
Abstract
Introduction
Victims of violence (VoV) are at disproportionate risk for future violence, making consideration of patient safety by Emergency Medicine (EM) physicians and Trauma Surgeons (TS) essential when discharge planning (DP) for VoV. Practice patterns and ethical perspectives in DP for VoV, and their respective scenario- and specialty-specific variations, are unknown.
Methods
We surveyed 118 EM and 37 TS physicians at a level 1 trauma center. Three clinical scenarios were presented (intimate partner violence, elder abuse, gun violence), each followed by four questions assessing practices and ethical dilemmas in DP. Responses were compared using Chi-Square testing.
Results
Response rate was 51.6%. EM physicians more frequently supported patient autonomy to proceed with a potentially unsafe discharge plan after an episode of Intimate Partner Violence (P = .013) and believed that admission could facilitate change in the victim’s social situation after an episode of Elder Abuse (P = .026). TS physicians were more likely to offer social admission, providing additional time to navigate safe discharge planning (P = .003), less likely to see social admission as an inappropriate use of limited resources (P = .030) and less likely to support patient autonomy to proceed with a potentially unsafe discharge (P = .003) after gun-related violence.
Conclusion
There appears to exist scenario- and specialty-specific variability in the practice patterns and ethical perspectives of EM and TS physicians when discharge planning for victims of violence. These findings highlight the need for further evaluation of specific factors underlying variability by situation and specialty, and their implications for patient-centered outcomes.
• Victims of violence are at disproportionate risk for future episodes of violence. To avert future harm, post-discharge safety necessitates careful consideration after episodes of violence. • There are intriguing differences in provider approaches to safe discharge planning for victims of elder abuse, intimate partner violence and gun violence scenarios, worthy of broad reflection. • Empirical research on the ethics of safe discharge planning after violence is scarce and provider guidance is limited. Further research and ethical deliberation is necessary to guide safe discharge planning after violence.Key Takeaways
Introduction
There exists a subset of patients who present to emergency departments (ED) with traumatic injuries who are victims of repeated trauma. Within this group, those most affected are victims of violence 1 (VoV), including victims of gun violence, intimate partner violence (IPV), elder maltreatment or any other type of violence inflicted by another person. Unfortunately, the rates of violent reinjury are high, 2 with nearly 40% of VoV seeking care for violent reinjury within 2 years of discharge. 3 Further, injury severity appears to progressively increase with each episode of violence, particularly with IPV and firearm violence.2,4,5 In a recent study evaluating IPV specifically, of victims who went on to die from violent injuries, up to 75% had presented for medical evaluation of violent injuries at least once prior to being killed. 6 In their Code of Medical Ethics opinion 8.10, the American Medical Association (AMA) calls upon physicians to “take appropriate action to avert the harms caused by violence and abuse” and posits that physicians hold a duty to treat the symptoms of violence while simultaneously working to mitigate its long term-consequences. 7 Collectively, this underscores the need to consider the potential for violent reinjury and to actively work to avert the its harms, every time a victim seeks medical care for violent injuries.
Emergency medicine (EM) and trauma surgery (TS) physicians frequently interact with VoV and invariably face situations where their patients are medically stable for discharge but have concerns for own their safety if they were to return to the environment in which they were victimized. It is here where careful disposition planning considering the risk of violent revictimization after discharge, and incorporating multidisciplinary perspectives, is most important. Occasionally, admission to the hospital, or “social admission,” with the sole purpose of buying more time to navigate a safe discharge plan may be necessary. It is in these situations where potential for ethical conflict arises, including concerns of resource utilization, patient autonomy and patient safety.
Aside from the AMA’s commentary on prevention, identification and treatment of violence, little has been done to delineate frameworks for navigating disposition planning for VoV without safe environments to return to, or to empirically characterize the ethical dilemmas faced therein. We aimed to characterize the ethical dilemmas faced, and the variations in practice patterns and perspectives that exist, when making disposition plans for medically stable victims of violence. Secondarily, we aimed to characterize differences in the approaches of Emergency and Trauma physicians, two key stakeholders in the care of violently injured patients, to these ethically complex situations.
Methods
The Vanderbilt University IRB deemed this research exempt (IRB #211145). Using a qualitative exploratory approach, 4 TS and 3 EM attending physicians were invited to voluntarily participate in semi-structured interviews. 6/7 physicians (85.7%) consented to an interview. All interviews occurred between November and December 2021. Interviews were conducted, recorded, transcribed, and coded by one researcher (MW) using an interview guide designed in conjunction with a trauma surgeon, emergency medicine physician, and bioethicist.
Emergent interview themes were abstracted, and assessed in a broader population using 33-question Likert scale survey (Strongly Agree, Somewhat Agree, Somewhat Disagree and Strongly Disagree). 155 EM attending and resident (PGY 1-3) physicians, TS attending and fellow physicians, and senior (PGY 4-5) general surgery residents at a single academic level 1 trauma center were surveyed, based upon their intimate involvement in trauma patient disposition planning. Voluntary invitations were sent by email, with a gift card raffle as a response incentive. All surveys were completed between January and March 2022. Survey data were collected and managed using REDCap electronic data capture tools.8,9
Survey Scenarios and Questions.
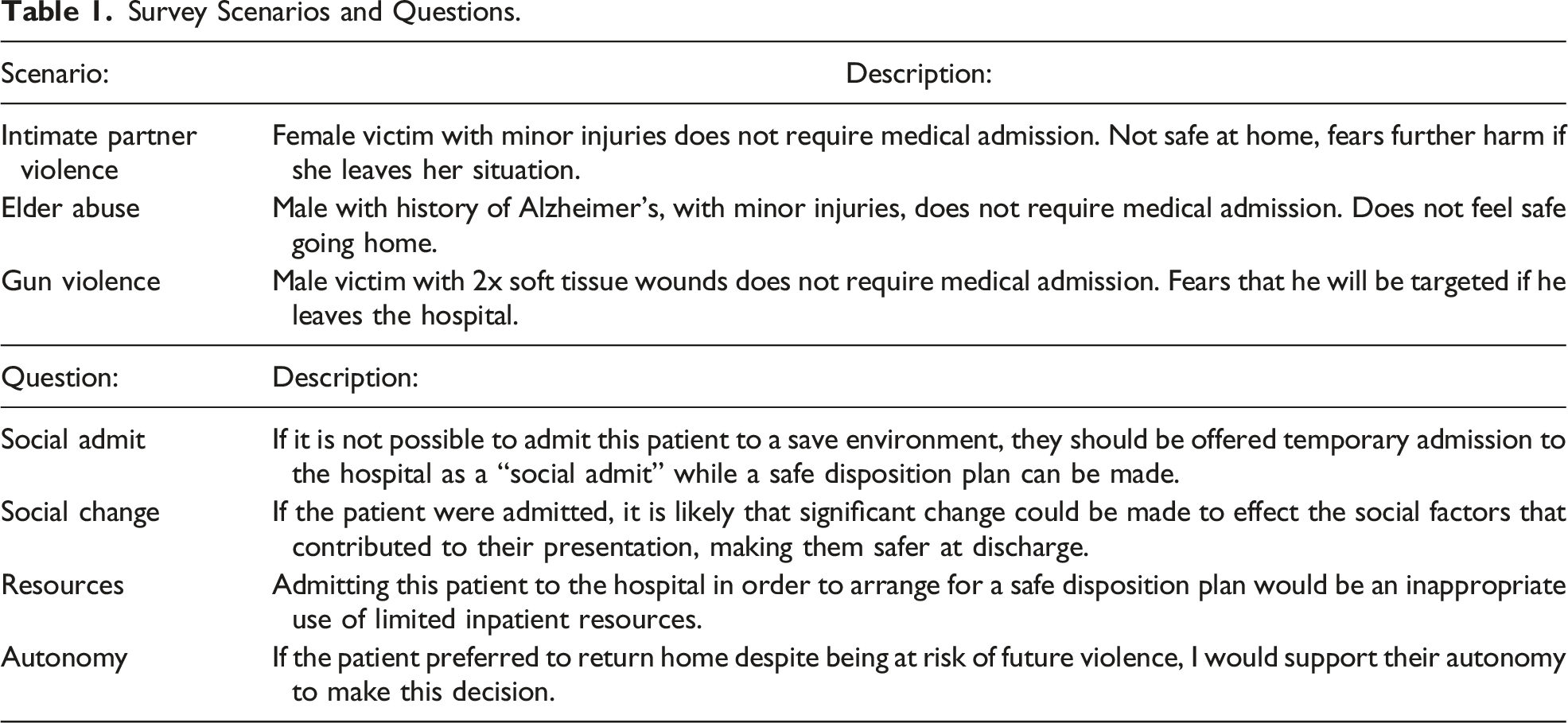
Data were analyzed to: (1) describe the overall physician responses to each question and scenario set to identify core differences in physician responses to each, and (2) describe the differences between EM and TS responses to each scenario and question set. Specialty-level results were analyzed by comparing EM and TS physicians, in which EM resident and attending physicians were grouped as “Emergency Medicine,” and TS fellow and attending physicians, as well as general surgery residents were grouped as “Trauma Surgery.” The 2-group t test was used to test numeric variables whereas the chi-squared (𝜒2) test was performed on categorical variables. Analyses were performed in R version 4.2.0. 10 All P-values set a priori at < .05 were considered statistically significant.
Results
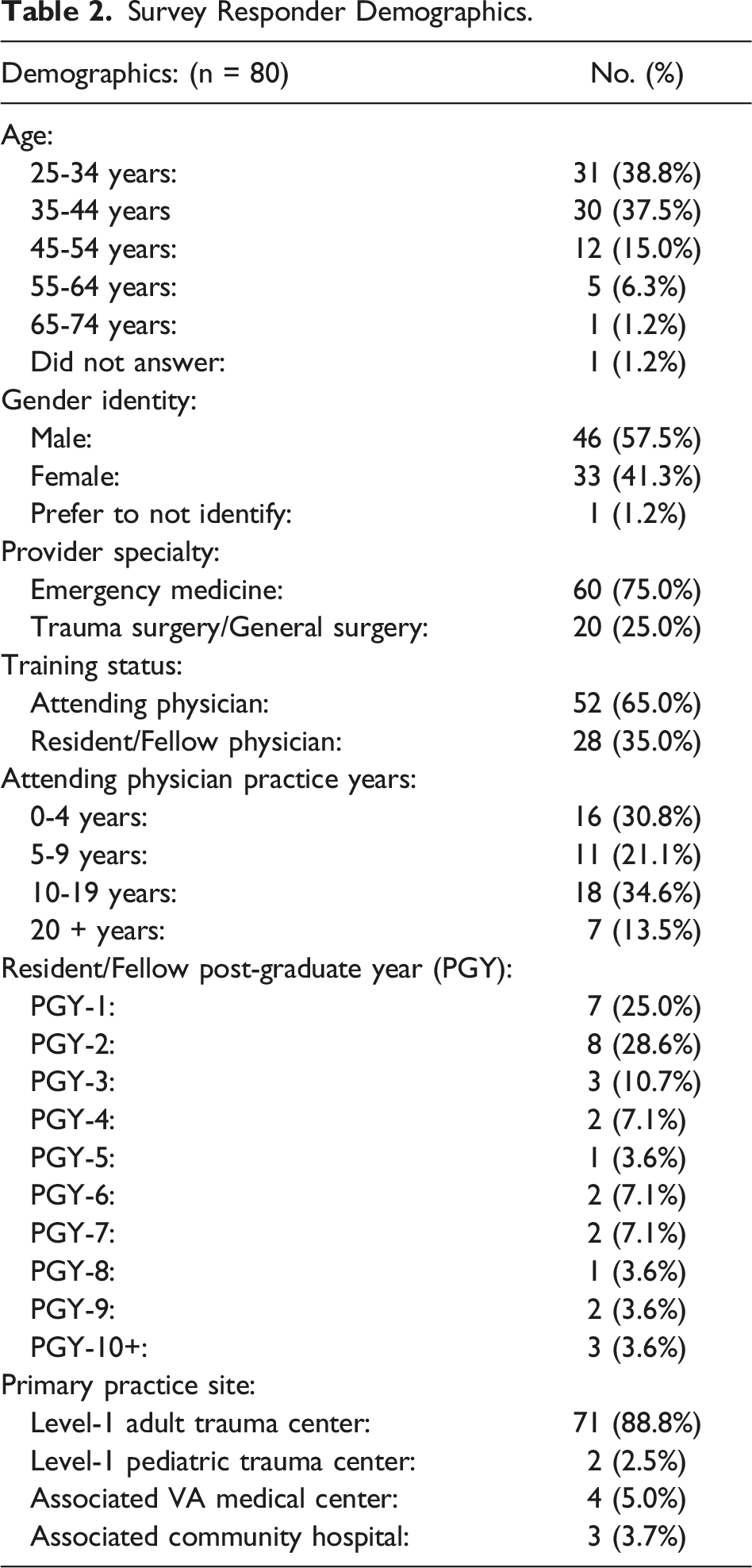
We received 80 responses (51.6% response rate). Most responders were male (57.5%). Of responders, 60 (75%) were EM and 20 (25.0%) TS physicians, consistent with their relative quantities at our institution. In total, 28 (35%) responders were attending physicians, while 52 (65%) were resident or fellow physicians. Of the 80 responders, 73 (91.3%) primarily practice at our adult or pediatric level 1 trauma centers, with 7 (8.7%) primarily at our associated VA medical center or community hospitals. (Table 2)
In the social admit question we observed that physicians were most likely to believe that social admission was appropriate in the Elder Abuse scenario (75.0% strongly agree, 22.5% somewhat agree) as compared to the IPV (57.5% strongly agree, 33.8% somewhat agree) and Gun Violence scenarios (18.8% strongly agree, 48.8% somewhat agree) (P < .01, Figure 1). For our social change question, physicians were most likely to believe that social admission could affect positive change in the patient’s social circumstances in the Elder Abuse scenario (27.5% strongly agree, 55.0% somewhat agree) as compared to the IPV (6.3% strongly agree, 52.5% somewhat agree) and Gun Violence (2.5% strongly agree, 18.8% somewhat agree) scenarios (P < .01, Figure 1). For our autonomy question, physicians were most likely to support a patient’s autonomy to knowingly return to a potentially unsafe situation in the Gun Violence (57.5% strongly agree, 35.0% somewhat agree) and IPV (43.8% strongly agree, 48.8% somewhat agree) scenarios as compared to the Elder Abuse (8.8% strongly agree, 32.5% somewhat agree) scenario (P < .01, Figure 1). Finally, for our resources question, physicians were least likely to view social admission as an inappropriate use of limited resources in the Elder Abuse scenario (53.8% strongly disagree, 37.5% somewhat disagree) as compared to the IPV (38.75% strongly disagree, 42.5% somewhat disagree) and Gun Violence (15.0% strongly disagree, 51.3% somewhat disagree) scenarios (P < .01, Figure 1). Descriptive analysis of aggregate responses to each question, per scenario. There are statistically significant variations between mean responses to each question across the three clinical scenarios (P < .01).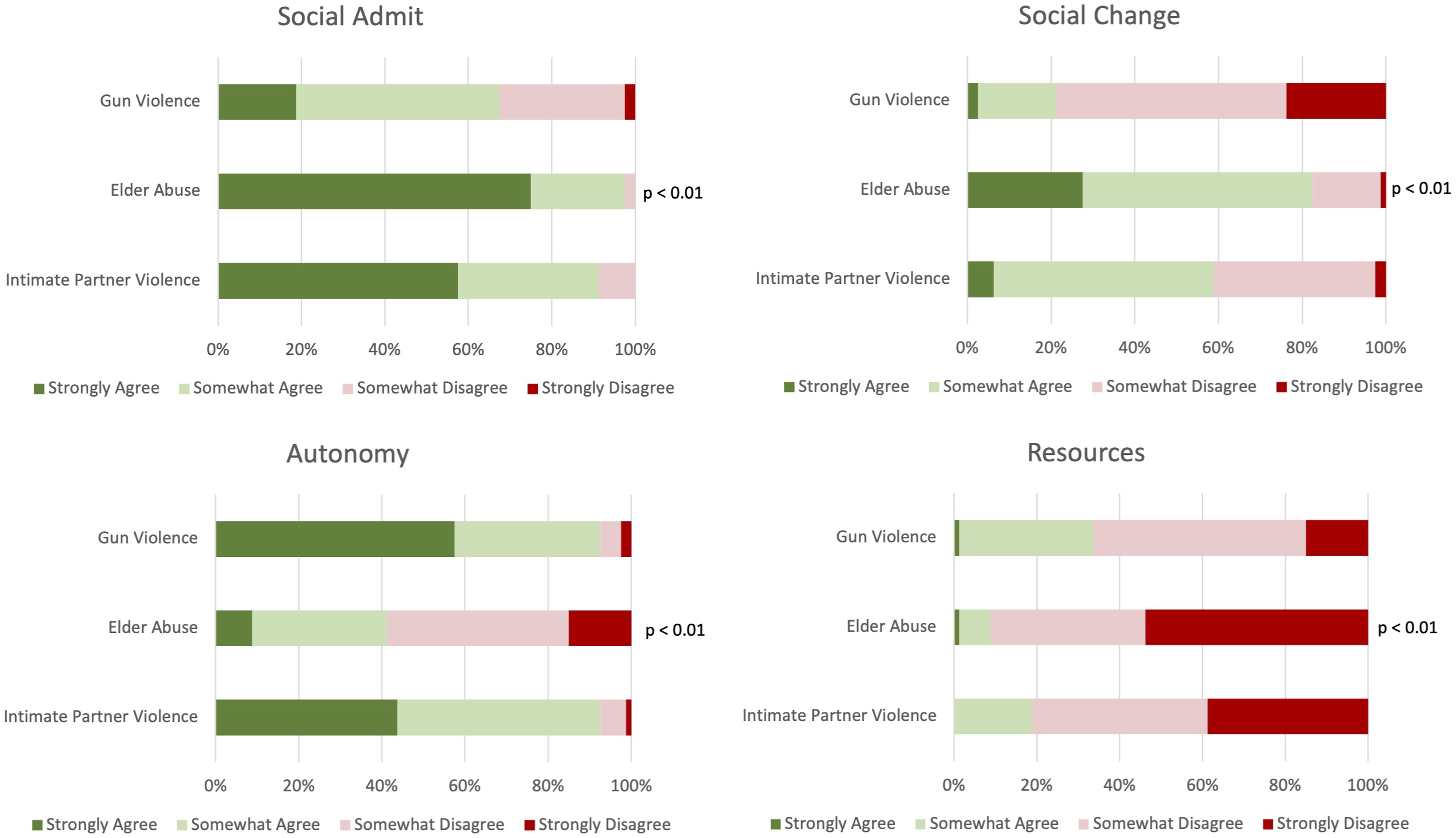
We observed that TS were more likely than EM physicians to believe that social admission was appropriate in the Gun Violence scenario (TS: 45.0% strongly agree, 45.0% somewhat agree, EM: 10.0% strongly agree, 50.0% somewhat agree, P = .003, Figure 2). For the social change question, EM physicians were more likely than TS to believe that social admission could effect positive change in the patient’s social circumstances in the Elder Abuse scenario (TS: 10.0% strongly agree, 55.0% somewhat agree, EM: 33.3% strongly agree, 55.0% somewhat agree, P = .028). For the autonomy questions, EM physicians were more likely than TS to support a patient’s autonomy to knowingly return to a potentially unsafe situation in the Gun Violence (TS: 25.0% strongly agree, 55.0% somewhat agree, EM: 68.3% strongly agree, 28.3% somewhat agree, P = .003) and IPV (TS: 25.0% strongly agree, 55.0% somewhat agree, EM: 50.0% strongly agree, 46.7% somewhat agree, P = .013) scenarios. Finally, for our resources question, EM physicians were more likely than TS to disagree with social admission being an appropriate use of limited hospital resources in the Gun Violence scenario (TS: 35.0% strongly disagree, 45.0% somewhat disagree, EM: 8.3% strongly disagree, 53.3% somewhat disagree, P = .03). Descriptive analysis of aggregate responses to each question, per scenario, between Emergency Medicine (EM) and Trauma (TS) physicians. In the gun violence scenario, there are significant differences for all questions except Social Change. For the Elder Abuse scenario, there are significant differences for the social change and for the Intimate Partner Violence scenario, there are significant differences in the Autonomy.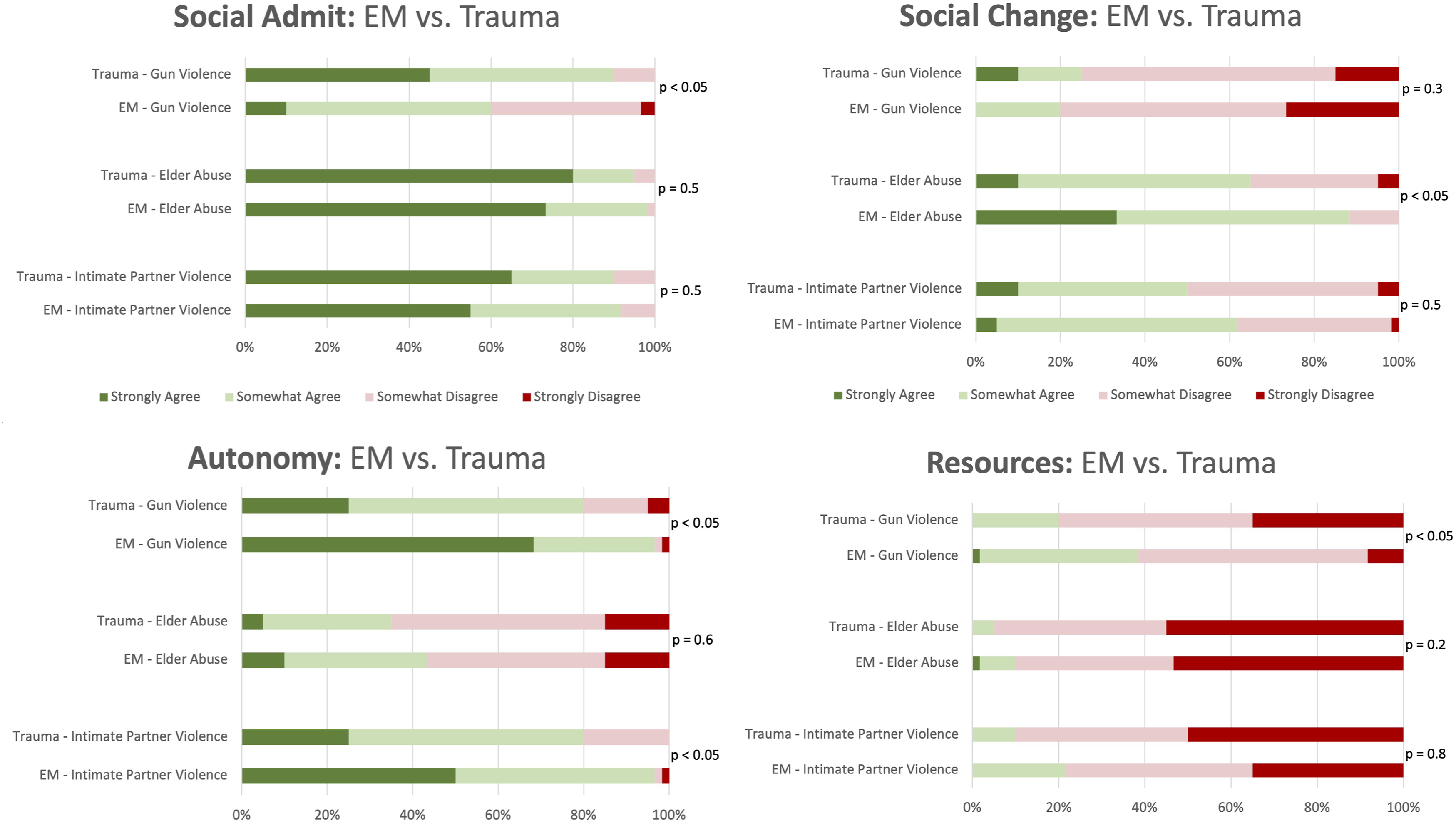
Discussion
Survey Responder Demographics.
We report four important overall trends (Figure 1): First, physicians were most likely to believe that social admission was an appropriate intervention in Elder Abuse, as compared to IPV and Gun Violence scenarios. Similarly, physicians were most likely to believe that social admission could affect positive change in their patient’s social circumstances in a Elder Abuse scenarios. Third, physicians were most likely to support a patient’s autonomy to knowingly return to a potentially unsafe situation in Gun Violence and IPV scenarios. Finally, physicians were least likely to view social admission as an inappropriate use of resources after Elder Abuse. Collectively these results appear to suggest a perceived responsibility to avert further harm in these populations with a concurrent perception of intractability associated with Intimate Partner and Gun Violence as compared to Elder Abuse, potentially limiting physician comfort in their abilities to intervene. It may similarly be the case that physicians perceive Elder Abuse victims as being more vulnerable, less capable of altering their own social circumstances or less likely to have decision making capacity, collectively making them more worthy of scarce hospital resources.
We further analyzed response variability between EM and TS physicians (Figure 2). First, TS physicians were more likely to believe that social admission was appropriate in the Gun Violence scenario. Next, EM physicians were more likely to believe that social admission could affect positive change in the patient’s social circumstances in the Elder Abuse scenario. EM physicians were more likely to support a patient’s autonomy to knowingly return to a potentially unsafe situation in the Gun Violence and IPV scenarios. Finally, EM physicians were less likely to believe that social admission was an appropriate use of limited hospital resources in the Gun Violence scenario. These data are important, because depending on each incident’s unique situational factors and each institution’s unique practice patterns, disposition planning for violently injured patients may be driven by either EM or TS physicians, or both. Collectively, we hypothesize that these differences represent differences resource availability and in the primary responsibilities of these physicians. With increasingly high ED censuses, emergency physicians are increasingly forced to make disposition decisions with limited inpatient resources available to draw upon. TS physicians, alternatively, primarily care for injured patients in an inpatient setting. This may lead to a difference in resource allocation and disposition decisions between the two specialties, as EM physicians may rely on alternative resources (social work, case management, etc.) to provide appropriate resources for VoV patients while preserving an available bed for another ED patient. Alternatively, TS physicians already caring for inpatients may have access to, and incorporate, more resource intensive inpatient services into disposition planning, and in turn seek to effect social change in the patients’ situations, leading to more emphasis placed on social admission and the ability to effect social change. Finally, due to their inherently limited involvement in inpatient care, EM physicians may have limited exposure to the potential benefits of social admission for victims of VoV, limiting their perceived utility of such interventions. Ultimately, the nature of these interspecialty differences is unknown and future studies should seek to explore these findings further and clarify their nature and existence.
Despite these scenario- and specialty-specific variations, these data collectively suggest that consistent with AMA Medical Ethics opinion 8 × 107, the surveyed physicians felt some responsibility to avert future harm in VoV, and in some situations, would consider temporary admission to address the consequences of potential repeated exposure to harm. The scenario-level response variation, however, does highlight the inherent difficulty of applying 1 potential solution, such as social admission, to diverse and nuanced clinical scenarios. While social admission may be more feasible, and pose more potential benefit, in a victim of elder abuse, it may be less feasible for a victim of IPV who feels responsible to return to the situation in which they were injured to continue providing care for dependents, for example. These variations are not inherently inconsistent with AMA opinion 8.10; rather, they underscore the need for incorporation of a broad repertoire of multidisciplinary harm-reducing safe discharge planning solutions in nuanced clinical scenarios. It is not lost on the authors, however, that survey question 4 which evaluated the physician’s willingness to support a patient’s wish to return to a potentially unsafe situation, conflicts with opinion 8.10s assertion that physicians must always work to avert further violence. This conflict between obligations to protect patients while simultaneously preserving their right to choose their own destiny, highlights the tension that can arise between autonomy and beneficence in principalist medical ethics. The apparent emphasis on autonomy seen in these data is consistent with the broader trend toward affording relative primacy to patient autonomy in American medical ethics, 11 introduced in Beauchamp and Childress’ landmark text “Principles of Biomedical Ethics.” 12 Accordingly, if a VoV has decision making capacity and desires to return to an unsafe situation, despite the risk of harm, it may be argued that it is most appropriate to honor their desire to do so. Going forward, resources should be devoted to broadly implementing evidence-based harm-reduction strategies in the safe discharge planning of VoV. To do so, however, further discussion and empirical research are both needed to further elucidate the ethical implications of safe discharge planning for VoV and to create consensus ethical frameworks to guide clinicians through the invariable complexities of discharge planning for this vulnerable patient population.
We highlight three key study limitations. First, this is a single center study, limiting its generalizability to the EM and TS physicians at our institution. However, with a response rate of 51.6% (80 respondents), encompassing both EM and TS attending and trainee physicians, the core themes are at least broadly hypothesis-generating. Second, by using a survey-based study with fixed scenarios and questions, which may not fully encompass the variety of nuanced ethical scenarios that present in victims of violence, our ability to generalize these results to novel situations may be limited. Finally, effective safe discharge planning should draw upon diverse perspectives and resources from stakeholders such as physicians, nurses, social workers, bioethicists and community partners. As this study only surveyed physicians, its conclusions may not fully represent the diverse perspectives of the entire discharge planning team.
Footnotes
Acknowledgements
Christopher Lindsell PhD, Paul Juarez PhD, Keith Meador MD, Laura Beskow PhD, Joseph Fanning PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work described was supported by CTSA award No. UL1 TR002243 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.