
Abstract
Alkaline reflux esophagitis is a recognized complication of procedures that compromise the lower esophageal sphincter (LES), including gastrectomy. Incidence of reflux is dependent on the reconstructive procedure, with Roux-en-Y (RY) esophagojejunostomy commonly accepted as the optimal method. The authors report their experience of 5 patients who underwent remedial intervention for severe alkaline reflux esophagitis following gastric cancer surgery, over a 6-year period (2014-2020). Primary diagnoses encompassed 4 gastric adenocarcinomas and 1 gastric neuroendocrine tumor. Four patients previously underwent total gastrectomy and 1 subtotal gastrectomy with RY reconstruction. Onset of postoperative reflux symptoms ranged from 2 weeks to 3 years. Failing medical management, all patients underwent jejunojejunal anastomosis and Roux limb length revision with surgical jejunostomy. At follow-up, 4 out of 5 patients had some degree of symptom resolution and one with unresolved symptoms. The authors report our experience of managing this complication following gastrectomy with jejunojejunal anastomosis and Roux limb length revision.
Introduction
Alkaline reflux esophagitis (ARO) is a recognized complication of procedures that compromise the lower esophageal sphincter (LES), including gastrectomy. Incidence of reflux is dependent on the reconstructive technique, with Roux-en-Y (RY) esophagojejunostomy commonly accepted as the optimal method. 1 Roux-en-Y reconstruction significantly decreases the incidence of this complication; however, when it does occur, it is often challenging to manage. Alkaline reflux esophagitis results from mucosal injury secondary to jejunal contents passing into the esophagus.
Initial management of ARO is conservative, entailing anti-reflux medication and lifestyle advice. Failing this, surgical intervention is required. Roux-en-Y reconstruction has been shown to reduce debilitating symptoms of ARO and improving patient quality of life. It also reduces the risk of long-term complications of ARO including Barrett’s esophagus and potential for malignant transformation. 2 The authors report their experience of 5 patients who underwent remedial intervention for severe alkaline reflux esophagitis following gastric surgery.
Approach at Our Center
Operations Performed
These 5 patients were managed in a national tertiary center over a 6-year period (2014-2020). Ethical approval was granted by the St. James’s Hospital Dublin ethics committee for purpose of audit. This center performs high volume upper gastrointestinal resectional surgery, undertaking a mean number of 54 esophagectomies and 29 gastrectomies annually during the study period described. Overall, 3/5 had their initial resectional surgery at this unit, with the remaining 2/5 undergoing surgeries elsewhere. From the ones performed in this unit, the overall prevalence of revisional surgery for (i) gastrectomies in total was 3/204 (1.27%), (ii) total gastrectomy (TG) was 2/124 (1.6%), and (iii) subtotal gastrectomy (STG) was 1/49 (2%).
Management
The management of reflux symptoms consists of – sucralfate, dietary counseling and in cases of failure, significant impact on health-related quality of life (HRQL), nutrition and esophagitis, and evidence of short or sub-optimal Roux limb length the center would offer a revisional surgery.
Roux Limb Lengthening
In regards to the revisional surgery, in all cases there is revision to the RY anastomosis in order to lengthen the limb, with average lengthening of limb being 40.5 cm, but ranging from 35-65 cm from original anastomosis site. There were no significant intraoperative or postoperative complications, and there were no intraoperative or perioperative deaths.
Clinical Summary
Baseline Characteristics of Post-Gastrectomy Patients With Severe Alkaline Reflux Esophagitis.
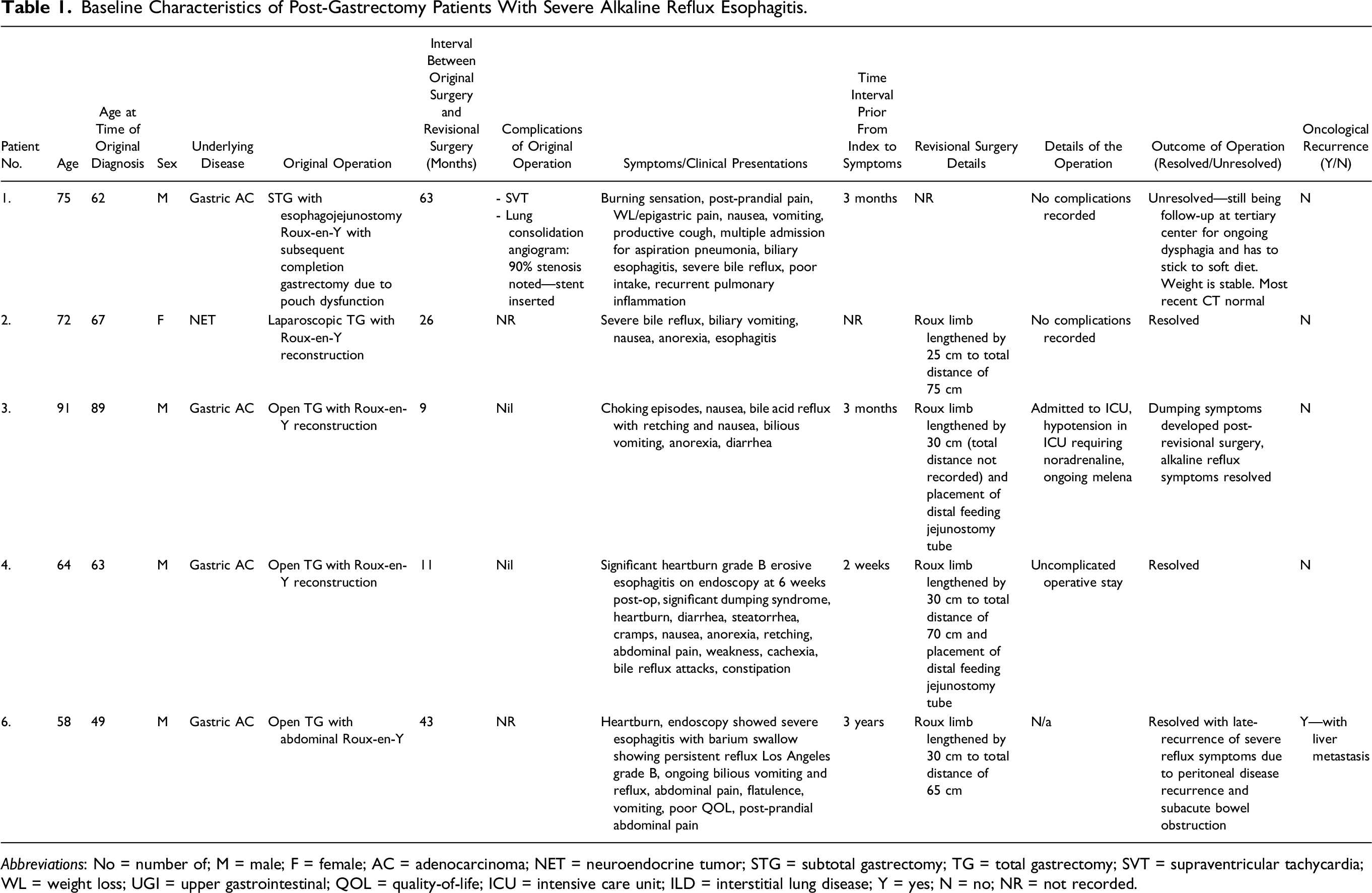
Abbreviations: No = number of; M = male; F = female; AC = adenocarcinoma; NET = neuroendocrine tumor; STG = subtotal gastrectomy; TG = total gastrectomy; SVT = supraventricular tachycardia; WL = weight loss; UGI = upper gastrointestinal; QOL = quality-of-life; ICU = intensive care unit; ILD = interstitial lung disease; Y = yes; N = no; NR = not recorded.
All of these individuals demonstrated a similar clinical picture, which is displayed in Table 1. Endoscopy was the single most important diagnostic study performed alongside serial outpatient appointments with clinical nutritionists at various centers with descriptive documentation of symptomatology, weight, and quality of life scores. Endoscopic findings were mostly consistent across the board, usually consisting of a reddened, oedamatous oesophagus, often with ulcerations/erosions. Endoscopy was also important in eliminating other entities such as marginal ulceration, and stomal, afferent, and efferent loop obstruction. All 5 patients underwent antacid therapy with PPI or sucralfate or both.
Operative Success and Post-Revisional Reflux Symptoms
Overall, 4/5 patients were significantly improved from ARO point of view and had improved body weight after revisional surgery. In 4/5 cases, there was drastic improvement of their symptoms post-intervention with dramatic weight gain, near-complete symptom relief, and greatly reduced bile reflux with no further pain, alongside self-reported great improvements in quality of life. In one case, it is documented that there was poor initial resolution with continuous follow-up with the upper gastrointestinal team for ongoing dysphagia with chest pain; however, improvement was seen in the coming months with no esophagitis seen on endoscopy and increasing weight gain. Overall, there was one case where there was a good initial response; however, within 3 months there was some symptom deterioration
Nutritional Findings and Body Weights
Summary of Weight Loss and Weight Regain.
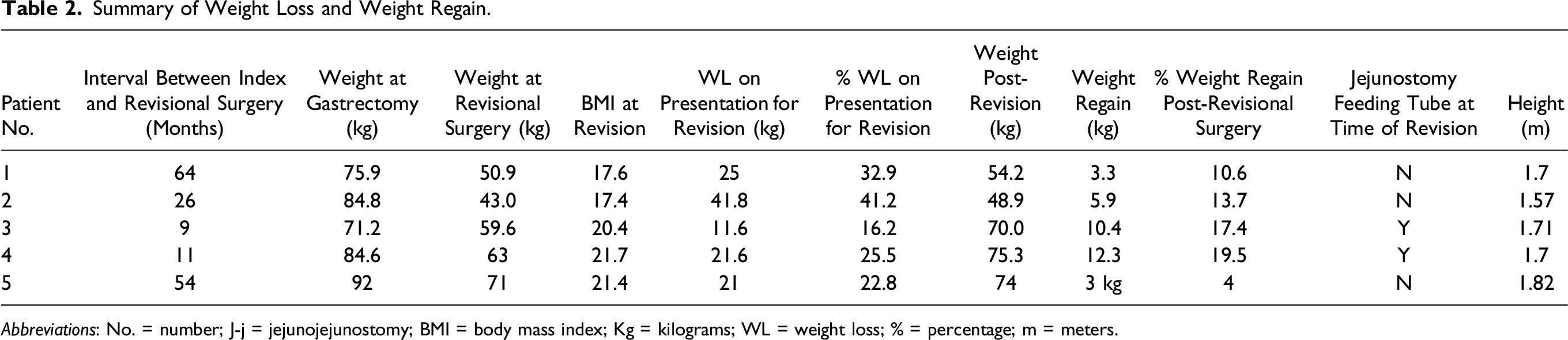
Abbreviations: No. = number; J-j = jejunojejunostomy; BMI = body mass index; Kg = kilograms; WL = weight loss; % = percentage; m = meters.
Discussion
Postoperative alkaline reflux esophagitis is a potentially devastating complication after TG. The advent of the RY reconstruction has significantly decreased the incidence of this complication. However, when reflux esophagitis occurs, it is often refractory to medical treatment. Any intervention that interferes with the mechanism of the pyloric sphincter enables increased reflux of duodenal/jejunal contents into the oesophagus and/or the gastric remnant. 3 Management of reflux can be challenging, particularly in the setting of mixed or alkaline reflux. Acid secretions can be readily controlled using proton-pump inhibitors and γ-aminobutyric acid (GABA) agonists, whereas bile salts and pancreatic secretions prove more difficult. 2 Failing medical management, patients with refractory symptoms require surgical reconstruction. 2
There are several possible explanations to demonstrate how duodenal fluid refluxes post-gastrectomy: First, the reconstruction method. In Billroth II method, the duodenal/jejunal fluid passes through the anastomosis. This method has a described incidence of ARO of 50%-60% of cases. 4 Comparatively, the RY method has a described incidence of 10%-30%. 4 Roux-en-Y esophagojejunostomy is widely accepted as the preferred reconstructive procedure and is effective in preventing reflux, maintaining ideal patient weight. 3 Second, the shorter the anastomotic distance, the more likely ARO to occur, and it has been demonstrated with an anastomotic distance of > 40 cm that leads to less ARO. 2 Third, in cases of TG requiring lower esophagectomy, the decrease in LES pressure due to its dissection and the thoracic cavity negative pressure on the esophageal jejunal anastomosis may increase the risk of ARO. 3 Finally, occlusive mechanisms such as disease recurrence or postoperative adhesions or strictures.
The major limitation of our study was the small number of patients we were able to analyze, given that we focused on only one tertiary hospital experience of this complication. This did not allow solid conclusions regarding the incidence of reflux esophagitis after gastrectomy with esophagojejunostomy. Another limitation was that the data was highly heterogenous, qualitative, and descriptive in nature, and therefore, no quantitative conclusions could be drawn.
Conclusion
Severe ARO is a recognized complication of gastric procedures compromising the LES. The authors report our experience of managing this complication following gastrectomy with jejunojejunal anastomosis and Roux limb length revision, with a majority of patients having improvement in, if not complete resolution of, reflux symptoms. However, higher power studies are required to contribute to the growing interest in this disease process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.