
Abstract
Background
Hemorrhaging trauma patients may be disproportionately affected by choice of induction agent during rapid sequence intubation (RSI). Etomidate, ketamine, and propofol are safe in the trauma population-at-large but have not been assessed in patients with ongoing hemorrhage. We hypothesize that in hemorrhaging patients with penetrating injury, propofol deleteriously affects peri-induction hypotension compared to etomidate and ketamine.
Methods
Retrospective cohort study. Primary outcome was the effect of induction agent on peri-induction systolic blood pressure. Secondary outcomes were the incidence of peri-induction vasopressor use and quantity of peri-induction blood transfusion requirements. Linear multivariate regression modeling assessed the effect of induction agent on the variables of interest.
Results
169 patients were included, 146 received propofol and 23 received etomidate or ketamine. Univariate analysis revealed no difference in peri-induction systolic blood pressure (P = .53), peri-induction vasopressor administration (P = .62), or transfusion requirements within the first hour after induction (PRBC P = .24, FFP P = .19, PLT P = .29). Choice of RSI agent did not independently predict peri-induction systolic blood pressure or blood product administration. Rather, only presenting shock index independently predicted peri-induction hypotension.
Conclusions
This is the first study to directly assess the peri-induction effects of anesthetic induction agent choice in penetrating trauma patients undergoing emergent hemorrhage control surgery. Propofol does not appear to worsen peri-induction hypotension regardless of dose. Patient physiology is most predictive of peri-induction hypotension.
Key Takeaways
• In adult penetrating trauma patients requiring intubation for emergent operative hemorrhage control, propofol does not appear to worsen peri-induction hypotension, regardless of dose. • Underscoring the importance of efficient resuscitation and operative hemorrhage control, patient presenting physiology, not choice of induction agent, is most predictive of peri-induction hypotension or requiring transfusions.
Background
Rapid sequence intubation (RSI) is a critical event in the care of the injured patient and involves a complex interplay between procedural proficiency, patient physiology, injury burden, and medication effect. Due to the time-sensitive and physiologically tenuous nature of care for acutely injured trauma patients, significant work has been done evaluating the impact of induction agent choice on patient outcomes during RSI.1-7 Patients in hemorrhagic shock represent an extreme example of those requiring swift interventions and most impacted by induction agent choice. Therefore, within these patients, the pharmacological profile of any induction agent needs to be weighed against patient physiology, the potentiation of hypotension, and worsening hemorrhagic shock.
Etomidate, ketamine, and propofol are the three most popular induction agents, and their use is predicated on varying physiological effects. Etomidate, once the most common induction agent in trauma due to its notable hemodynamic stability, has been shown to cause adrenal insufficiency and is associated with increased rates of Acute Respiratory Distress Syndrome and Multiple Organ Dysfunction Syndrome.8,9 Propofol, often used for its rapid onset and short duration of action, is a potent cardiac depressant and significantly reduces systemic vascular tone, increasing the risk of peri-induction hypotension.2,10 Ketamine, conversely, is heavily favored for its hemodynamic and respiratory stability but has yet to gain widespread hold as the sole induction agent of choice in trauma for its perceived risk of increasing intracranial pressure. 1
Numerous studies have demonstrated the safety and efficacy of all 3 agents for RSI in the acutely injured, but these studies are mired by analysis of heterogenous patient populations with varying injury patterns and hemodynamic derangements.3-6 Reductions in systemic vascular tone and cardiac output may disproportionately affect acutely hemorrhaging patients; therefore, understanding the consequences of induction agent choice is vital. 11 Nevertheless, the wealth of available literature does not adequately address the effect of induction agent choice in hemorrhaging patients. This study assesses the effect of induction agent choice on peri-induction vital signs and resuscitation efforts in trauma patients with active hemorrhage requiring emergent operative intervention. Given its pharmacological profile, we hypothesize that propofol causes significant peri-induction hypotension in hemorrhaging patients, given its vasodilatory and cardio-depressant effects compared to etomidate and ketamine.
Methods
Following approval from the Institutional Review Board (IRB), we performed a retrospective chart review of all trauma patients undergoing emergent operative intervention for management of penetrating injury over a three-year period (2017-2020) at a level I academic trauma center. Patients were included in the study if they (1) had a penetrating injury (ie, stab or gunshot wound), (2) proceeded directly from the emergency department (ED) to the operating room for hemorrhage control procedures, and (3) were intubated in the operating room by an anesthesia provider. We employed the need for an emergent hemorrhage control procedure following penetrating injury as a surrogate marker for the presence of active hemorrhage and/or hemorrhagic shock. Patients were excluded if they were intubated without an anesthetic agent or required resuscitative thoracotomy or resuscitative endovascular balloon occlusion of the aorta (REBOA) catheter deployment in the ED. We focused on penetrating trauma patients to minimize the inclusion of patients with non-hemorrhagic causes of shock (often seen in blunt trauma), which may contribute to their presenting physiology. We only examined patients who were intubated in the operating room because many patients intubated in the trauma bay (1) did not require a hemorrhage control operation and (2) the frequency of peri-induction vital signs recorded in the patient chart was much greater in the operating room than in the trauma bay, making it effectively impossible to compare across the groups. Our analysis evaluated those who received propofol induction against those who received a non-propofol agent (limited to ketamine or etomidate). We focused on 3 domains depending on the phase of care, including (1) presenting characteristics, including patient demographics, presenting injury characteristics, triage information and ED resuscitation, (2) peri-induction variables, including vital signs, resuscitation, intubation, and anesthesia data, and (3) operative resuscitation. To standardize the maintenance anesthetics of isoflurane and sevoflurane, the inhaled anesthetic exposure was quantized as the average exhalational minimum alveolar concentration (MAC) in hours (MAC-hours). The effects of isoflurane or sevoflurane were not differentiated since their reductions in systemic vascular resistance are similar.
Peri-induction variables focused on vital signs and resuscitation measures in the time immediately preceding and following administration of an induction agent. Only vital signs within the first 10 min following induction agent administration were recorded. This time denomination was chosen specifically as the hemodynamic effects of the RSI agent would be most likely to manifest in this timeframe. 12 Vital signs were recorded in the electronic medical record (EMR) automatically and in real time and were subsequently abstracted retrospectively from the EMR. Recorded blood pressures were either from an arterial line or blood pressure cuff, though arterial line recordings were preferentially recorded, if present. Peri-induction hypotension was defined as one or more recorded systolic blood pressures less than 90 mmHg. Peri-induction vasopressor support was defined as vasopressors administered in the 10 min immediately preceding and following induction, to account for any pre-induction medication for anticipated hemodynamic derangements. Peri-induction blood product and crystalloid resuscitation was defined as intravenous fluid administration or blood component transfusion in the first 60 min following induction, to account for all possible delays in blood product transfusion associated with obtaining blood from the blood bank.
Our primary outcome was the effect of the choice of induction agent on peri-induction systolic blood pressure. Secondary outcomes include the incidence of intra-operative vasopressor use and the amount of post-induction resuscitation required within the first hour of an operation measured in individuate blood products administered.
Data were analyzed according to their normality in the form of mean and standard deviation as well as median with 25th and 75th percentiles. Normality was assessed using the evaluation of skewness and Kurtosis. Student’s T-test and Chi-square test, or Fischer’s exact test, were used where appropriate for normally distributed variables. The Mann-Whitney U Test was used for nonparametric variables. Multivariate regression modeling with risk adjustment was performed to identify independent predictors of change in blood pressure. Specifically, to assess the effect of propofol dosage on changes in peri-induction systolic blood pressure, a linear multivariate regression was conducted with variable entry into the model using significant univariate associations and purposeful selection. Additionally, we wanted to assess the effect of propofol on the incidence of peri-induction hypotension as it is possible that increasing propofol dosage may influence peri-induction systolic blood pressure that is statistically meaningful but clinical irrelevant. To assess whether propofol increased the odds of peri-induction hypotension, a multivariate logistic regression was performed on patients who received propofol through to identify significant predictors of hypotension. B coefficients and Odds Ratios were reported for linear and logistic regressions, respectively, as well as 95% confidence intervals. A P-value of greater than .05 was considered significant. Data analysis was performed using JASP Team (2020, Version .14.1). Study methods were confirmed to be in accordance with the STROBE observational study checklist.
Results
Two hundred fifty-five patients with penetrating injuries who underwent operative hemorrhage control were identified for analysis. Eighty-six patients were excluded—12 patients who did not receive any induction agent, 32 patients who received a combination of induction agents, and 42 patients who underwent a procedure for reasons other than for hemorrhage control (eg, orthopedic, urologic procedure, and ophthalmologic). One hundred sixty-nine patients were included, with 146 patients in the propofol group and 23 in the non-propofol group (Figure 1). Summary flowchart demonstrating inclusion and exclusion criteria used. 255 patients were identified, 169 met inclusion criteria. In total, 146 patients received propofol and 23 received a non-propofol induction agent (etomidate or ketamine).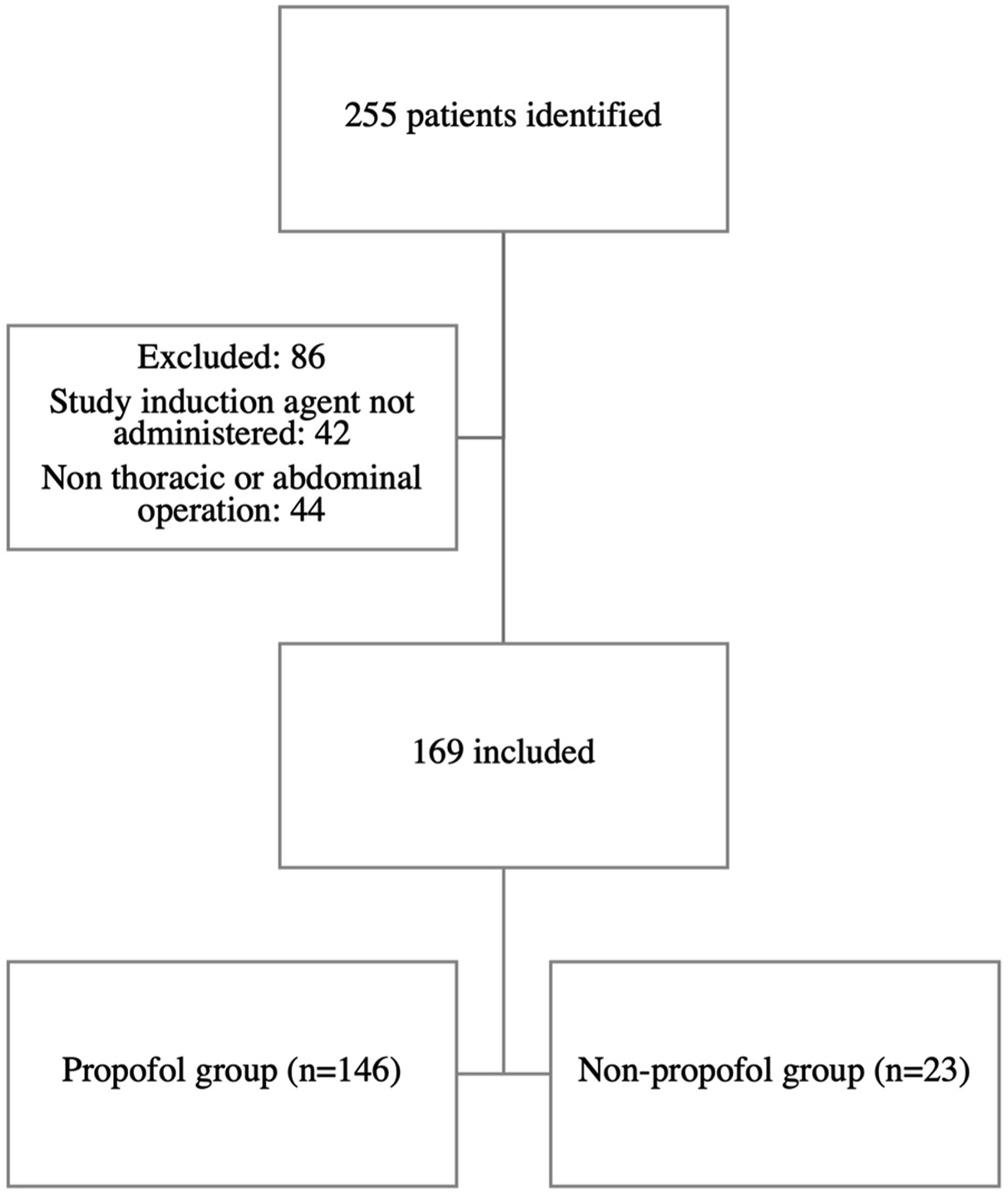
Baseline Demographics and Anesthesia.
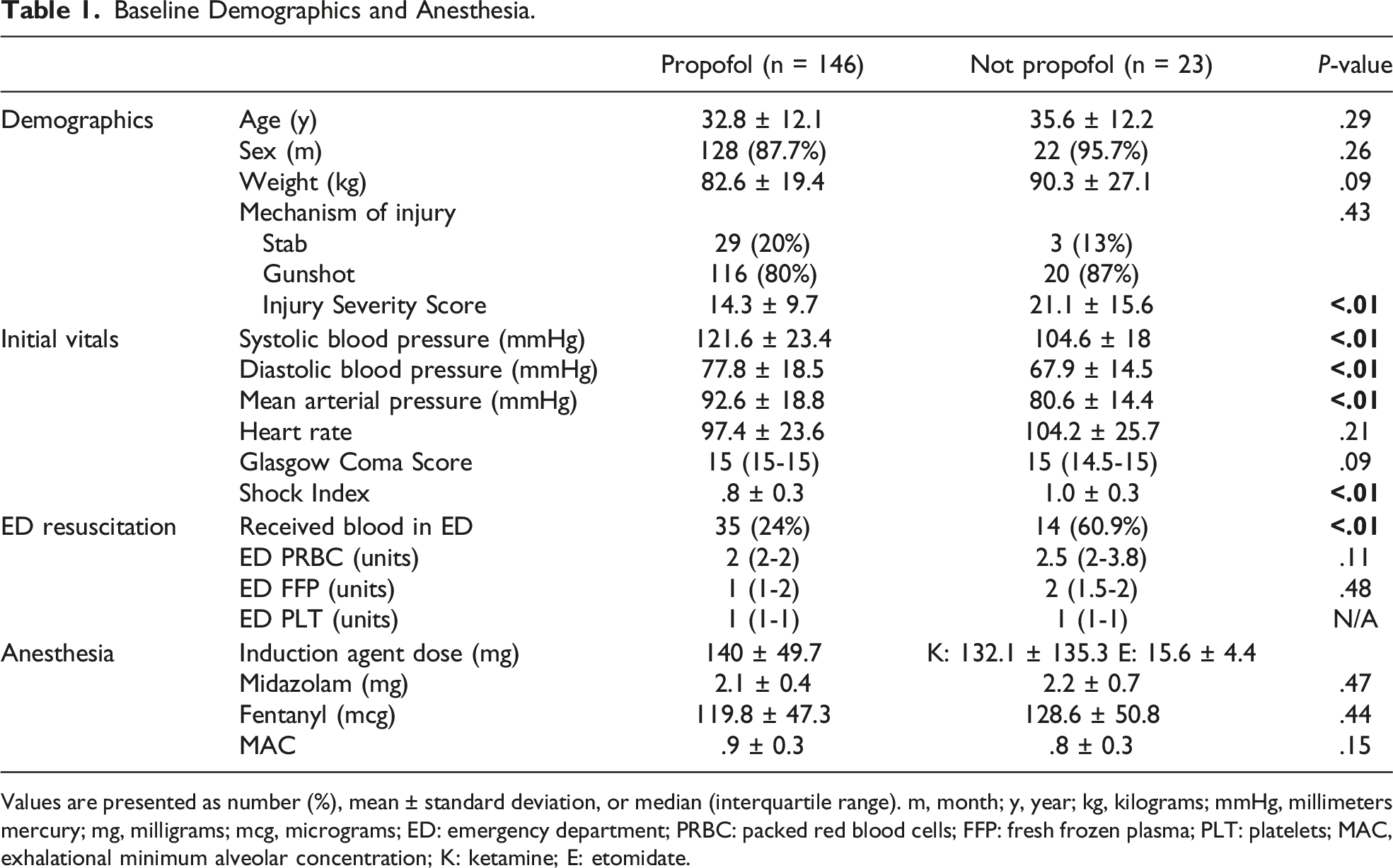
Values are presented as number (%), mean ± standard deviation, or median (interquartile range). m, month; y, year; kg, kilograms; mmHg, millimeters mercury; mg, milligrams; mcg, micrograms; ED: emergency department; PRBC: packed red blood cells; FFP: fresh frozen plasma; PLT: platelets; MAC, exhalational minimum alveolar concentration; K: ketamine; E: etomidate.
Operative Information.
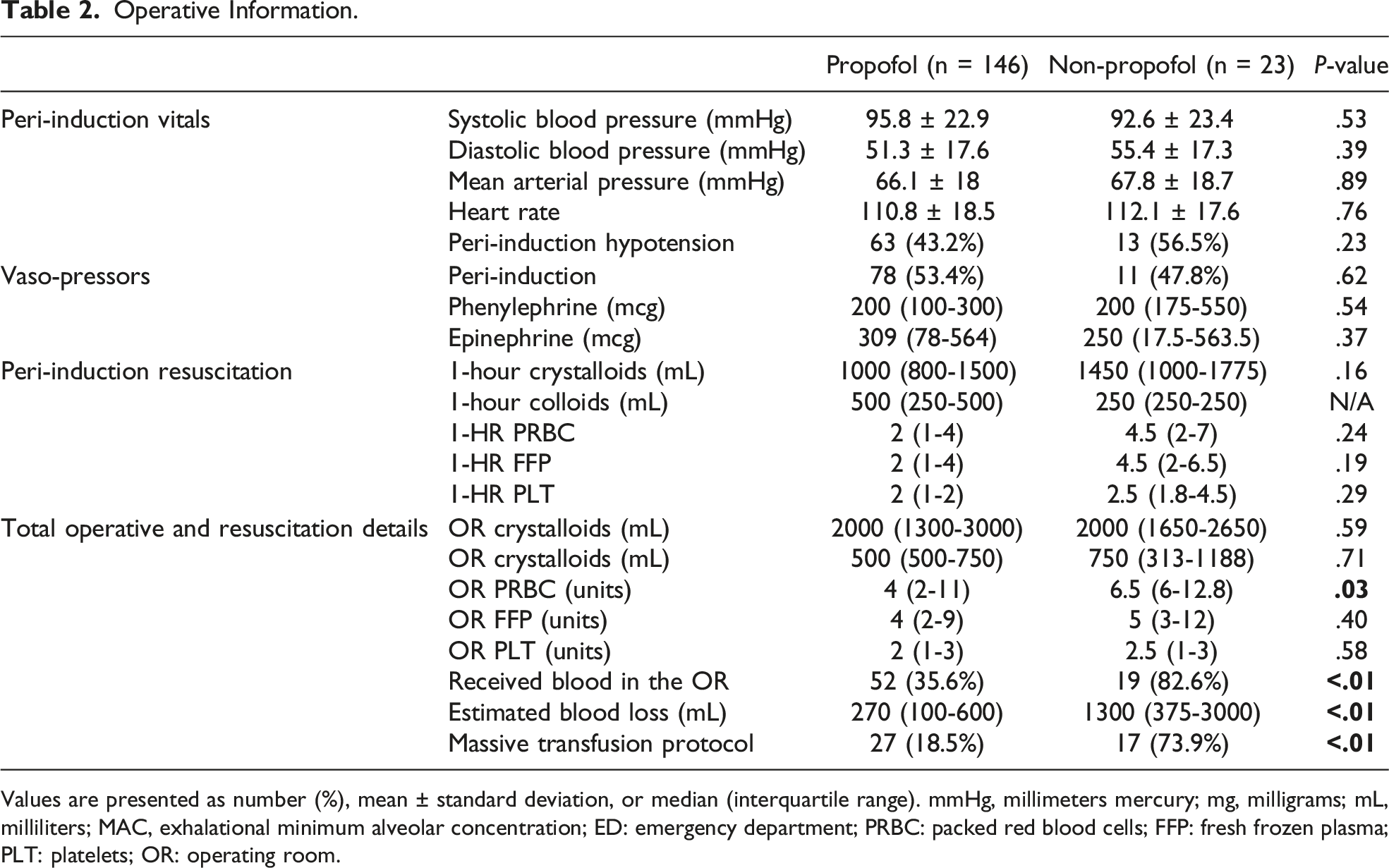
Values are presented as number (%), mean ± standard deviation, or median (interquartile range). mmHg, millimeters mercury; mg, milligrams; mL, milliliters; MAC, exhalational minimum alveolar concentration; ED: emergency department; PRBC: packed red blood cells; FFP: fresh frozen plasma; PLT: platelets; OR: operating room.
Multivariate linear regression predicting change in peri-induction systolic blood pressure.
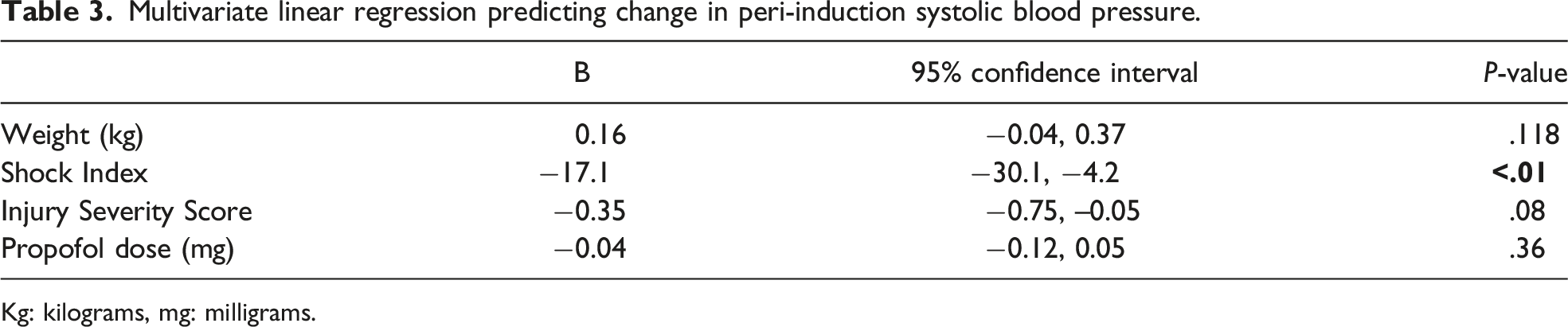
Kg: kilograms, mg: milligrams.
Multivariate logistic regression predicting peri-induction hypotension in the OR for patients receiving propofol.
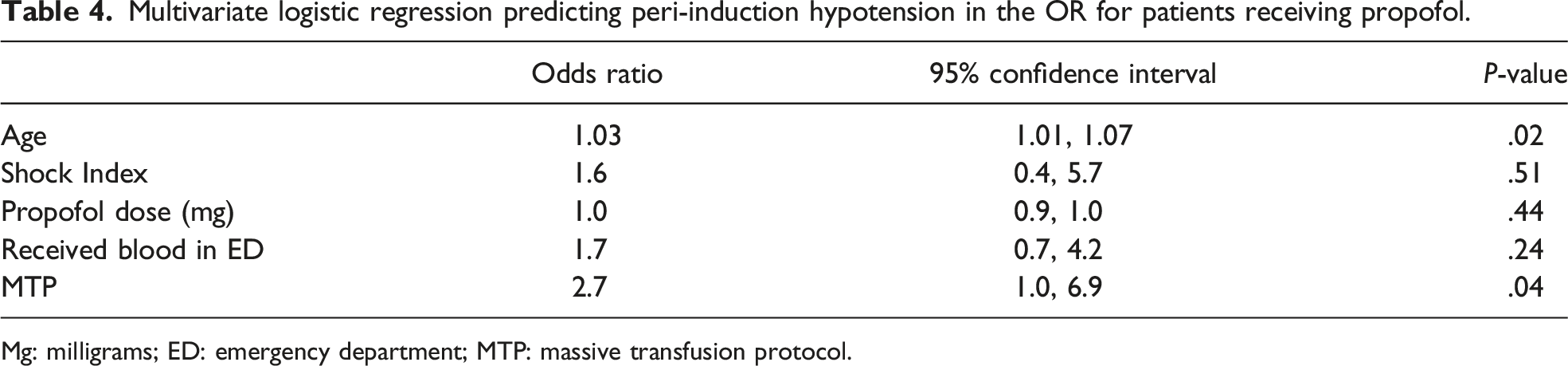
Mg: milligrams; ED: emergency department; MTP: massive transfusion protocol.
Discussion
This study assessed the effect of different RSI agents on peri-induction vital signs in acutely hemorrhaging trauma patients. We hypothesized that the choice of induction agent would have a clinically significant impact on the incidence of peri-induction hypotension and specifically that propofol would be the worst offender. The assumptions underlying our hypothesis lie in the vasodilatory and cardio-depressant effects of propofol compared to etomidate and ketamine and the sensitivity within hemorrhaging patients to reductions in systemic vascular resistance and cardiac output.1,2,10,11 Our findings do not support this hypothesis. Rather, we found that hemorrhaging trauma patients who underwent RSI with propofol did not incur more peri-induction hypotension than patients who received either etomidate or ketamine. This aligns with previously published literature on the topic, demonstrating the overall safety of propofol for RSI in trauma patients.3,7 To our knowledge, this is the first study to focus on the interaction between RSI agent choice and its effect on patient physiology in the setting of acute hemorrhage. The management of hemorrhaging patients comprises a balance of high-risk and high-stakes interventions with little margin for error to maximize survival and minimize morbidity.13,14 Therefore, findings that induction agent choice does not appear to worsen hemodynamic derangement are important and impactful for any patient undergoing RSI regardless of location.
The demographics of patients in our study varied between those who received propofol vs ketamine or etomidate and were notable for non-propofol patients having higher injury severity scores, lower initial systolic blood pressure, and a higher initial shock index. We investigated the effect of propofol on our peri-induction outcomes by controlling for these differences using multivariate linear regression. Initial shock index was the only significant predictor of change in peri-induction systolic blood pressure. Conversely, propofol administration and injury severity were not significant predictors of peri-induction hypotension. The reasons for these findings are likely multitudinous. On the one hand, we surmise that our study evaluated victims of penetrating injury to which the injury severity score may not accurately reflect injury severity or potentiation of hemodynamic aberrancy. This phenomenon has been well described.15,16 On the other hand, we assumed that propofol-related hypotension might be dose-independent in hemorrhaging patients, given their reliance on increased systemic vascular resistance and cardiac output. Our findings do not support this and receiving propofol does not necessarily precipitate hypotension. Prior work has suggested that there may be a dose-dependent effect of propofol with peri-induction hypotension in elective surgical populations.17,18 To test whether the dose of propofol affected our primary outcome, we performed a multivariate linear regression on propofol dose as well as injury severity and shock index. We found that the dose of propofol did not correlate with changes in peri-induction blood pressure or blood administration. This suggests a distinct physiologic milieu in hemorrhaging trauma patients for which elective surgical data may not apply.
We evaluated peri-operative resuscitation, including vasopressors and blood component therapy, to assess whether RSI agents altered resuscitation practices. Vasopressor use and blood component therapy were not significantly different in the peri-induction period between groups, indicating the vasodilatory effects of propofol may not be as pronounced in hemorrhage. More specifically, push-dose vasopressor use of phenylephrine and epinephrine were similar between groups in the peri-induction period, and there were no differences in blood product use in the peri-induction period. Non-propofol patients did receive more blood products overall, including massive transfusion, which is likely reflective of their higher ISS, shock index, and intra-operative blood loss.
Within our data, propofol is not associated with changes in peri-induction systolic blood pressure; however, there may be individual susceptibility to the vasodilatory effects of propofol. To provide clarity on which patients within the propofol group should or should not have received propofol based on the prevalence of peri-induction hypotension, we performed a logistic regression model evaluating patients receiving propofol to identify independent predictors of hypotension. Our results align with our linear regression model demonstrating that propofol dose was not associated peri-induction hypotension. In contrast to the linear model, which suggests presenting patient physiology may be more impactful than induction agent on peri-induction hypotension, our logistic regression demonstrated a significant effect of massive transfusion on the potentiation of hypotension. This aligns with the concept that physiology and surrogate representation of physiology (ie, needing more resuscitation) drive peri-induction physiology. Induction agent choice is not as contributory as dogma would suggest.
To bolster this, our findings are consistent with 2 recently published trials demonstrating no harm in propofol use during RSI in trauma patients. In their two-center retrospective analysis, Kuza et al found propofol was a safe alternative to etomidate and ketamine and did not portend worse mortality or a higher overall complication rate. Interestingly, they too noted a trend in the use of non-propofol RSI agents in sicker patients. 7 This mirrors our own experience where ketamine and etomidate appeared to be used preferentially in patients with higher ISS and shock index. Similarly, in their eight-center retrospective review, Leede et al reported no reductions in systolic blood pressure following the use of ketamine, etomidate, or propofol. 9 While neither of these studies specifically evaluated hemorrhaging patients, they represent the largest evaluations to date on the effect of RSI agents and provide equipoise that propofol may not be dangerous.
This study has several limitations worth discussing. This is a retrospective cohort study with limitations inherent to its design. Specifically, assessing changes in blood pressure, correlations between medication administration and hemodynamic changes, and the timing and amount of blood products given are all subject to the electronic medical record accurately portraying the temporal events of resuscitation. The stringency of our inclusion criteria limited the overall sample size and reduced statistical power. However, several points are important to consider. First, limitations of data fidelity through the electronic medical record became problematic beyond our three-year study period due to changes in the electronic medical record software. This limited our access to further actionable patient data. Second, we found benefit in performing a focused retrospective assessment of practice variations amongst our anesthesia colleagues, as they serve a vital role in guiding the peri-induction care and resuscitation of the hemorrhaging patient. At our institution, specific induction protocols in the operating room do not exist, so variation in provider practices including induction agent choice, rate of administration and the consequences thereof, are important considerations. Third, patients intubated in the ED were excluded for several reasons: (1) Patients in the ED were almost uniformly induced with ketamine based on institutional norms, which makes like-to-like comparison difficult with patients intubated in the operating room. Vital sign capture to the EMR is less frequent in the emergency room compared to the operating room. In the latter, every vital sign is automatically recorded to the EMR while the former requires nursing confirmation before being tracked in the EMR. (2) The reason and circumstances for intubation of patients in the emergency room vs. operating theater may be entirely different (emergent remediation of an obstructed airway vs. preoperative airway control, for example), which makes comparison problematic. And finally, our study was limited by the baseline differences between the non-propofol and propofol groups. Namely, our non-propofol group was more severely injured with higher shock indices and MTP requirements. Multivariate analysis controlling for injury severity and presenting physiology via shock index did not demonstrate worse peri-induction hypotension, but small sample size may limit interpretation of these results. Nevertheless, our findings align with the greater body of work published on the use of propofol in emergent settings and its apparent safety. Future study should focus on 2 areas: first, prospective evaluation of induction agent safety involving induction agent randomization should be performed to facilitate minimization of confounding and a thorough evaluation of comparative agent safety; second, the hemodynamic effects of induction agent choice in RSI occurring both in the emergency department and in the operating theater should be assessed, to confirm agent safety across care settings.
This is the first study to directly assess the effect of anesthetic induction agent on peri-induction metrics in acutely hemorrhaging patients requiring emergent surgery for penetrating trauma. Propofol does not appear to worsen peri-induction hypotension, regardless of dose. Patient physiology is most predictive of peri-induction.
Footnotes
Acknowledgments
Dr. Jill R. Streams
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the Vanderbilt University Medical Center IRB (IRB# 200789).
Correction (October 2023):
Dr. T. Noel Hess is no longer listed as co-first author.