
Abstract
Background
This study aimed to determine the impact of emergency medical service (EMS) scene time variability on adult and pediatric trauma patient outcomes with moderate or severe penetrating injuries.
Methods
This retrospective study analyzed the American College of Surgeons (ACS) Trauma Quality Improvement Program (TQIP) database between 2017 and 2020 to evaluate the relationship between EMS scene time on adult and pediatric patients with moderate to severe injuries. Primary outcomes included Dead on Arrival (DOA) to the Emergency Department (ED), ED mortality, 24-hour mortality, and in-hospital mortality. Multivariable logistic regression models were used to examine the association of each EMS scene time category and mortality.
Results
Adult patients with 10-30 minutes of EMS scene time had increased odds of experiencing ED mortality, 24-hour mortality, and in-hospital mortality. Adults with >30 minutes of EMS scene time were more likely to be DOA to the ED. There was no significant association with mortality for patients with <10 minutes of EMS scene time. In the pediatric subset of patients, those with 10-30 minutes of EMS scene time were more likely to experience ED mortality and in-hospital mortality.
Conclusion
EMS scene times less than 10 minutes were associated with the greatest odds of survival, supporting the “load and go” theory for penetrating trauma. Our study suggests that even an EMS scene time of 10-30 minutes results in a significantly increased risk of mortality, and further efforts are needed to improve scene time through improved EMS and hospital policies.
Keywords
Introduction
Emergency medical service (EMS) personnel in the United States respond to an estimated 42 million calls annually with an average response time of 8 minutes.1,2 The first 60 minutes after a traumatic injury has occurred is often referred to as the “golden hour,” which emphasizes a timeframe for which an injured patient must receive definitive care to decrease morbidity and mortality risks. 3 In efforts to achieve effective care within this 60-minute window, two strategies for the pre-hospital management of trauma patients were developed. The first is the Franco-German model, which prioritizes on-scene treatment and stabilization of the patient; however, there has been limited evidence in managing injured patients outside of the hospital. 4 The second model, the Anglo-American model, predominates in the United States and is based on the “load and go” method, emphasizing reduced prehospital time due to fewer prehospital interventions. 5
Prehospital time intervals have not been well-defined for EMS, but previous literature has shown that minimal prehospital time is beneficial among trauma patients.6,7 Various negative outcomes including mortality have been associated with increased prehospital time; therefore, minimizing prehospital times has been encouraged by the National Association of State EMS Officials (NASEMSO).8-10 This decreased prehospital time interval is especially important among penetrating trauma with previous literature suggesting higher mortality rates among various penetrating trauma injuries.8-10
Components of prehospital time include response time, scene time, and transport time, all of which have been target areas for improvement for EMS in the United States. While response and transport times may have debated roles in prehospital outcomes, scene time has been found to be the one time interval in which EMS systems have the most power to control. 7 In penetrating trauma patients, longer prehospital time, including EMS scene time, was associated with higher mortality. 7 This is further supported by United States EMS guidelines which recommend minimizing scene time to under 10 minutes, especially for penetrating torso traumas. 8
Therefore, our study aims to examine how EMS scene time variability affects outcomes of penetrating trauma patients with moderate or severe injuries on measures of a patient being found Dead on Arrival, ED mortality, 24-hour mortality, and in-hospital mortality.
Methods
Study Design and Data Source
This retrospective study utilizes de-identified trauma patient data from the American College of Surgeons (ACS) Trauma Quality Improvement Program (TQIP) database between 2017 and 2020 to evaluate the relationship between EMS scene time and penetrating trauma injury mortality in adult and pediatric patients. The ACS TQIP is a national database that is thoroughly evaluated and screened and provides a comprehensive data dictionary that explains all included variables and any changes per year. 11
Study Population and Eligibility Criteria
Patients with an ISS ≥15 with penetrating injuries who were transported by ground EMS were selected. ISS severity ≥15 was chosen to better evaluate the effect of EMS scene time variance in severe trauma cases. Patients were stratified by age, with adults being ≥18 years of age, and pediatrics being ≤17 years of age. Cases were excluded if they lacked data pertaining to age, race, gender, ISS severity, or EMS scene time. Patients transferred from another facility or had a different mode of transport, such as aeromedical transport, were excluded. Patients were considered Dead on Arrival if they presented to the ED with no signs of life. The ED mortality was defined as a patient who died in the ED; 24-hour mortality was a patient who died within 24 hours in any setting; and in-hospital mortality was a patient who died within the hospital.
Outcomes of Interest
The primary outcomes of this study included mortality rates, specifically the number of patients who were Dead on Arrival (DOA), Emergency Department (ED) mortality, 24-hour mortality, and in-hospital mortality.
Statistical Analysis
Descriptive analysis of all variables was evaluated. Emergency medical service scene time was categorized into <10 minutes, 10-30 minutes, and greater than 30 minutes. These time parameters were set to highlight the potential benefits of decreased scene times <10 minutes in contrast to intermediate (10-30 minutes) and increased scene times (>30 minutes) on mortality outcomes on a national level. Data for adult cases were analyzed for all three time categories; however, data for pediatric cases was only assessed in the <10-minute and 10-30 minute categories due to insufficient population size for analysis in the >30-minute group. Within each scene time category, multivariate logistic regression models were used to examine the association between each covariate (ie, age, race, gender, insurance status, hospital teaching status, and verification level) and each outcome. Multivariable logistic regression models were used to examine the association of each EMS scene time category with each outcome while adjusting for patient covariates. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A P-value <.05 was considered statistically significant. IBM SPSS Statistics (Armonk, NY) v28.0 was used. This study was conducted in compliance with ethical standards, was reviewed by our institutional review board, and was deemed exempt.
Results
Patient Population Characteristics and Demographics
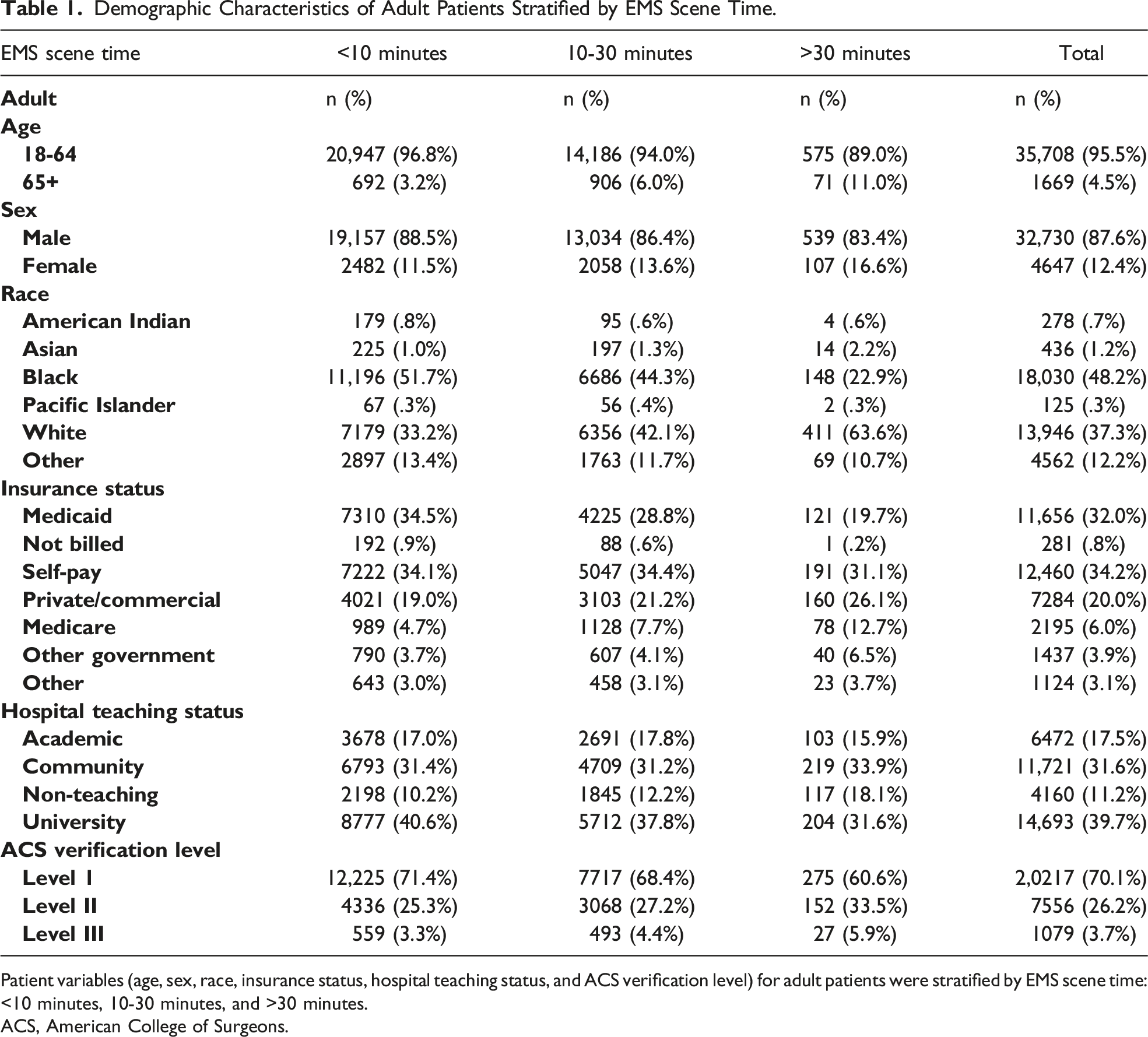
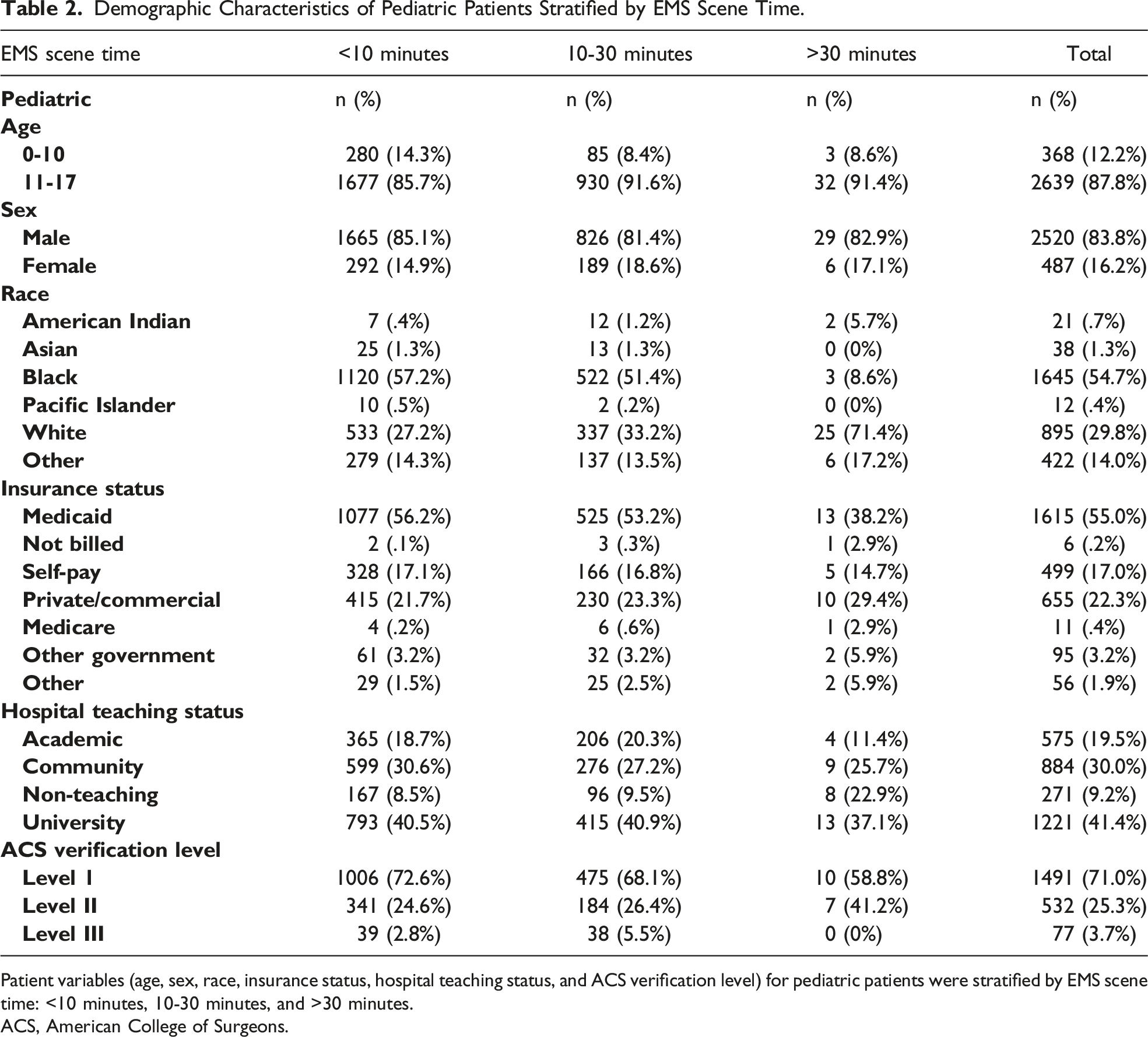
This study analyzed 37,377 adult cases (Figure 1(A)) and 3007 pediatric cases (Figure 1(B)). For patient demographics, adults were most commonly male (n = 32,730, 87.6%), Black patients (n = 18,030, 48.2%), and White patients (n = 13,964, 37.3%), with an average age of 37.1 years (Table 1). Pediatric demographics were similar for race and gender, being most commonly male (n = 2,520, 83.8%), Black patients (n = 1,645, 54.7%), and White patients (n = 895, 29.8%), with an average age of 14.5 years (Table 2). (A) Study population and inclusion characteristics in adult patients. (B) Study population and inclusion characteristics in pediatric patients. Demographic Characteristics of Adult Patients Stratified by EMS Scene Time. Patient variables (age, sex, race, insurance status, hospital teaching status, and ACS verification level) for adult patients were stratified by EMS scene time: <10 minutes, 10-30 minutes, and >30 minutes. ACS, American College of Surgeons. Demographic Characteristics of Pediatric Patients Stratified by EMS Scene Time. Patient variables (age, sex, race, insurance status, hospital teaching status, and ACS verification level) for pediatric patients were stratified by EMS scene time: <10 minutes, 10-30 minutes, and >30 minutes. ACS, American College of Surgeons.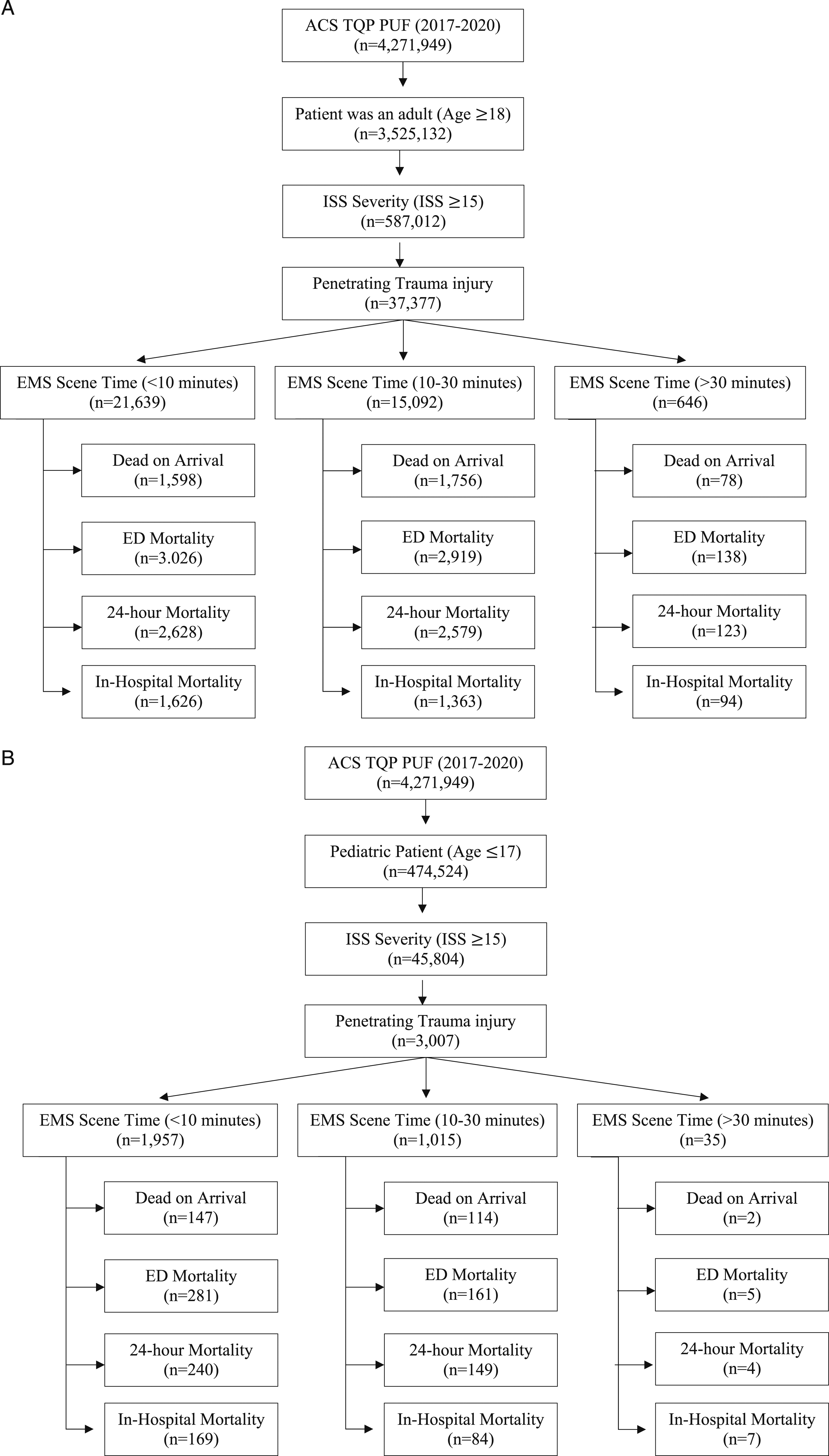
Unadjusted Outcome Measures for Adult and Pediatric Patients
For adult patients, 18.4% of patients with <10 minute scene time, 22.9% with 10-30 minute scene time, and 24.8% with scene time greater than 30 minutes were DOA. 24.1% of patients with <10 minute scene time, 30.9% with 10-30 minute scene time, and 31.8% with scene time greater than 30 minutes experienced ED mortality. 23.6% of adult patients with <10 minute scene time, 30.5% with 10-30 minute scene time, and 31.9% with scene time greater than 30 minutes experienced 24-hour mortality. 17.3% of adult patients with <10 minute scene time, 21.3% with 10-30 minute scene time, and 21.7% with scene time greater than 30 minutes experienced in-hospital mortality.
Mortality Rates in Adult and Pediatric Patients Stratified by EMS Scene Time.
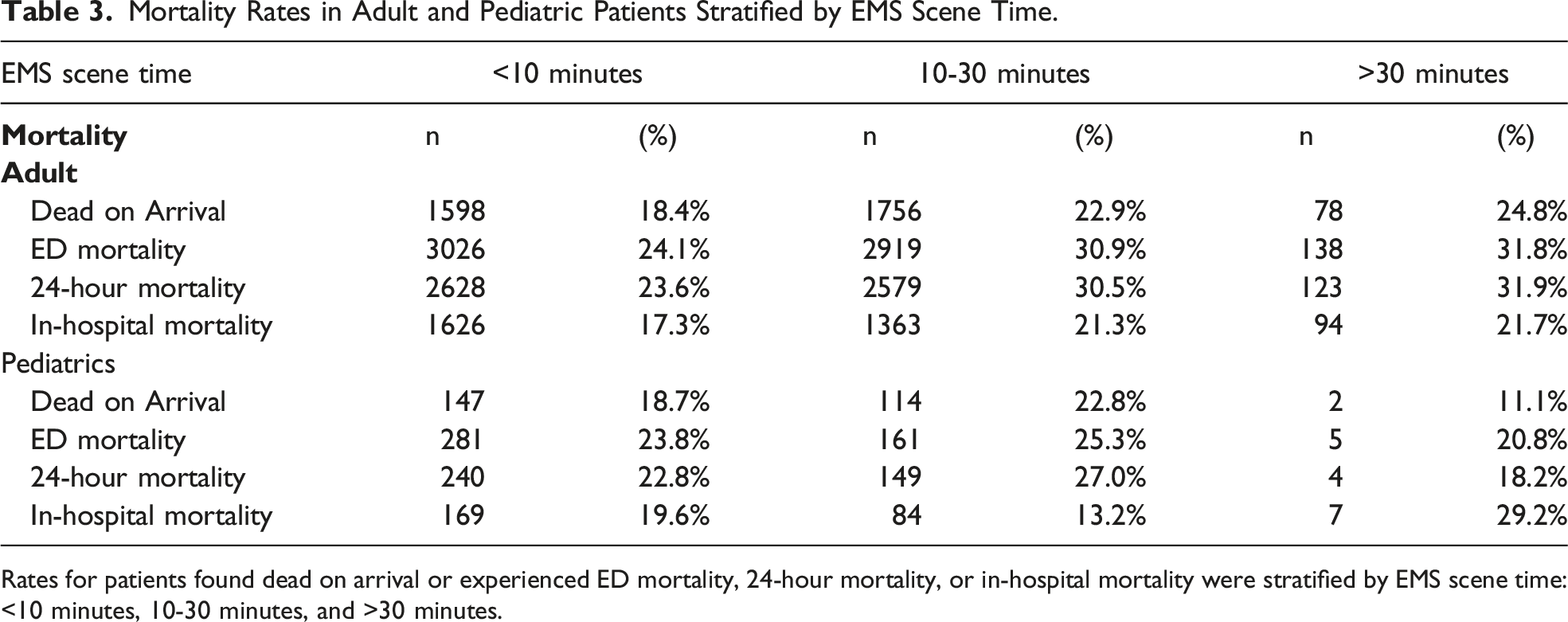
Rates for patients found dead on arrival or experienced ED mortality, 24-hour mortality, or in-hospital mortality were stratified by EMS scene time: <10 minutes, 10-30 minutes, and >30 minutes.
Adjusted Outcome Measures for Adult Patients
Dead on Arrival
Adjusted Mortality Outcomes for Adult Patients with EMS Scene Time.
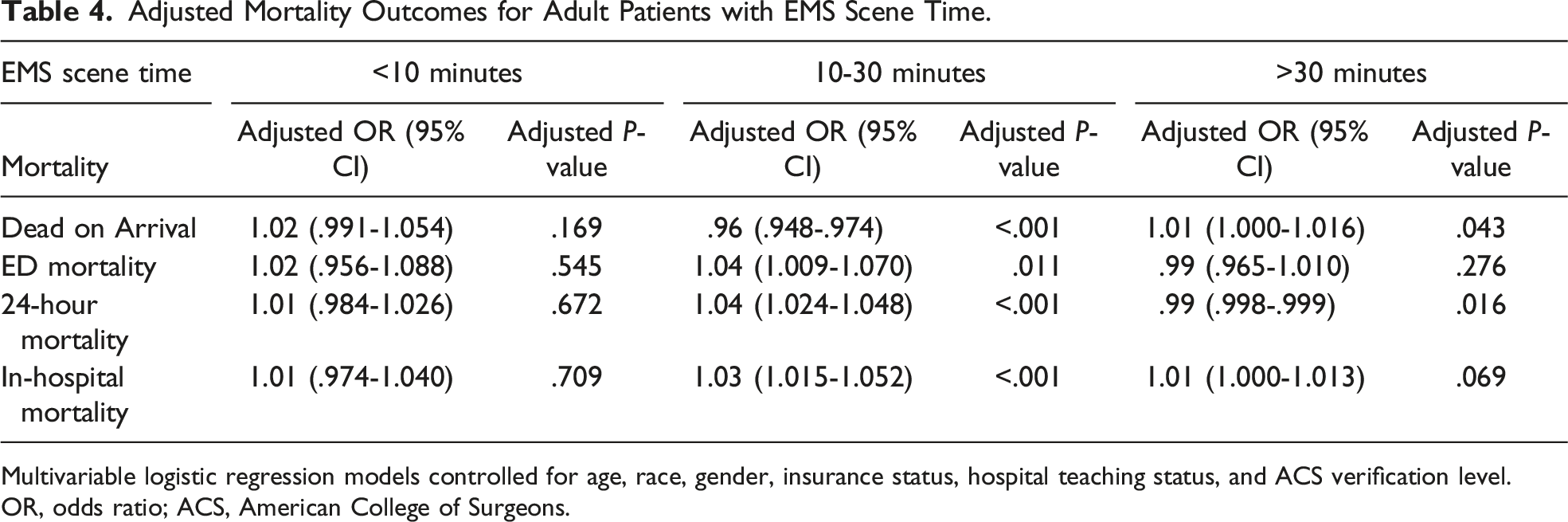
Multivariable logistic regression models controlled for age, race, gender, insurance status, hospital teaching status, and ACS verification level.
OR, odds ratio; ACS, American College of Surgeons.
ED Mortality
Adult patients with an EMS scene time between 10 and 30 minutes had higher odds of mortality in the ED (OR 1.04, 95% CI [1.009, 1.070], P = .011). Adults with EMS scene times of <10 and >30 minutes were not significantly associated with ED mortality (OR 1.02, 95% CI [.956-1.088], P = .545; OR .99, 95% CI [.965-1.010], P = .276, respectively) (Table 4).
24 hour Mortality
Adult patients with 10-30 minutes spent on-scene were more likely to experience 24-hour mortality (OR 1.04, 95% CI [1.024-1.048], P < .001); however, those with EMS scene time >30 were less likely to experience 24 hour mortality (OR .99, 95% CI [.988-.999], P = .016). Adult patients with an EMS scene time of <10 minutes were not significantly associated with 24-hour mortality (OR 1.01, 95% CI [.984-1.026], P = .672) (Table 4).
In-hospital Mortality
Patients with 10-30 minutes spent on-scene were significantly more likely to experience in-hospital mortality (OR 1.03, 95% CI [1.015-1.052], P < .001). The EMS scene times of <10 and >30 minutes were not associated with in-hospital mortality (OR 1.01, 95% CI [.974-1.040], P = .709); (OR 1.01, 95% CI [1.000-1.013], P = .069, respectively) (Table 4).
Adjusted Outcome Measures for Pediatric Patients
Dead on Arrival
Adjusted Mortality Outcomes for Pediatric Patients with EMS Scene Time.
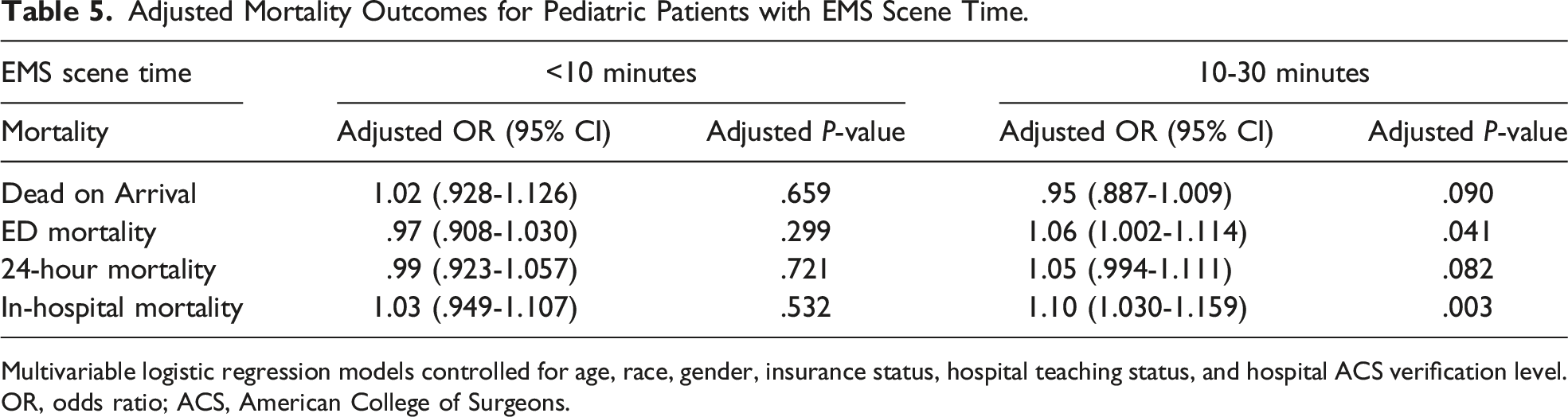
Multivariable logistic regression models controlled for age, race, gender, insurance status, hospital teaching status, and hospital ACS verification level.
OR, odds ratio; ACS, American College of Surgeons.
ED Mortality
Pediatric patients with EMS scene time of 10-30 minutes were associated with greater odds of ED mortality (OR 1.06, 95% CI [1.002-1.114], P = .041). EMS scene time of <10 minutes was not significantly associated with ED mortality (OR .97, 95% CI [.908-1.030], P = .299) (Table 5).
24-hour Mortality
Pediatric patients that had <10 minutes and 10-30 minutes on-scene time were not significantly associated with 24-hour mortality (OR .99, 95% CI [.923-1.057], P = .721; OR 1.05, 95% CI [.994-1.111], P = .082, respectively) (Table 5).
In-hospital Mortality
Pediatric patients with an EMS scene time of 10-30 minutes had higher odds of in-hospital mortality (OR 1.10, 95% CI [1.030-1.159], P = .003). EMS scene time of <10 minutes was not associated with a change in-hospital mortality (OR 1.03, 95% CI [.949-1.107], P = .532) (Table 5).
Discussion
When evaluating adult patients with 10-30 minutes of EMS scene time, they were significantly less likely to be dead on arrival, but every minute was associated with 4% higher odds experiencing ED mortality, 4% higher odds of 24-hour mortality, and 3% higher odds of in-hospital mortality. When assessing adults with >30 minutes of EMS scene time, they were more likely to be dead on arrival, however, they had decreased odds of experiencing 24-hour mortality. With respect to mortality outcomes in patients with <10 minutes of EMS scene time, there was no significant association between EMS scene time and any of the mortality outcomes. In the pediatric subset of patients analyzed, those with 10-30 minutes of EMS scene time were more likely to experience ED mortality and in-hospital mortality. However, similar to the adult population, there was no significant association found between EMS scene time of less than 10 minutes and any of the mortality outcomes.
Our results demonstrating that increasing EMS scene time is associated with worse mortality outcomes are consistent with other studies that found an association between increased prehospital times and adverse patient outcomes.7,12-15 A recent study by Waalwijk et al evaluated regional trauma systems in Europe and found that an on-scene time of 20 minutes or longer demonstrated a strong association with 24-hour and 30-day mortality, with significant associations with on-scene time per minute. 14 Similarly, McCoy et al, in a single urban Level I trauma center over a 14-year period identified increased odds of mortality with penetrating trauma if scene time was greater than 20 minutes. 7 Our study strengthens these findings in previous literature through use of a national database encompassing hospitals across the United States, expanding the studied population to include nearly 40,000 adults and 3000 pediatric patients. In addition to these studies, we identified that an EMS scene time between 10-30 minutes for penetrating injuries rather than for >20 minutes was significantly associated with mortality. Each minute within that time frame is associated with about 3-4% higher odds of death in the ED, death within 24 hours, and in-hospital mortality, suggesting that the window of 10-30 minutes of EMS scene time represents a significant loss of life that can be improved upon. This zone should be an area of focus for the development or modification of EMS protocol and policy to improve a patient’s survival following penetrating trauma.
Our study found that pediatric penetrating trauma patients with an EMS scene time of 10-30 minutes had a significantly increased risk of ED mortality and in-hospital mortality. However, these findings are inconsistent with a retrospective study by Tijssen et al that looked at the association between EMS scene time and survival to hospital discharge and found that the highest survival occurred with a scene time of 10-35 minutes. Unlike our study which focused on pediatric penetrating trauma, Tijssen et al specifically looked at out-of-hospital cardiac arrest in the pediatric population. 16 Our findings instead indicate that on-scene times of less than 10 minutes may be ideal for reducing in-hospital mortality in pediatric penetrating trauma patients, which is consistent with the 2022 National Association of State EMS Officials guidelines that emphasize minimizing on-scene time to less than 10 minutes for patients with penetrating trauma. 8 Together, our findings in the context of the literature on other pediatric emergencies highlight the importance of adjusting pre-hospital management strategies for different pathologies.
Our findings aid in the identification of moderate to severe patients with penetrating injuries who may benefit from decreasing EMS scene time. This is consistent with most other studies that have demonstrated increased benefit to hospital-based measures for survival, rather than on-scene measures. Changes on the EMS system level have the potential to save lives in the emergency department, within 24 hours, and in the hospital. Scene time is the most modifiable variable as it is composed of extraction, evaluation, and management. Shorter EMS scene times are associated with better odds of survival for penetrating injuries likely due to the requirement for radiological imaging and surgical intervention due to the anatomical complexity and non-compressible nature of large vessels. Therefore, EMS systems should focus on limiting time spent on the scene as much as possible to improve patient survival.
This analysis of the ACS TQIP dataset has several limitations. First, the unavailability of data regarding prehospital interventions and EMS transport time from the scene to the hospital within the ACS TQIP dataset may contribute to differences in mortality rates. However, EMS transport time is often considered unalterable; therefore, we believe our focus on EMS scene time is more clinically relevant and applicable. Additionally, our selection criteria for patients included penetrating injuries and moderate or severe ISS scores, reflecting decisions of severity by an appropriate trauma team, and not EMS personnel. Additionally, future studies may choose to investigate ISS severity as an adjusted covariate in a continuous fashion to better evaluate if varying severity of injury is associated with mortality and EMS scene times. Lastly, the small sample size limited our ability to analyze EMS scene time >30 minutes in the pediatric population. Interestingly, EMS scene times greater than 30 minutes did not necessarily suggest increased odds of mortality in the adult population. This may have been due to a small sample size or other factors not recorded in ACS TQIP dataset that may have increased scene time. Additionally, the magnitude of the odds ratios between EMS scene time and outcome are small. This is most likely due to the large sample size and number of covariates controlled for in the multivariable, thus diluting the odds ratio. However, we would not change the method of analysis, as we believe the sample size was appropriate to run a robust and strong analysis of EMS scene time and EMS arrival time in relation to mortality outcomes.
The debate between “load and go” vs “stay and stabilize” can be a major source of contention. 7 Our results show that a “load and go” approach might work best, as patients with an on-scene time of less than 10 minutes had lower mortality. Complicating the debate are public, political, and financial interests, which influence the care provided by EMS agencies. Additionally, local EMS systems in the United States vary in terms of policy and resources, and services rendered are often affected by unforeseen circumstances such as inclement weather or traffic based on geographical location. Although our study population was heterogeneous, policy changes on the local level should focus on minimizing scene times to less than 10 minutes, as a 10-30 minute period demonstrates significant increases in mortality risk. Future research should consider other case-specific factors or specific patient groups that benefit from minimizing EMS scene times which would allow for the specification of local guidelines for EMS scene time policy.
Conclusion
Our findings support EMS guidelines which recommend minimizing scene time to under 10 minutes, especially for penetrating traumas. In trauma patients with penetrating injuries, an EMS scene time of 10-30 minutes was associated with an increased risk of overall mortality, including ED mortality, 24-hour mortality, and in-hospital mortality in adults, and only ED and in-hospital mortality in pediatrics. As EMS scene time increased across our time categories, patients were more likely to be dead on EMS arrival. The EMS scene times of less than 10 minutes were associated with the greatest odds of survival, supporting the “load and go” theory for penetrating trauma. Our study also shows that even an EMS scene time of 10-30 minutes results in a significantly increased risk of mortality, and further efforts are needed to improve scene time through improved EMS and hospital policies.
Footnotes
Author’s Note
All authors read and approved the final manuscript.
Author Contribution
Study design and conception: AE.
Data collection, analysis, and interpretations: AR, TB, MA, and AE.
Manuscript preparation: AR, TB, MA, BM, PM, and AE.
Critical revision of the manuscript: AR, TB, MA, BM, PM, and AE.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.