
Abstract

Hepatic cystic echinococcosis (HCE), also known as hydatid disease, is a complex zoonotic disease with the highest prevalence in Argentina, Peru, East Africa, Central Asia, and China. 1 While rare in the United States, HCE can be a severe, fatal disease, so it should be included in the differential diagnosis for liver cysts, especially if the patient has traveled to an endemic country.
Patients with HCE may be asymptomatic for years because these cysts grow slowly, but symptoms and complications may arise as the cyst gets larger. 1 Cysts may cause obstructive symptoms depending on their location and have been described to cause jaundice secondary to biliary obstruction. While rare, anaphylaxis is a serious complication and should be considered in patients with HCE, especially during invasive treatment. Rupture of echinococcal cysts and release of their contents into the peritoneal cavity can cause anaphylaxis and death. 1
Depending on cyst size and the number of cysts, a combination of several different therapeutic approaches may be employed. Anthelmintic chemotherapy, watch and wait, percutaneous therapies, and surgery have been described as options to treat HCE. In this original publication, we present a case of surgical treatment of massive HCE.
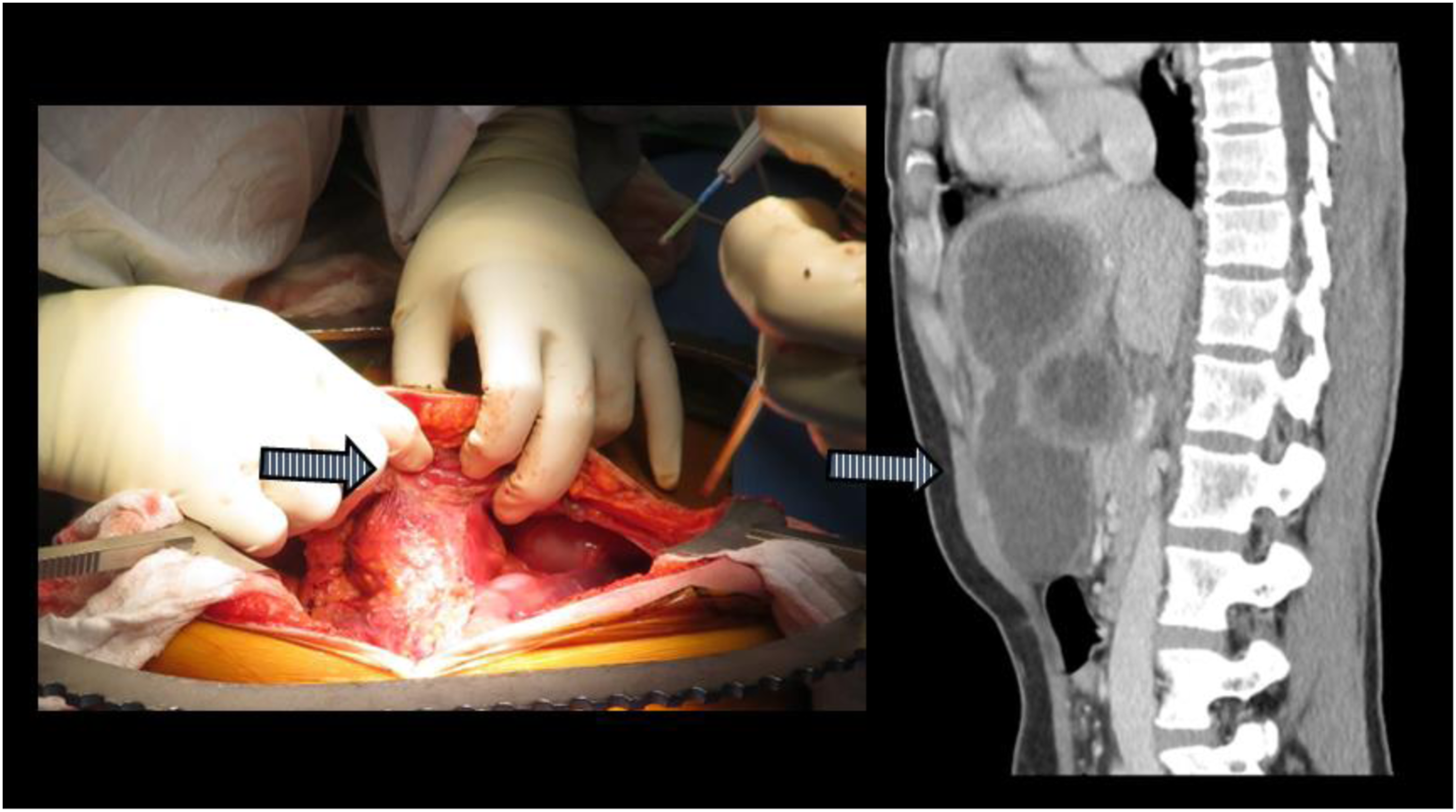
A 33-year-old female from Syria who immigrated to the United States 5 years prior with no significant past medical history presented with a history of 2 month worsening abdominal pain and enlarging epigastric mass. She also described having early postprandial epigastric fullness. She had no fever, nausea, jaundice, or any other symptoms. On physical exam, she was of a petite body habitus with a large visible and palpable epigastric mass. She had no laboratory work abnormalities. Serum anti-echinococcus antigen IgG antibody was positive. An abdomen computed tomography scan with intravenous contrast showed the left lateral hepatic segments were entirely covered by multiloculated cystic lesions with punctate peripheral calcifications and internal daughter cysts concerning for hydatid cysts. These lesions caused significant mass effect on the stomach. Another cyst involving segment 4 (left medial) included a 6 cm × 5.2 cm x 7 cm intraparenchymal component and a 5.9 cm × 5.1 cm x 6.6 cm exophytic component with concern for invasion of the abdominal wall (Figures 1 and 2). Coronal CT images of the abdomen and post-resection specimen. Dotted white line and arrows indicate line of transection during left hepatectomy. Sagittal CT image of the abdomen and intraoperative photo showing invasion of anterior abdominal wall, arrow. Note proximity of lesions with abdominal wall and viscera.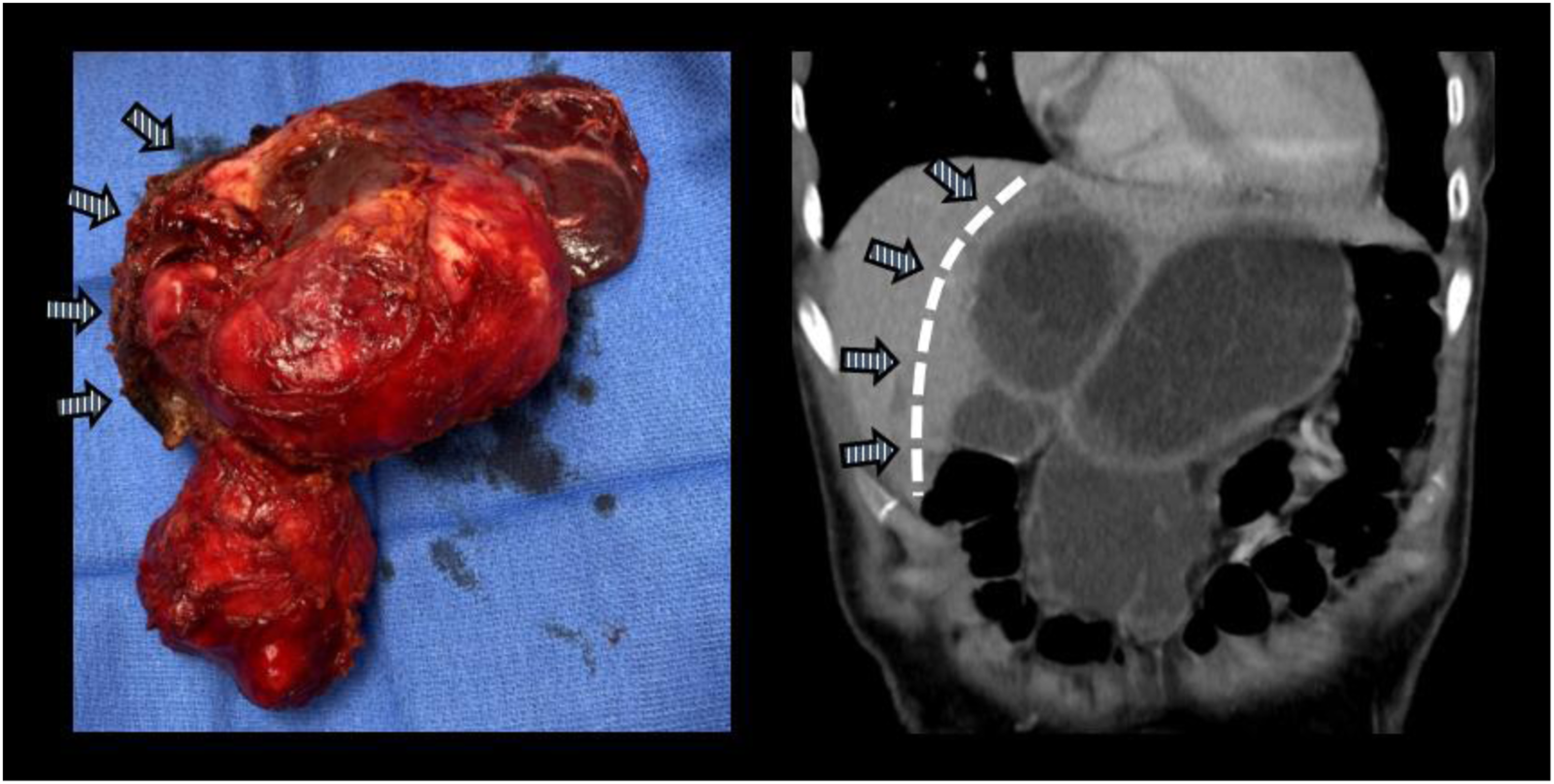
She was evaluated by a multidisciplinary team including infectious disease, hepatology, and surgery and the decision was made to admit her and to start treatment with albendazole and praziquantel in preparation for surgical treatment. Although an extended course of anthelmintic therapy was preferred prior to intervention, given her symptoms, a one-week course was agreed upon prior to proceeding to the operating room for an exploratory laparotomy and left hepatectomy.
Through a bilateral subcostal incision, the abdomen was explored and there were dense adhesions to the anterior abdominal wall as expected from the CT scan. It was thought this might be due to a prior contained rupture into the abdominal wall and so a small portion of the peritoneum and muscle was resected en bloc. The peritoneal cavity was packed with hypertonic saline soaked towels and a formal left hepatectomy was performed. The extra hepatic left portal vein and hepatic artery were divided and the parenchyma was divided along the line of demarcation, Cantlie’s line. The middle hepatic vein was preserved. The operative time was 300 minutes with an estimated blood loss of 300 milliliters. Her postoperative course was uneventful. She tolerated a regular diet after three days and went home on postoperative days 6. After two months, she had gained 10% of her body weight and continued her planned six-month course of albendazole without issue. She was last seen 8 months after surgery completely asymptomatic.
Pathology revealed cysts with a thick fibrous rim as well as multiple daughter cysts and cyst fluid with protoscolices consistent with the suspected diagnosis of HCE.
Echinococcal liver disease treatment has evolved in the last several years with an increased variety of options available for the clinician today. Therapy should be guided by the clinical status of the patient, the number and size of the lesions, and center expertise. The ultrasound-based classification described by the WHO-IWGE aids in guiding treatment. 1
Benzimidazole therapy is the medical treatment of choice for hepatic cysts. Albendazole and mebendazole have been proven to be effective in liver and peritoneal cyst disease. Albendazole is more effective since its metabolites are more active than mebendazole. The EchioMedrev study collected data from six different centers adding up to 711 patients. 1-2 years after initiation of benzimidazole treatment, 50%-75% of active C1 cysts were classified as inactive/disappeared, and 30%-55% of CE2 and CE3 cysts. 50%-60% of cysts less than 6 cm responded to treatment compared to 25%-50% of cysts greater than 6 cm. Still, 25% of cysts reverted to active status within 1.5-2 years after having initially responded. After the second and third treatment, 60% of cysts relapsed within 2 years. They estimated that after 2 years 40% of cysts are still active or become active again. 2
Indications for PAIR (Puncture, Aspiration, Injection, and Re-aspiration) include single compartment cysts (WHO-IGWE CE1 and CE3a) less than 5 cm that did not respond to chemotherapy and in combination with medical therapy for cysts over 5 cm. 1 Multiseptated cysts, superficial cysts with a risk of rupture, or cysts that communicate with biliary structures are not candidates for PAIR. PAIR consists of draining the cyst and afterward injecting it with a scolicidal agent. Smego et al 3 analyzed 769 patients with hepatic cysts treated with PAIR and compared them to historical patients treated surgically. They concluded that PAIR with chemotherapy has better clinical and parasitological efficacy, and lower rates of morbidity, mortality, and disease recurrence. This makes PAIR an excellent tool for patients with CE1 and CE3a disease.
Surgery is the traditional treatment of echinococcal liver disease, but many discussions still exist regarding which procedure should be done. The leading debate is conservative vs more radical approaches. Different surgical techniques have been described but the goal is the same: remove the cyst, avoid spillage to the abdominal cavity, and repair any contiguous lesions that the cyst might have caused (such as a biliary fistula). Literature describes the treatment for gigantic liver cysts, but we could only find 2 patients described by Pavlidis et al 4 in which a formal hepatectomy was done. They described two patients with lesions of 18 and 20 cm that underwent a left hepatectomy as we did with our patient. To our knowledge, our case is the 3rd case reported of a left hepatectomy due to massive involvement of hydatid liver disease.
Despite a variety of treatment options, surgery remains the mainstay treatment for advanced echinococcal liver disease. The WHO-IGWE classification and expertise at each center should guide the best therapy for patients with liver echinococcus. Transfer to experienced hepatobiliary centers may be warranted. A multidisciplinary approach to these patients is crucial to obtain the best results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.