
Abstract
For this lecture, I was inspired by Dr. Bryan Richmond’s Southeastern Surgical Congress presidential address, “Finding your own unique place in the house of surgery.” I struggled to find my own place in cancer surgery. The choices available to me and those who came before me enabled the wonderful career I am blessed to enjoy. What I share as part of my own story. My words do not represent those of my institutions or any organizations of which I am privileged to belong.
Keywords
Introduction
I would like to express my gratitude to the Southeastern Surgical Congress for the invitation to speak at these August proceedings. It is humbling to give an address named after such a giant in cancer care as Dr. A. Hamblin Letton. Dr. Letton was the President of the American Cancer Society (ACS), an organization to which he would devote 50 years of volunteer service. The ACS awarded me my first major 5-year grant, which served as a significant impetus for any successes I have had as a surgeon and cancer researcher. Dr. Letton advocated education, research, and community empowerment. According to the Atlanta Journal-Constitution, he was “instrumental in getting the Pap smear accepted by women and their physicians back in the 1950s.” 1 I am particularly grateful to Dr. Bryan Richmond, Bradford Professor and Chair of the West Virginia University Department of Surgery, my friend and colleague on the American Board of Surgery Council, for his presidential invite to meet my fellow surgeons in this beautiful town of Savannah, Georgia.
My words do not represent those of my institutions or any organizations of which I am privileged to belong. I ask forgiveness for any discomfort (or, as my teenagers say, “cringe”) that my anecdotes may engender.
World History
My maternal grandparents (“Popo” and “Yeye”), pictured here on their wedding day in Mainland China, had a strong influence on their children, and on me (Figure 1). My maternal great-great grandfather was the Chinese equivalent of an old-time country doctor, wading through rice paddies to treat patients and taking poultry or whatever people could trade in payment. My grandfather, in contradistinction, was a university-educated surgical resident in Manchuria when he met my grandmother, who was a rare female medical student. They married, but unlike many of her peers and despite the 4 children she bore during her training, my Popo finished her studies and became an obstetrician/gynecologist and family physician (Figure 2). Drs. Kwan Li and Chang En-Shu with wedding guests, Manchuria, China. Four Chinese siblings. Dr. Tseng’s mother Chang Yun-Li (later, Rose Tseng, PhD) second from left.
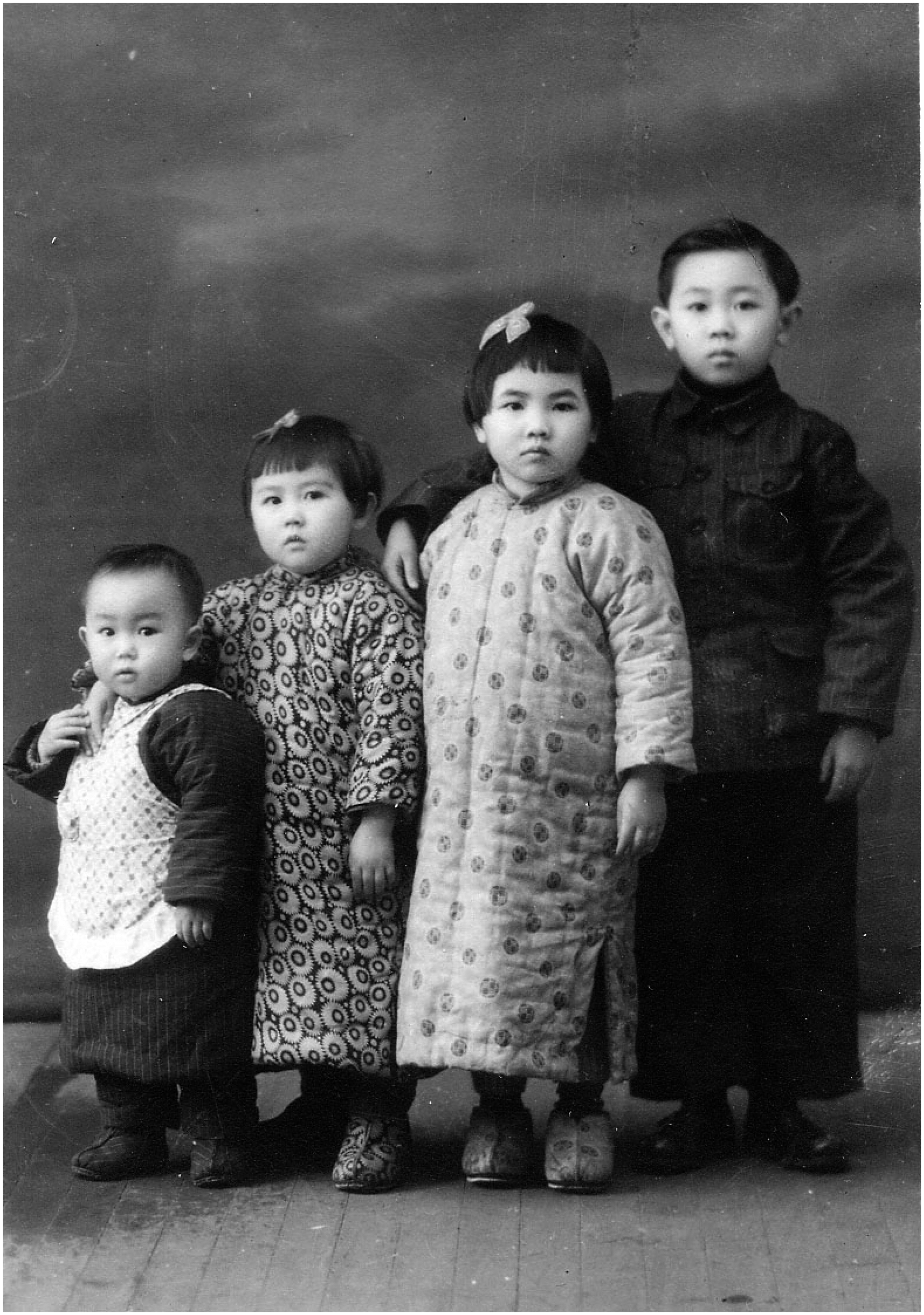
After the Chinese Civil War and the Communist victory, and due to my grandmother’s foresight, my mother’s parents fled with their children to Taiwan in 1949. Of note, my Popo and Yeye were criticized by their peers for waiting longer for 6 tickets, instead of taking only their sons. Meanwhile, in Southern China, my paternal grandparents also fled the Communists, except they left their daughter behind in Hainan and brought only their 2 sons through Macau, Hong Kong, and eventually to Taiwan. This agonizing choice haunted my paternal grandmother (“Nai-nai”) to her dying day. They were never reunited, although I did later meet my Aunt once in China with my father, afterward.
In Taiwan, my maternal grandfather, Dr. Chang, was a general surgeon and, after training at City of Hope, a thoracic surgeon at both National Taiwan University Hospital and the military hospital in Taipei. My grandmother Dr. Kwan ran a clinic and ambulatory surgery center adjacent to their house, and my grandfather Dr. Chang would perform private practice surgery on nights and weekends, with her assisting him. My mother would be sent to deliver prescriptions and messages after class, still in her schoolgirl uniform.
Coming to America
My parents, who did not know each other in Taiwan, attended university there but longed for greater opportunities in the United States. Initially, they were prohibited by the Chinese Exclusion Act of 1882 and its revisions, resulting in the 1924 Johnson-Reed Act, the U.S. system that limited immigrants from each country to 2% of their “nationality,” as reported by the 1890 U.S. Census but completely excluded Asians (Johnson-Reed Act
2
). This “National Origins” system was finally put to rest in the mid-1960s,
3
opening the way for immigrants like my parents to pursue their American dreams. After visiting my grandparents in Ethiopia, who were by then working there for the World Health Organization, my mother went to Kansas State to study chemistry because they offered her a scholarship; my father went to the University of Colorado and received a master’s degree in aeronautical engineering. My mother longed to follow in her parents’ footsteps and practice medicine, but as a foreigner she was unable to obtain loans or scholarships for medical school, so she made do with a PhD in nutrition from the University of California, Berkeley. There, Chang Yun-li, restyled Rose Chang, met my father Tseng Chi-Jen, AKA “Raymond,” who was working on his doctorate in mechanical engineering. After they wed, I arrived 2 years later. As a child, I was always tickled that the month on my mother’s PhD diploma was the same as that of my birth. I knew even then that she must be a very efficient woman (Figure 3). Doctors Tseng with baby Jennifer on PhD graduation day, University of California, Berkeley, 1969 (close readers of the text, please note that Dr. Rose [Chang] Tseng’s degree was officially conferred September 1968).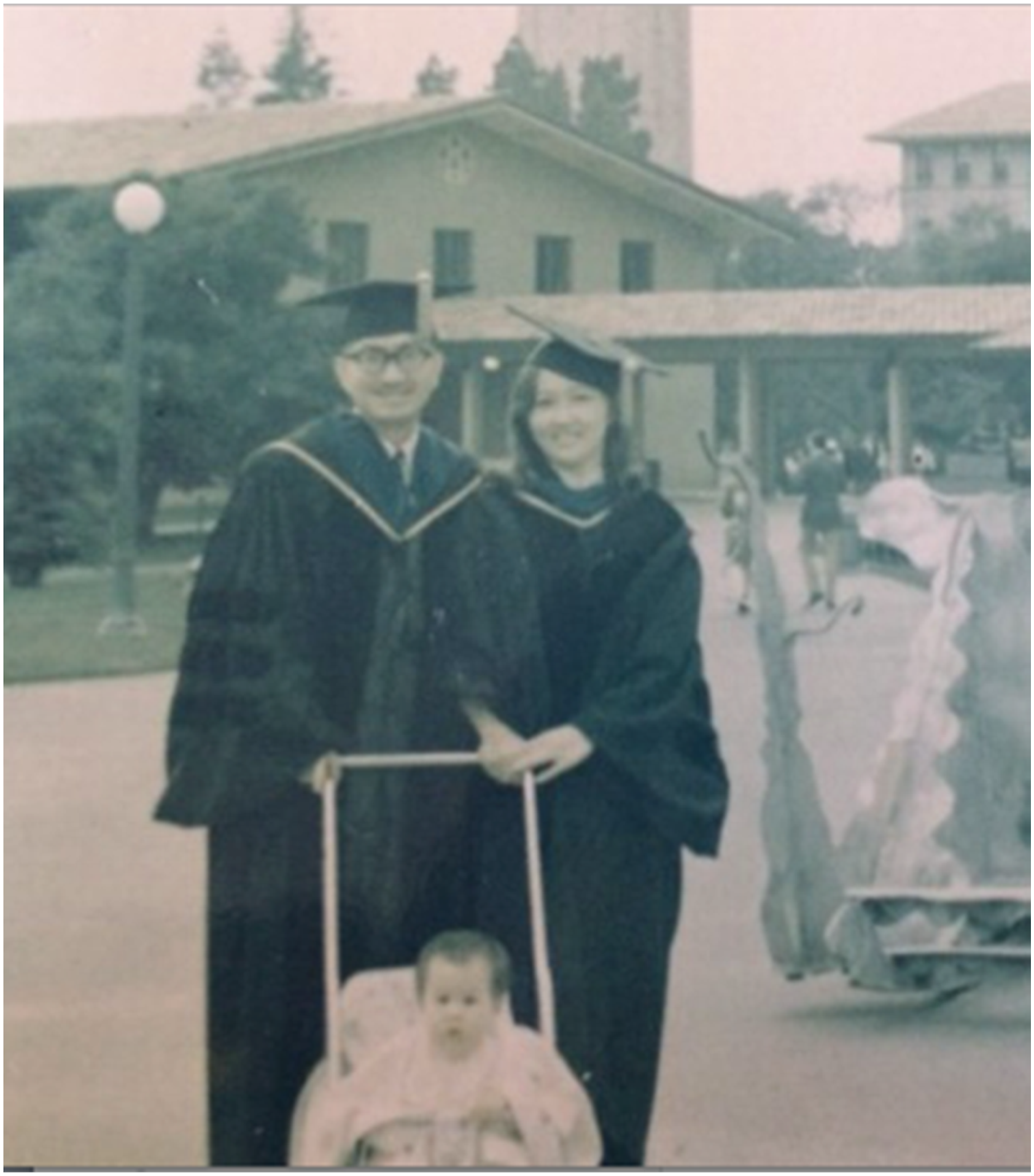
I wanted to be a doctor ever since I can remember. Honestly, the only thing I ever wanted more was to be a mother. I went to public schools in San Jose, California, and then earned degrees in biology and English at Stanford, but my desire to excise cancer dates from the University of California School of Medicine in San Francisco. In my preclinical years, I took a fascinating seminar on the molecular biology of cancer with faculty that included Nobel winners Mike Bishop and Harold Varmus, as well as Bruce Alberts 4 of Molecular Biology of the Cell fame. But at the same time, my beloved maternal grandparents, who had moved to the U.S. decades earlier to retrain and practice medicine, were in crisis. My grandfather had bilateral adenocarcinomas diagnosed in his lungs. I was struck by both the unwillingness of his 4 highly educated children to discuss hospice, palliative care, or even the true nature of his diagnosis with him, and his profound focus during his final illness on us, his grandchildren, and our future. His last spoken words to me were, “You need to go into a subspecialty. You will not be satisfied in primary care” (I had committed the unforced error early on in medical school of telling him that I was drawn to primary care women’s health or OB-GYN). Of course, my grandfather was right about me.
Much to my shock, in my third year, I fell in love with surgery. I did transplant with Nancy Ascher and John Roberts, Gold Surgery with Ted Schrock and TK Hunt, and a trauma subinternship with Bill Schechter and Peggy Knudson, and Marco Patti as a chief resident. Resistance was futile. I went with Sean Mulvihill as a fourth-year sub-I to break the news after laparoscopy to a pancreatic cancer patient that he had metastatic disease. I was infuriated that there was “nothing we could do,” and I resolved to do something. My closest female friends in medical school, all superior students to me, told me they were not choosing surgery because I want to have a family. I remember having an argument with my mother, who went directly from tiger mom forbidding me to date to “Where are my grandchildren?” trying to talk me into either pediatrics or ophthalmology as a career. At the end, she tried, “I watched you very closely. You were NOT that good with your hands as a child. Your piano teacher said so.” She also laid the guilt on, despairing, “Why do you always have to do the hardest thing?”
I ended up at Massachusetts General Hospital (MGH) for surgery residency. I think perhaps it was because I had nervously mentioned during the infamous grilling that passed for an interview at the time, that my grandfather performed the first closed mitral commissurotomy in Taiwan. Apparently, Gordon Scannell was on my panel and had performed the first one at MGH. I dislike the term imposter syndrome, but upon arrival, I surely felt like a fish out of water. My fellow interns were superb, and to me, intimidating, including one born at MGH and raised at Harvard and another whose ancestor cofounded the hospital. 5 My only flat shoes were Birkenstocks, I didn’t own a winter coat; I had barely heard of the American Football Conference (who are these so-called Patriots?); and I didn’t understand why anyone would need separate football and baseball stadiums when one Candlestick Park would do.
Go East, Young Woman
I confess, I went East in part for a man. And I will say, there is fault on both sides, but it did take the gentleman awhile to get around to proposing. There were some obstacles. We were from opposite backgrounds and coasts, were registered in different political parties, and held divergent views on privacy and as to whether one should hire house cleaners (I was pro). He was raised Roman Catholic, and while my mother was baptized by missionaries in high school in Taiwan, my parents thought my brother and I should choose for ourselves. He was indifferent to football, of either college or professional varieties, disliked outdoor activity unless it involved a beach or pool, and had no idea what March Madness was. Worst of all, the man rooted for the New York Yankees.
As we know in cancer surgery, with enough effort and neoadjuvant pre-treatment, miracles do happen. I conceded I would seek a job in Massachusetts; he agreed to biweekly house cleaning, skiing vacations, and Asian in-laws in occasional residence; and I spent 6 months in intensive study with a Jesuit priest and was baptized as a Catholic on Pope John Paul II’s 80th birthday. 6
By the time we were married on Labor Day weekend, I was in my third and last year of research with Drs. Richard Mulligan, Judah Folkman, and others, working on pancreatic cancer vaccines. I had decided on a career in surgical oncology, preferably of the upper gastrointestinal variety, with clinical, research, and teaching being equally important to me. I also was eager at the age of 31 to get started with my lifelong dream of being a mother. I proposed to my new spouse that we embark on this journey immediately. My husband has a faux-bro “New York” sense of humor and said, “Well, I’m Italian, so of course we’ll get pregnant on our honeymoon. When are you going back to residency?” When I told him July 1, 2001, he did the calendar math and laid down the law. He would not be the primary caregiver of the proposed infant while I returned to surgery residency as a PGY4. He said, “I would have to call DSS on myself!” So, we delayed.
When it became time for me to apply for fellowship to fulfill my goal of being a cancer surgeon, the conflict between my chosen career and my family aspirations was in full flower. I applied to only a few programs; my reasoning was that if I was going to leave my immovable spouse for 2 years it would need to be for extremely good reason (of note, this was in 2002; there is so much more parity and diversity in surgical oncology programs today, and I would choose differently if doing it over). I was incredibly fortunate to match at the University of Texas MD Anderson Cancer Center in Houston, where I have family and I could fulfill my secret aspirations to work with Doug Evans, Peter Pisters, Jeff Lee, and others.
Houston, Texas
I started fellowship at MD Anderson in July 2003, at the age of 34¾ (but who’s counting). My husband and I agreed we would fly out every other weekend to see each other. It was wonderful for 2 people with demanding jobs not yet blessed by children to work all week as hard as we needed to without guilt and then on weekends to go on actual dates and spend quality time with each other as a couple. I gloried in helping with breast, melanoma/sarcoma, colorectal, hepato-pancreato-biliary cases, and helping patients live their lives. Six months before fellowship ended, we finally reached agreement on the possibility of parenthood, and lo and behold, we conceived a highly desired pregnancy, with the estimated day of confinement of mid-November 2005.
Advisory: I share some medical details of my pregnancy below. Please jump ahead to the next section, if you prefer.
I concealed my pregnancy from everyone around me during my fellowship except my program director. Again, I would make a different choice today. The year before, a pregnant fellow experienced preterm labor and required bedrest, and I heard a fair amount of complaining from some male fellows—all fathers themselves — about covering for her. I resolved not to make my pregnancy an item of discussion unless it needed to be. It never was. I never missed a day of work during fellowship because of my pregnancy.
I planned my first OB visit at 10 weeks’ gestation to coincide with my one week of Boston vacation. On the way to George Bush International Airport, I had an event in the car. Upon making it through security, I was certain that I had miscarried and made my way to the restroom and called my spouse. At my insistence, he used his privilege to reach my scheduled OB at Brigham and Women’s Hospital, where they both worked. With the reluctant acceptance of husband and MD, I somehow made my way onto the plane and flew frantically to Boston.
I had an urgent ultrasound at Brigham and Women’s, after which the OB ultrasound MD told me that our long-desired fetus was implanted so close to the cervix that in conjunction with a previously unknown 14-centimeter fibroid at the fundus, this was functionally a cervical pregnancy that would not come to term, would be life-threatening to me, and would need to be terminated. This was devastating news. My husband was terrified for my health, was ready to proceed with this recommendation immediately, and tried to comfort me with his faux-bro humor, “I worked very hard to select the best mother of my children, and I need to her to be alive to be able to allow my genes to continue in this world.” I did not find this funny. At my request, he also used his privilege to get me a next-day private practice appointment with the brilliant Dr. Beryl Benaceraf, the founder of genetic ultrasonography, who happened to be married to my husband’s boss. Beryl repeated the imaging herself and told us that while there certainly was a heightened risk for fetal demise and maternal complication, including potential emergent hysterectomy and even fatal hemorrhage for me, there was some chance of viability to term, and that with careful monitoring, we could make the calculated choice of “wait and see.”
With extreme anxiety on the part of my husband, and less on mine—surgeons are optimists—I went back to Houston and finished my training in advanced surgical oncology. My cousin Charlotte, who worked in gynecologic oncology at MD Anderson, found a wonderful, high-risk OB-GYN at St. Luke’s Hospital, a courtly Southerner with a bowtie and a drawl, who let me sprint unscheduled across the Texas Medical Center into his office like a mad person between cases once a week to assess the fetus and me. This picture is of our graduation, with my fellow complex general surgical oncology fellows and me in the front row (Figure 4). From left to right, the graduating fellows are seated, and the general surgical oncology fellows are from left to right, Tom Aloia, John Mullen, me, Keith Delman, Todd Bauer, and Tim Pawlik. The 2 other women in the front row were the 1-year breast fellows, Nazanin Khakpour and Roshni Rao. No one knew of my pregnancy then, except for Steve Curley, in the hat, although Keith’s wife, Dana Meaney-Delman, an OB-GYN, became suspicious that very graduation night. The University of Texas MD Anderson Cancer Center Surgical Oncology Fellowship Graduation 2005.
I can say with 100% certainty that if the current United States and Texas laws were in place, my husband would never have let me go back to finish my fellowship, and my career would have been very different.
Tex-Mass
During all these, I was scheming to get a job at Boston University (BU)/Boston Medical Center (BMC). My thrilling clinical time in Texas had made it clear to me that I wanted a career in upper GI surgical oncology, with complex, challenging cases. While I had a longstanding interest in basic science and pancreatic tumor immunology, at MD Anderson for the first time I was privileged to take care of a diverse patient population and witness and investigate disparities in care.
I hope Dr. Letton would be proud of my first paper from MD Anderson, which elucidated different rates of immediate reconstruction for breast cancer based on race and helped MD Anderson develop protocols to make sure all patients are offered appropriate options for care. 7 At BU and BMC I interviewed multiple times, including in my current office, with the then-chair of surgery, only to be ghosted. Luckily, I had the great good fortune to get a position at UMass Memorial Medical Center in Worcester. While I had no start-up package and it required an hour-long drive each way (even without traffic or Nor’easter), my department and my chiefs and partners and residents formed such a supportive community I was able to start a pancreas program and a research group, Surgical Outcomes Analysis & Research (SOAR), which led me to obtaining independent funding like aforementioned American Cancer Society grant. More importantly, I was able to achieve my lifelong dream of being a mother.
In this 2006 photo in Worcester, Mass., here I am with former first fetus and current 17-year-old, with a host of cancer-fighting colleagues at the UMass Walk for Cancer (Figure 5). Pictured are surgeons, medical oncologists, nurses, secretaries, family, friends, and more. The purple on our shirts is for pancreatic cancer, one of the most lethal, and the message is “hope.” To me, this shows it takes a village to treat and beat cancer. The UMass Walk for Cancer 2006.
After I pushed my son’s stroller across the finish line and made it home from Worcester, here he was (Figure 6). Clearly, he’s not making a political statement! He’s trying to decide which ball to throw at Mom, but to me, it represents all the choices we make, in cancer surgery and also along our way. The next year we were joined by his little sister, who was born after a thoroughly uneventful pregnancy and is pictured here with me and my resident Dr. Melissa Murphy, with her son and her sister in Chicago in 2009 (Figure 7). We were all there to attend the annual meeting of the Society for Surgery of the Alimentary Tract (SSAT). I have the honor of being the current president of the SSAT. Organizations like SSAT and the Southeastern Surgical Congress are vital to fostering the careers of surgeons at every step of the way.
8
Back home after the UMass Walk for Cancer 2006. Surgeons and family members in Chicago between presentations at the Society for Surgery of the Alimentary Tract, 2009.

BU and BMC
Finally, more than a decade after failing to get hired at BU and BMC as a new fellowship graduate, I was hired as the Utley Professor and Chair of Surgery at Boston University and the Surgeon-in-Chief at Boston Medical Center. As institutions and in my department, we focus on health equity from research, educational, and clinical aspects. We have a BMC Health Equity Accelerator, which aims to provide “Exceptional Care without Exception” and to promulgate best practices wherever they are needed. Our next chapter is entitled “Rewriting Health Care,” and I look forward to leading our department of surgery in that worthy endeavor.
As you now know, I am not a native New Englander. But in my decades on the East Coast, I have learned something of history. The words of John Winthrop, preacher and colony leader, resonate. They have been used by politicians from Kennedy to Reagan and beyond, but to me, they represent health care.
“We shall be as a city on a hill. The eyes of the world are upon us.”
We are all faced with difficult choices, even in positions as privileged as I have generally found myself. The journey to a lifetime career in cancer care is no exception, and I for one, feel that we should enable those around us to make their choices as best they can, whether they be patients, trainees, or colleagues.
Lastly, here is a picture of why we do what we do, at work (Figure 8). This is a dear patient I have known for 2 decades who had pancreatic cancer, and after an aborted Whipple and double bypass at another hospital in the Northeast was told he was incurable and advised to get palliative chemotherapy and get his affairs in order. He sought an opinion from my mentor Doug Evans, and on his advice had neoadjuvant chemo and radiotherapy in Massachusetts, and returned to Houston for his reoperative pancreaticoduodenectomy with vascular resection while I was a trainee. This photo was three years ago just before COVID at Boston Medical Center; last year, he walked his daughter down the aisle as a 20-year survivor of pancreatic cancer. He and his wife want you all to know that they are profoundly grateful for what surgeons, and all doctors and caregivers on our complex multidisciplinary teams, do for patients every day. A long-time patient and 20-year pancreatic cancer survivor and spouse at Boston Medical Center, 2019.
What a privilege we have as surgeons to participate in our patients’ cancer journeys. I am grateful to President Richmond for the kind invitation, to the Southeastern Surgical Congress for the privilege of the floor, and for your generosity in hearing me out. It is my life’s blessing to be the mother of my 2 children, and an enormous privilege to be a cancer surgeon. I am so grateful for all the opportunities and the choices I have had along the way.
Footnotes
Acknowledgments
The editorial expertise of Patricia Cleary is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.