
Abstract
Introduction
Lower extremity vascular injuries have significant implications for trauma patients with regards to morbidity from limb loss. There is limited evidence on outcomes for patients with injuries to tibial arteries. Our study focuses on defining outcomes of traumatic vascular injury to vessels below the knee.
Methods
A retrospective review using ICD-9 and 10 codes of all patients with below knee vascular injuries was performed at a Level 1 trauma center from November 2014 to June 2022. Interventions, outcomes, and complications were assessed.
Results
Seventy-six patients were identified fitting inclusion criteria. The mean age was 35.3 +/− 15.2 years and 67 (88%) patients were male. Thirty-nine suffered penetrating trauma, 37 suffered blunt trauma. The most injured artery was posterior tibial artery (40%) followed by anterior tibial artery (36%). Injuries included 51 transections, 22 occlusions and 4 pseudoaneurysms. Forty-five (59%) patients underwent operative intervention. Thirty (67%) operations were performed by trauma surgery. Arterial ligation was performed in 30 cases (67%), arterial bypass in 12 (27%), and 2 (4%) primary amputations. Vascular surgery performed all bypasses. Overall amputation rate was 8% (n = 6) with 3 for mangled extremity and 3 due to failed bypass graft. All amputations were associated with open fracture and amputations for failed bypass had multiple arterial injuries.
Conclusion
The management of below knee vascular trauma requires a multidisciplinary approach. Patients requiring reconstruction are more likely to have multiple vessel injuries and may have significant risk of graft failure. These patients as well as those with extensive soft tissue injury and/or multi-vessel injuries are at increased risk for amputation
Background
Lower extremity vascular injuries have significant implications for trauma patients with regards to limb loss and limb specific morbidity and mortality including an up to 10% risk of limb loss and mortality. 1 Previous studies have cited polytrauma, blunt mechanism of injury, vascular reoperation as well as injury to multiple tibial vessels as risk factors for amputation.2-4 Most of the literature describes outcomes regarding vascular injury from below the inguinal ligament; however, there is limited data regarding the outcomes for patients specifically with injuries to tibial arteries. Our study examines the management and clinical outcomes following traumatic vascular injury to vessels below the knee.
Methods
Following exemption from the IRB, a retrospective case series of all patients who suffered below knee vascular injuries was performed at an urban ACS-verified Level 1 trauma center from November 2014 to June 2022. Patients were identified using ICD- 9 and 10 diagnosis codes (904.50-1, 904.53, 904.6-8, S85.1-2, 8-9, S95.0-1, 8-9, respectively). Medical records were reviewed for patient demographics, vital signs, injury severity score (ISS), vascular exam at presentation, artery injured, management, and outcomes.
Inclusion criteria consisted of patients who suffered blunt and/or penetrating vascular injury to the anterior tibial (AT) artery, posterior tibial (PT) artery, and peroneal artery. Patients were excluded from analysis if they, were found to be erroneously coded, had isolated superficial venous injury or isolated injury to small arterial branches of tibial vessels. Injuries were classified as transection (partial or complete), dissection, occlusion, traumatic arteriovenous fistula (AVF), and pseudoaneurysm. Interventions were defined as ligation in the emergency department, ligation in the operating room, primary repair, surgical bypass, thrombectomy, angiogram without intervention or observation.
The primary endpoint was need for amputation. Secondary endpoints were unplanned reoperation, delayed compartment syndrome, in-hospital mortality, deep venous thrombosis (DVT), myocardial infarction (MI), and stroke.
Stata program was used for statistical analyses.
Results
Demographics, Mechanism of Injury, Associated Injury.
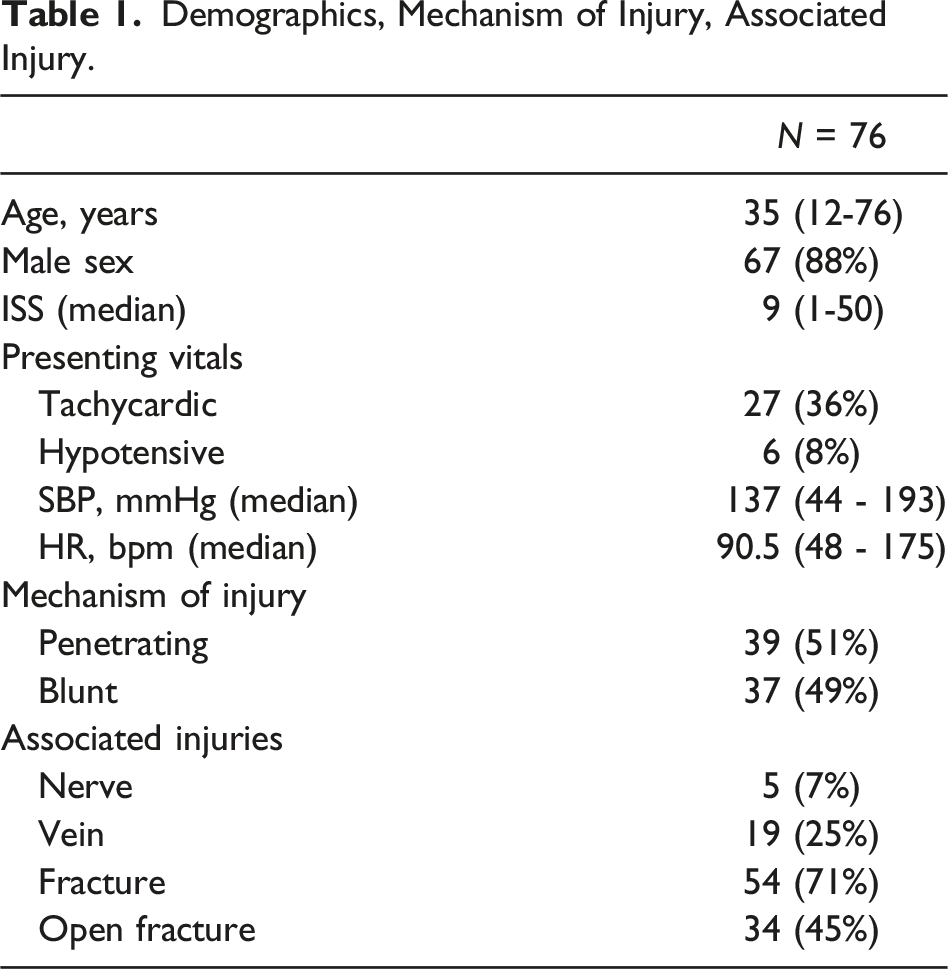
Twenty-seven patients (36%) presented with tachycardia and 6 (8%) with hypotension. Three (4%) patients were both hypotensive and tachycardic on arrival. Sixty-seven patients (88%) underwent imaging with CT-angiography of the lower extremity. Of the 9 patients who did not undergo CT imaging, 7 underwent emergent arterial ligation in the operating room and two underwent arterial ligation in the emergency department. The mean ISS was 11.0 +/− 7.8.
Forty-six patients (61%) had palpable pedal pulses (Dorsalis pedis (DP), posterior tibial (PT) or both) documented on arrival, and 27 had non-palpable pedal pulses. Of those, 12 had no DP or PT Doppler signals present.
Over half of patients (61%, n = 45) underwent operative intervention for their vascular injury. Thirty (67%) operations were performed by trauma surgery and 15 (33%) by vascular surgery.
Hospital and Operative Course.
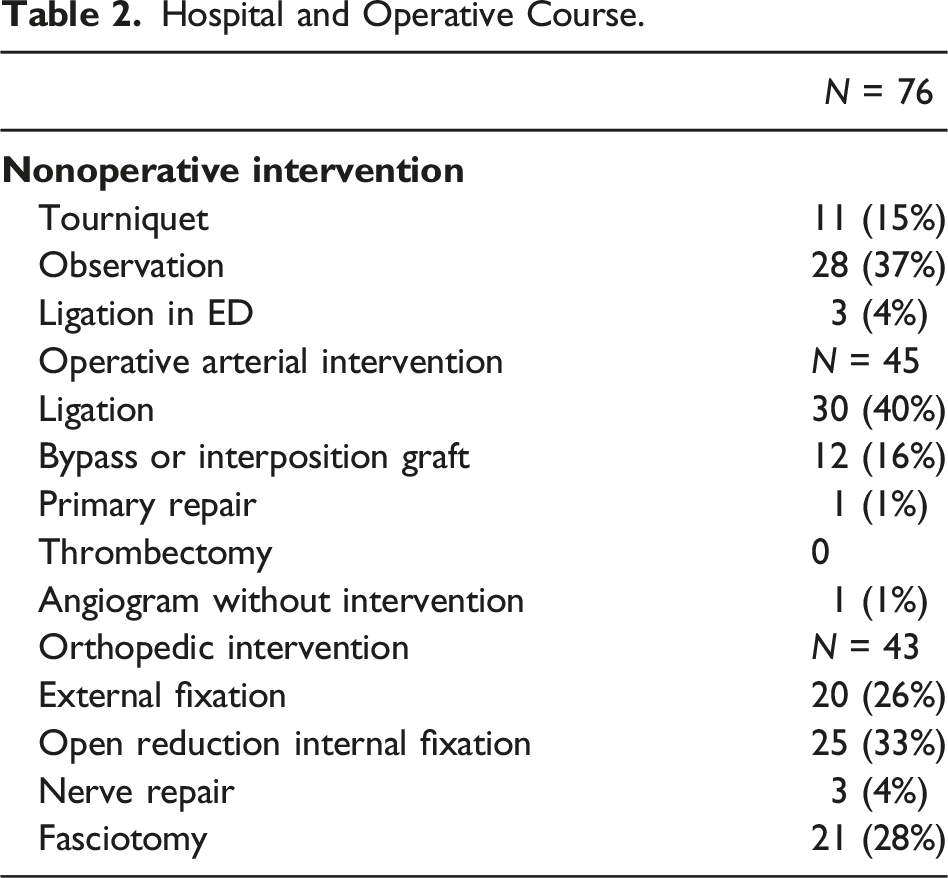
Four (9%) patients required unplanned reoperations, 3 (7%) for thrombosis of arterial bypass, and 1 for management of delayed compartment syndrome. Four (9%) patients underwent delayed amputation with an overall amputation rate of 8% (n = 6).
Three (50%) amputations were performed for mangled extremities and 3 (50%) due to failed arterial bypass and foot ischemia. Of the three that were performed for mangled extremity, two were at index operation due to non-reconstructible fracture and soft tissue loss and one patient elected amputation over free flap for soft tissue coverage. Five (83%) amputations had signs of ischemia (non-Dopplerable signals) at presentation. All amputations were associated with open fractures and all amputations performed for failed arterial bypass had multiple arterial injuries as well as large soft tissue defects on presentation.
Three patients developed DVTs, and there was one in-hospital mortality (brain death due to traumatic head injury).
Discussion
Below knee arterial trauma can have potentially devastating consequences with regards to limb loss. In our study, 6 (8%) patients required amputation and of those, half were due to associated soft tissue defects with bone loss and half due to foot and soft tissue ischemia as a result of arterial bypass graft failure. All patients, however, had large, complex soft tissue injuries upon presentation.
While 50% of amputations in our study were performed due to lower limb ischemia, one must take into consideration that all patients requiring amputation had substantial soft tissue defects on arrival. Many prior studies have documented risk factors for amputation including soft tissue injury, open fracture, nerve injury as well as blunt mechanism of trauma.1-3,5-10 Our study shows similar patterns including open fracture and blunt mechanism. Signs of ischemia on presentation (absent Doppler signals) were also associated with amputation in our study.
Of the 12 below knee arterial bypasses in our study, 3 developed thrombosis during the hospitalization and all three required reoperations for thrombectomy and ultimately below knee amputation. This shows a bypass graft failure rate of 25%. Given the lack of data specific to below knee arterial trauma, one can loosely draw comparisons to below knee tibial bypass for non-traumatic reasons. Prior data shows primary patency rate of 69.1% at 1 year in the setting of tibial bypass grafts performed for chronic limb ischemia. 11 Trauma patients in general, typically are younger with fewer comorbidities; however, in our small sample, patency rates are similar to published data. Tibial bypasses in trauma patients may be at high risk due to the prothrombotic state associated with traumatic injury. 12 Current recommendations note that single vessel injury may not necessitate revascularization interventions, but for patients with multiple arterial injuries, at least one tibial vessel should be repaired primarily or revascularized with an interposition or extra-anatomic bypass graft. 13
Risk Factors for Amputation.
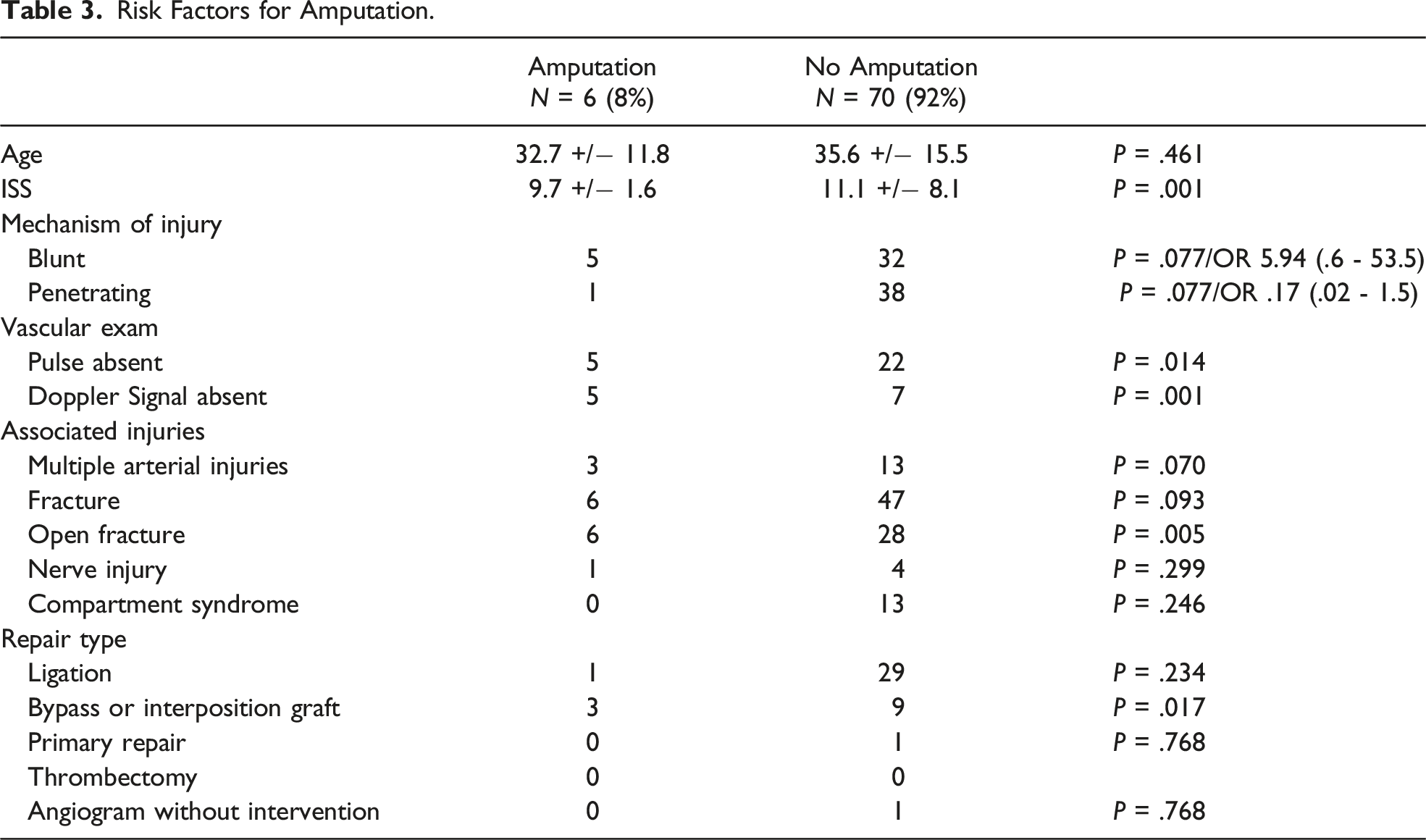
Two thirds of our cohort who underwent operative intervention had arterial ligation. Of those, most had single vessel injury with only three with multiple arterial injury. In those with multiple injuries, at least one tibial vessel remained intact. All patients had evidence of limb perfusion (palpable pulse or Doppler signal present). No patients in this group underwent amputation. This may suggest that ligation can be safely performed without revascularization in patients without signs of ischemia and at least one tibial vessel intact. The majority of our patients were diagnosed with arterial imaging by CTA. Patients who present with fractures of tibia or fibula may benefit from CTA to identify potential injury to tibial vessels with the exception of those with active arterial hemorrhage who require immediate intervention.
Risk Factors for Amputation Among Tibial Bypass Graft.
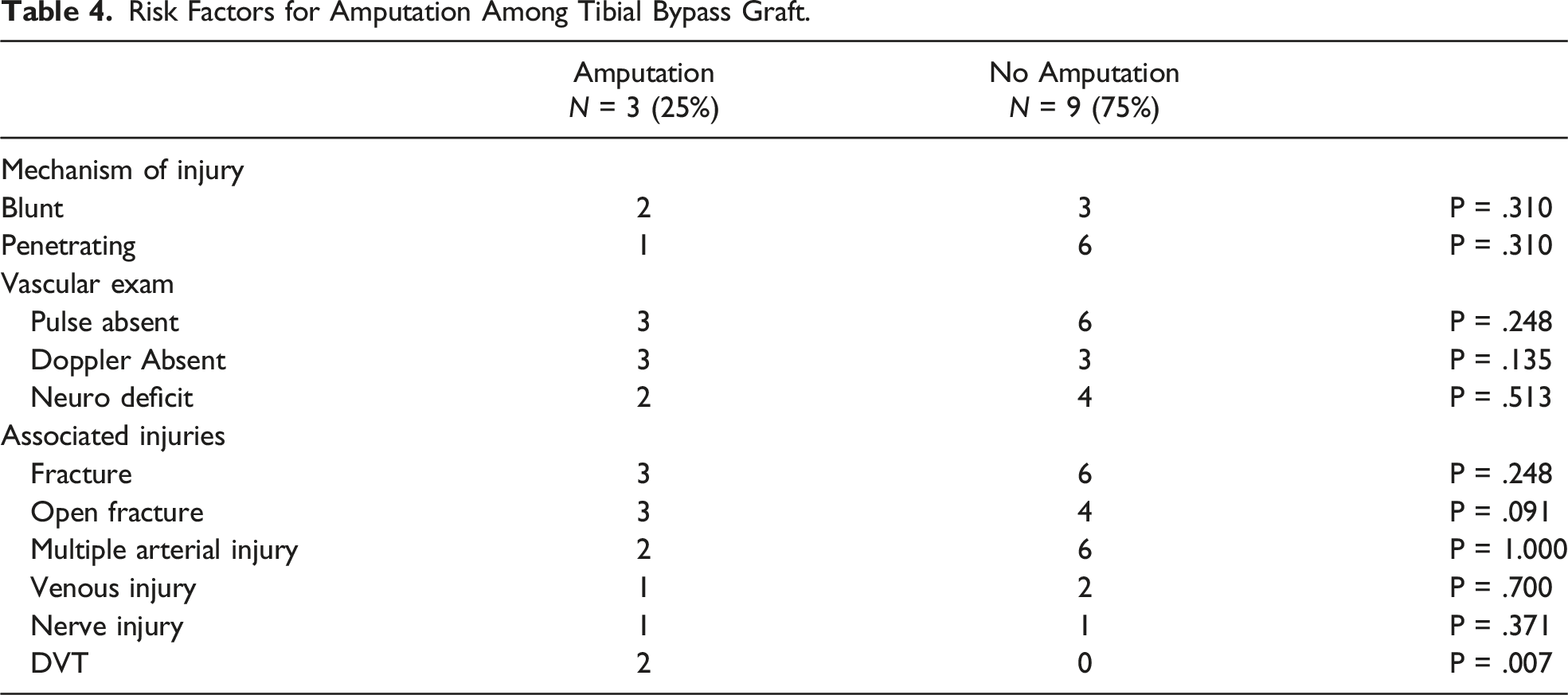
Prior studies have shown poor predictors of amputation in patients with mangled extremity or lower extremity vascular trauma. 15 Our study is consistent with this and that decision for amputation should be individualized and involve a multidisciplinary team.
This study has limitations due to its retrospective design. Medical records were reviewed and certain details of the vascular exam, size, and severity of soft tissue defects as well as multidisciplinary decision for amputation may not have been adequately recorded. Additionally, our study is from a single institution and has a relatively small sample size. Despite this, our study provides opportunity for further investigation into the potential limb salvage in patients with below knee arterial trauma.
Conclusion
The management of below knee vascular trauma requires a multidisciplinary approach to address small arterial injuries. Patients requiring arterial reconstruction are more likely to have multiple vessel injuries and may have significant risk of graft failure, as high as 25%. These patients as well as those with extensive soft tissue injury and/or multi-vessel injuries are at increased risk for amputation.
ORCID iD
Tessa Lamberton https://orcid.org/0000-0002-2093-0593
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.