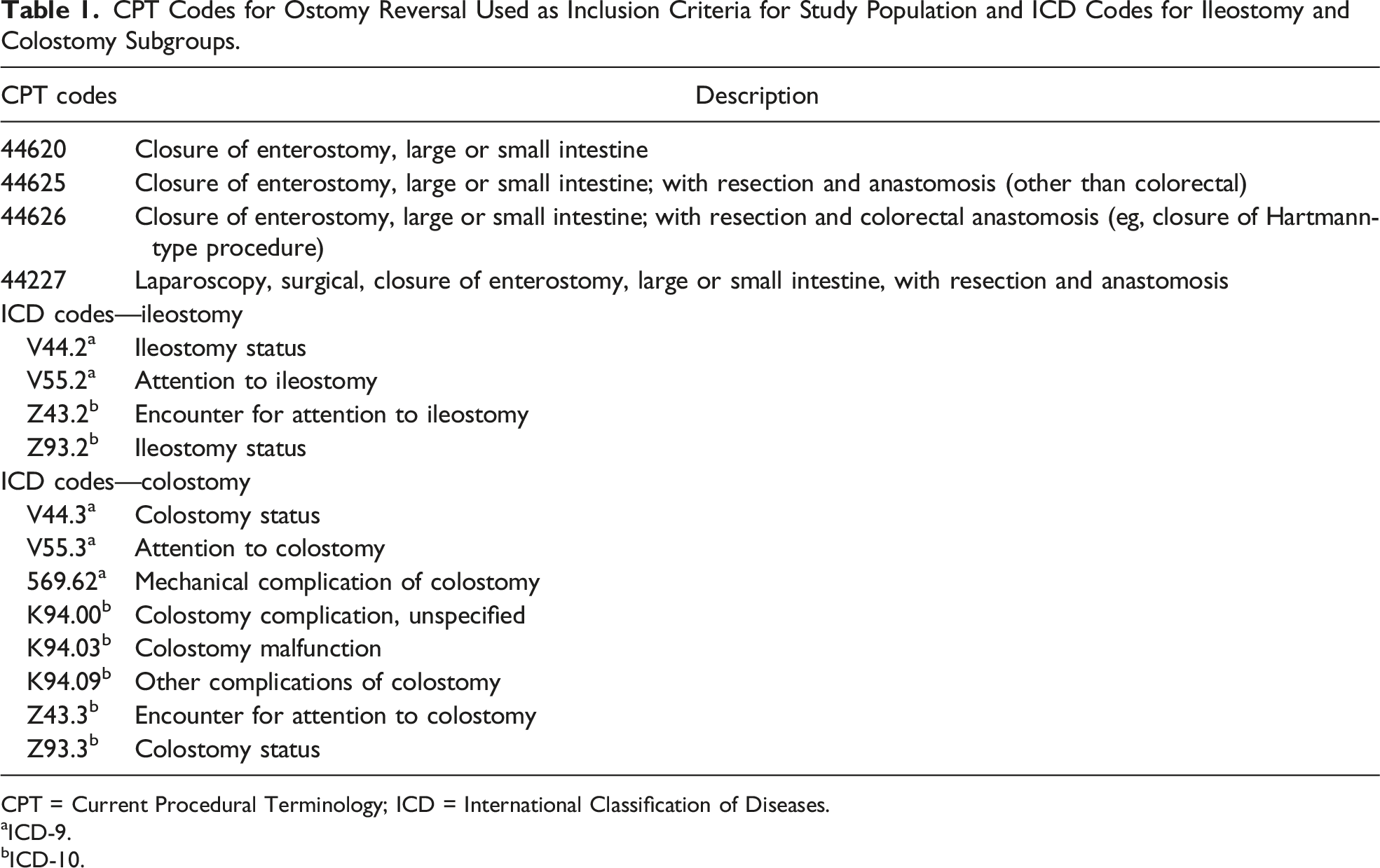
CPT = Current Procedural Terminology; ICD = International Classification of Diseases.
aICD-9.
bICD-10.
Primary Regressor of Interest
The 5-item MFI was the primary regressor of interest. The 5-item MFI is calculated using 5 variables: diagnosis of congestive heart failure, diagnosis of diabetes, diagnosis of chronic obstructive pulmonary disease, diagnosis of hypertension requiring medication, and dependent functional status (either “partially” or “completely” dependent). 5 The presence of each item is given 1 point, for a total score of 0-5. Frailty is defined as a score of ≥2.
Other Predictor Variables
Patient characteristics of age, sex, race/ethnicity, body mass index (BMI), and active tobacco use (tobacco user within 1 year of surgery) were included as predictor variables. Age was categorized into 3 groups: 64-74 years, 75-84 years, and 85+ years. Body mass index was categorized into 2 groups based on the cutoff for defining obesity: BMI <30 kg/m2 and BMI ≥30 kg/m2. Additionally, preoperative laboratory values of serum creatinine (mg/dL) and albumin (g/L) levels were also included.
Outcomes
The outcomes of interest were 30-day mortality, 30-day serious complications, discharge to a facility, and 30-day readmission. The definition of serious complications was based on the ACS NSQIP surgical risk calculator, which defines 30-day serious post-operative complications as cardiac arrest, myocardial infarction, renal insufficiency, acute renal failure, reintubation, pneumonia, venous thromboembolism, wound dehiscence, deep incisional or organ space surgical site infections (SSIs), systemic sepsis, urinary tract infection, or reoperation. 25 A subanalysis of serious complications was performed to evaluate differences in individual complications by ostomy procedure.
Statistical Analysis
STATA version 16 (Statacorp, College Station, TX) was used to perform all analyses. Univariate analysis was performed using a chi-square test for categorical variables and Mann-Whitney U tests for continuous variables which were all non-normally distributed. Univariate logistic regression was performed for the 3 outcomes of interest. Variables with statistical significance in the univariate regression were included in the respective multivariate models. Patients with missing values for variables in the regression analysis were not included in the final regression. Predicted probabilities were calculated with coefficients from the multivariate models for frail and non-frail adults at each age category using marginal analysis.
Results
Bivariate Analysis
Patient Characteristics and Outcomes for the Total Cohort Including Stratification by Type of Ostomy.
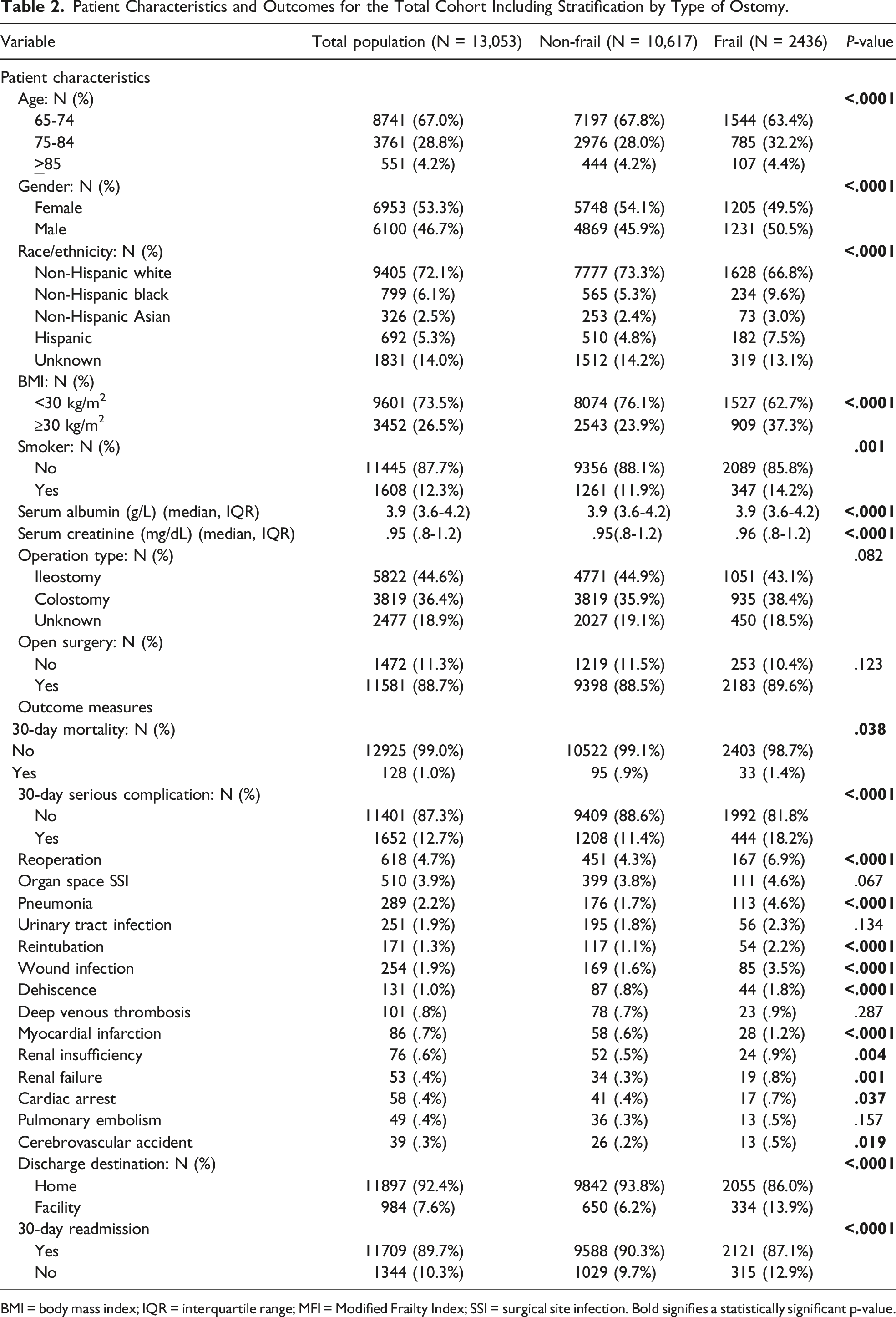
BMI = body mass index; IQR = interquartile range; MFI = Modified Frailty Index; SSI = surgical site infection. Bold signifies a statistically significant p-value.
In analysis of outcomes, there was no difference in 30-day mortality by ostomy procedure. Patients who underwent colostomy reversal did have higher rates of both serious complications (P < .0001) and discharge to facility (P < .0001) compared to those undergoing ileostomy reversal. Subanalysis revealed that reoperation, organ space SSI, and pneumonia were the most frequent serious post-operative complications (see Table 2), of which reoperation (P < .0001) and pneumonia (P < .0001) were significantly more likely to occur in frail patients. However, the 3 most common complications were significantly less likely to occur after ileostomy closure when compared to colostomy reversal or unknown operations. Rates of clostridium difficile were highest among ileostomy reversal (3.5%), compared to colostomy (2.0%) and unknown reversals (2.3%, P < .0001).
Univariate Regression Analysis
Univariate Logistic Regression of Predictor Variables With the Outcomes of 30-Day Mortality, 30-Day Serious Complication, Discharge to Facility, and 30-Day Readmissions.
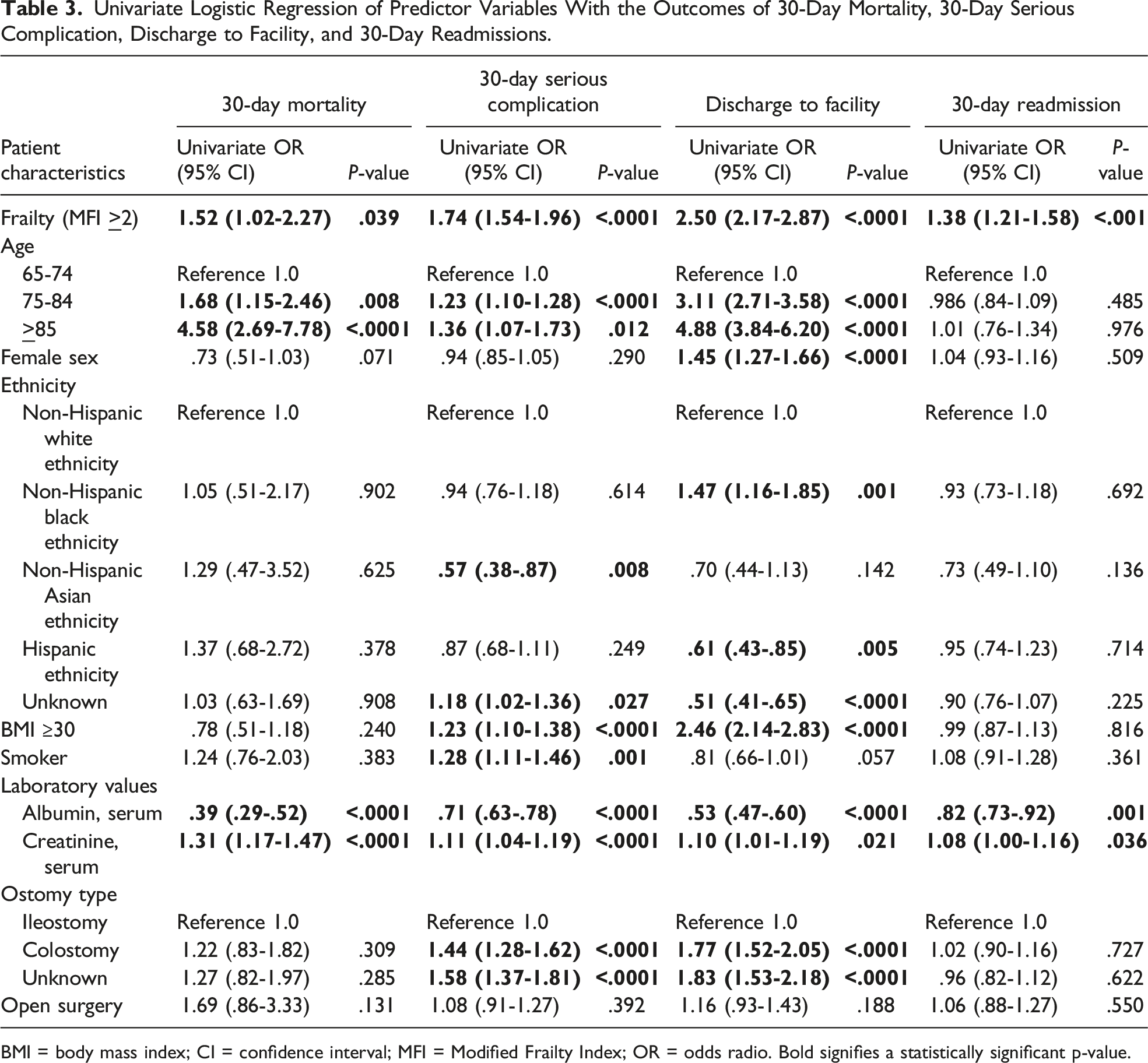
BMI = body mass index; CI = confidence interval; MFI = Modified Frailty Index; OR = odds radio. Bold signifies a statistically significant p-value.
Multivariate Regression Analysis
Multivariate Logistic Regression for Primary Outcomes of Predictor Variables With the Outcomes of 30-Day Mortality, 30-Day Serious Complication, and Discharge to Facility.
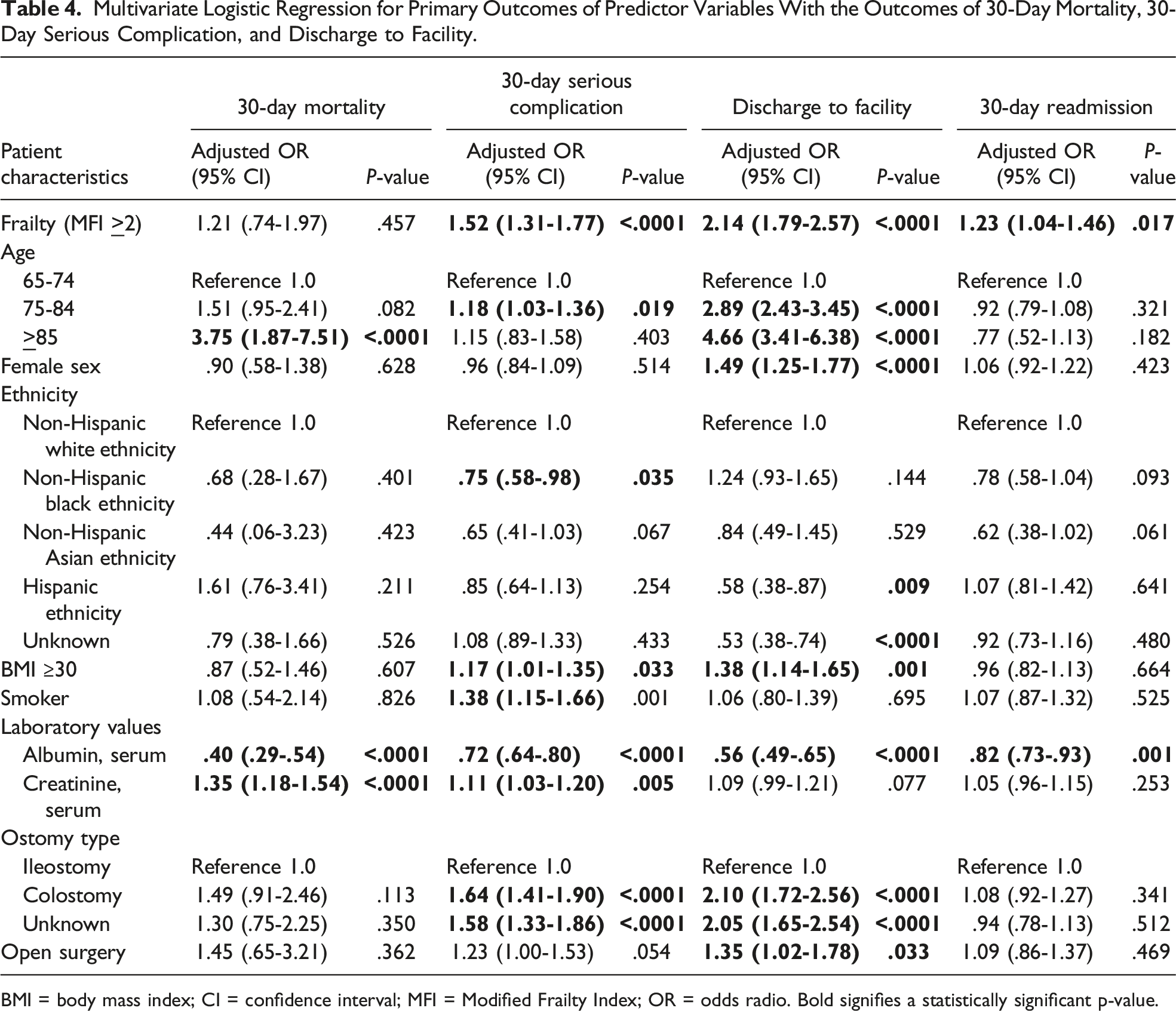
BMI = body mass index; CI = confidence interval; MFI = Modified Frailty Index; OR = odds radio. Bold signifies a statistically significant p-value.
Predicted Probabilities of Outcome Pressures by Age, Frailty Status, and Stoma Procedure.
Discussion
The current study seeks to provide information to support patient selection for an elective ostomy reversal among older adults. In this large, national database study of older adults undergoing ostomy reversal, frailty was independently associated with increased odds of adverse post-operative outcomes including 1.5 times the rate of serious complications, 2.2 times the rate of discharge to a skilled nursing facility, and 1.2 times the rate of readmission within 30 days. Age was also predictive of worse outcomes, with patients aged 85 years and older being 3.7 times more likely to die within 30 days after surgery and over 4.5 times more likely to be discharged to a facility compared to patients of ages 65-74 years. In addition, patient risk factors of obesity and tobacco use also predicted serious short-term complications. Finally, the type of ostomy reversal also impacts outcomes with colostomy reversal (which is most commonly reversal of an end colostomy) independently associated with increased odds of serious complications and discharges to facility when compared to ileostomy reversal. Frailty was associated with higher predicted probability of serious complications and discharge to facility among patients who underwent both ileostomy and colostomy reversal.
While age as a deciding factor is appealing in its simplicity, the literature is clear that the calculus is more complex. Frailty scoring has emerged as a valuable predictor since it incorporates both functional and physiologic domains, which may provide better guidance. The elective setting, such as an outpatient visit for consideration of ostomy closure, allows for in-depth discussions and shared decision-making based on risk factors such as frailty, the oldest old (age 85+), obesity, and active tobacco use as shown in the current study. In addition, there is opportunity for risk modification with preoperative optimization of comorbidities as well as prehabilitation to potentially improve exercise tolerance, nutrition, and smoking cessation. While ostomy reversal is often desirable from a quality of life standpoint, it is important to consider the risks of this elective surgery and make sure the risk/benefit ratio is concordant with the patient’s goals of care.
Our findings are consistent with prior studies showing the negative impact of frailty on post-operative outcomes.7–12,24 Two recent systematic reviews have supported the finding that frailty is associated with worse outcomes in colorectal surgery. Maturana et al reviewed 17 studies and concluded that frail patients undergoing elective or emergent colorectal cancer surgery have more post-operative complications, and in 5 of 7 included studies found higher mortality rates among frail patients. 12 In a review by Fagard et al, frailty was again associated with more post-operative complications after primarily elective colorectal surgery, although there was no association with mortality. 11 Further, Al-Khamis et al used the ACS-NSQIP database to find that short-term outcomes after both elective and non-elective colorectal surgery were worse among frail patients, including higher morbidity, mortality, and discharge to facility. 10 Our study findings are supported by these large investigations on the impact of frailty in colorectal surgery. A recent NSQIP analysis by Kooragayala et al found frailty (also defined by the 5-item MFI) predicted worse outcomes among patients undergoing Hartmann’s reversal. 24 Interestingly, frailty was not a predictor of mortality in our elective surgery study population, and it appears that in prior literature, studies including non-elective surgery found mortality differences by frailty score. This finding likely reflects selection bias in the current cohort of patients who were selected to undergo elective ostomy reversal and likely felt to have a low risk of perioperative mortality.
The current study also examined the role of chronological age as a risk factor. Prior literature shows that in the majority of cases, age is not an independent risk factor for morbidity following ostomy reversal.18,20,26–28 For example, several studies showed that age was not associated with increased morbidity after ileostomy18,26 or Hartmann’s reversal.20,28 Similarly, Bosshardt et al found that even age over 70 years was not predictive of complications following ostomy closure. 23 In our study population, however, older age was significantly associated with some negative outcomes. Patients aged 85 years and older had higher risk of mortality, those aged 75-84 were at an increased risk of serious complications, and those aged 75 and older had higher rates of discharge to a facility. Therefore, while in our analysis older age may be predictive of worse outcomes, these findings support the use of more nuanced risk factors such as frailty since age is a non-modifiable risk factor.
New guidelines from the American Society of Colon and Rectal Surgeons (ASCRS) support the use of frailty over chronological age in perioperative care. 29 These new guidelines recommend preoperative screening for frailty and consideration of prehabilitation based on patient-specific factors that may improve outcomes. Prehabilitation can target and improve individual risk factors in multiple domains including activity level and exercise endurance, nutrition and weight loss, and psychosocial dynamics. The new ASCRS guidelines also provide a strong recommendation for the integration of prehabilitation into surgical pathways for frail patients when possible. 29 While the MFI score for a given patient may not change after prehabilitation, screening for frailty using MFI identifies at-risk patients who would benefit from optimization with the potential to reduce perioperative risk.
This study does have several limitations. First, the use of a large, retrospective database is subject to the inherent limitations of the available data. A significant proportion of the patients could not be categorized by type of ostomy procedure (ie, ileostomy vs colostomy takedown) or by underlying disease process (ie, malignant vs benign) due to non-specific coding. Second, this study is subject to selection bias as only patients who ultimately underwent ostomy closure were included. Therefore, these selected patients are likely among the most fit for elective surgery, which is supported by the overall low mortality rates seen in our data. Furthermore, the effect sizes determined by this study are likely underestimated for the same reason. In addition, despite in the growing use of preoperative frailty evaluation, there is no consensus on the optimal instrument for frailty assessment. Therefore, although the 5-item MFI has been shown to predict outcomes in general and colorectal surgery, it has been also shown to underperform in its predictive value when compared to other frailty measures. 30 However, it was nevertheless correlated with more in-depth metrics such as the Risk Analysis Index, suggesting that MFI remains a valuable marker of frailty. Finally, the outcomes studied here are limited to short-term 30-day outcomes, while the long-term outcomes such as quality of life after major surgery and functional recovery after surgery are also important to consider.
This study showed that among older adults undergoing elective ostomy reversal, frailty predicts increased odds of both 30-day serious complications and discharge to a facility independent of other variables such as age. These results add to the mounting evidence for the use of frailty as well as chronological age for preoperative assessment of surgical risk. As a potentially modifiable risk factor, identification of frailty is important for shared decision-making regarding the risk/benefit ratio of surgery as well as the opportunity for prehabilitation in this vulnerable patient population. Future studies should evaluate the association of frailty with longer-term outcomes such as quality of life or functional recovery after surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Salzman was supported by the VA office of Academic Affiliations through the National Clinician Scholars Program.
Data Availability Statement
The ![]() given this article are: The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
given this article are: The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.