
Abstract
Background
Some reports suggest Diagnostic peritoneal aspiration (DPA) or lavage (DPL) may better select which hypotensive blunt trauma patients (BTPs) require operation, compared to ultrasonography. However, whether both moderately hypotensive (systolic blood pressure [SBP] < 90 mmHg) and severely hypotensive (SBP < 70 mmHg) patients benefit from DPA/DPL is unclear. We hypothesized DPA/DPL used within the first hour increases risk of death for severely vs moderately hypotensive BTPs.
Methods
The 2017-2019 Trauma Quality Improvement Program database was queried for BTPs ≥ 18 years old with hypotension upon arrival. We compared moderately and severely hypotensive groups. A multivariable logistic regression analysis was performed controlling for age, comorbidities, emergent operation, blood transfusions, and injury profile.
Results
From 134 hypotensive patients undergoing DPA/DPL, 66 (49.3%) had severe hypotension. Patients in both groups underwent an emergent operation (43.9% vs 58.8%, P = .09) in a similar amount of time (median, 42-min vs 54-min, P = .11). Compared to the moderately hypotensive group, severely hypotensive patients had a higher rate and associated risk of death (84.8% vs 50.0%, P < .001) (OR 5.40, CI 2.07-14.11, P < .001). The strongest independent risk factor for death was age ≥ 65 (OR 24.81, CI 4.06-151.62, P < .001).
Discussion
Among all BTPs undergoing DPA/DPL within the first hour of arrival, an over 5-fold increased risk of death for patients with severe hypotension was demonstrated. As such, DPA/DPL within this group should be used with caution, particularly for older patients, as they may be better served by immediate surgeries. Future prospective research is needed to confirm these findings and elucidate the ideal DPA/DPL population in the modern era of ultrasonography.
Keywords
• Blunt trauma patients with severe hypotension are associated with increased risk of mortality compared to patients with moderate hypotension after DPA/DPL. • Older age (65 years and older) blunt trauma patients have an over 25 times higher risk of death when DPA/DPL is performed.Key Takeaways
Introduction
Trauma is the leading cause of mortality within the first 4 decades of life in the United States. 1 Blunt trauma is the most common mechanism of injury and may result in multiple injuries throughout the body. 2 Hypotension after trauma is most commonly related to hemorrhage and is considered the leading cause of preventable death for blunt trauma patients (BTPs). 1 However, the etiology of hypotension (ie, non-compressible torso hemorrhage, neurogenic shock, blunt cardiac injury, etc.) and the source of hemorrhage are not always easily identified soon after a BTPs arrival. 3 If hypotension becomes life-threatening, resuscitation must be initiated and hemorrhage control achieved in a timely fashion.1,3 Some BTPs may require an emergency laparotomy due to intra-abdominal hemorrhage, which may be life-saving when performed in a timely manner. 1
Unfortunately, clinical examination alone is unreliable in detecting the source of bleeding in BTPs. 4 Currently available tools to augment the detection of significant intra-abdominal hemorrhage include the focused assessment with sonography for trauma (FAST) exam and diagnostic peritoneal aspiration (DPA) or lavage (DPL). Although computed tomography (CT) imaging is used frequently for BTPs, it is not appropriate for patients that are persistently hypotensive even after resuscitation as it may delay hemorrhage control. 5
Historically, DPA/DPL were the gold standard to help identify intra-abdominal hemorrhage in BTPs with reported sensitivities and specificities of 82%-96% and 87%-99%, respectively.6,7 However, with increased use of the FAST exam, and early reports of reasonable sensitivity (73%-88%) and specificity (98%-100%),8,9 and the non-invasive nature of the FAST exam, it soon replaced DPA/DPL as the diagnostic test of choice in the hemodynamically unstable BTP. 10 More recently there have been questions regarding the accuracy of FAST examinations.5,10 Thus, there has been some renewed interest in using DPA/DPL for unstable BTPs. 10
In the modern era, it is unclear which BTPs benefit from DPA/DPL and whether this procedure is suitable for all degrees of hypotension, including those with severe hypotension (eg, systolic blood pressure [SBP] < 70 mmHg). Therefore, this study aimed to compare the use of DPA/DPL in moderately hypotensive (SBP 70-90 mmHg) vs severely hypotensive (SBP < 70 mmHg) BTPs. We hypothesized that patients presenting with severe hypotension have an increased risk of mortality compared to patients with moderate hypotension who undergo DPA/DPL within the first hour of arrival.
Methods
This study was deemed exempt and a waiver of consent was granted by our institutional review board as it utilizes a national deidentified database. The 2017-2019 Trauma Quality Improvement Program (TQIP) database was queried for patients 18 years of age and older presenting after blunt trauma. Transferred patients and those with a penetrating trauma mechanism were excluded. We then selected for BTPs presenting with hypotension (SBP < 90 mmHg) on arrival and requiring a DPA/DPL within 1 hour. DPA refers to the insertion of a catheter in the peritoneal cavity and aspiration of any fluid, while DPL involves infusion of normal saline, lavage of the cavity, and evaluation of the returned fluid, requiring more time for completion and analysis.10,11
Two groups were compared: patients with moderate (SBP 70-–90 mmHg) and severe (SBP < 70 mmHg) hypotension on arrival. The primary outcome was mortality. Secondary outcomes included hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, and the number of packed red blood cells transfused within 4 hours and emergent operative intervention. Demographic variables collected for this study included age, sex, Glasgow coma scale (GCS), vitals on admission, and comorbidities including chronic obstructive pulmonary disease (COPD), congestive heart failure, and diabetes. The injury profile included the injury severity score (ISS) and rates of injury to the head.
Bivariate analyses were performed using a Mann-Whitney U test to compare continuous variables and Pearson’s chi-squared analysis to compare categorical variables. Continuous variables were reported as medians with an interquartile range and categorical variables were reported as frequencies. After a discussion among coauthors and a review of the literature, we selected variables available in TQIP that are associated with a higher risk of death. 12 We then included these variables in a univariable logistic regression model and those with a P-value < .20 were then utilized in a multivariable logistic regression analysis. The variables included age ≥ 65 years old, moderate (SBP 70-–90 mmHg) or severe (SBP < 70 mmHg) hypotension on admission, hypertension (SBP > 14 mmHg) at the time of arrival, chronic obstructive pulmonary disease, and severe AIS to the head. We also controlled for the injury severity score (ISS ≥ 25), severe thorax and abdomen injuries (AIS > 3), number of packed red blood cells transfused, number of BTPs transported to the operating room from the emergency room, and comorbidities (cirrhosis, cerebrovascular accident, congestive heart failure). The hierarchical multivariable logistic regression model evaluated the adjusted risk for death for severe vs moderate hypotension and reported this with an odds ratio (OR) and 95% confidence intervals (CI). All analyses were conducted using IBM SPSS Statistics for Windows (version 28; IBM Corporation, Armonk, NY), with a statistical significance set at P < .05.
Results
Demographics, Vitals, and Comorbidities of Moderately vs Severely Hypotensive BTPs Undergoing DPA/DPL
Demographics, Vitals, and Injury Profile of Blunt Trauma Patients with Moderate vs Severe Hypotension Who Undergo Diagnostic Peritoneal Aspiration or Lavage Within 1 Hour of Arrival.
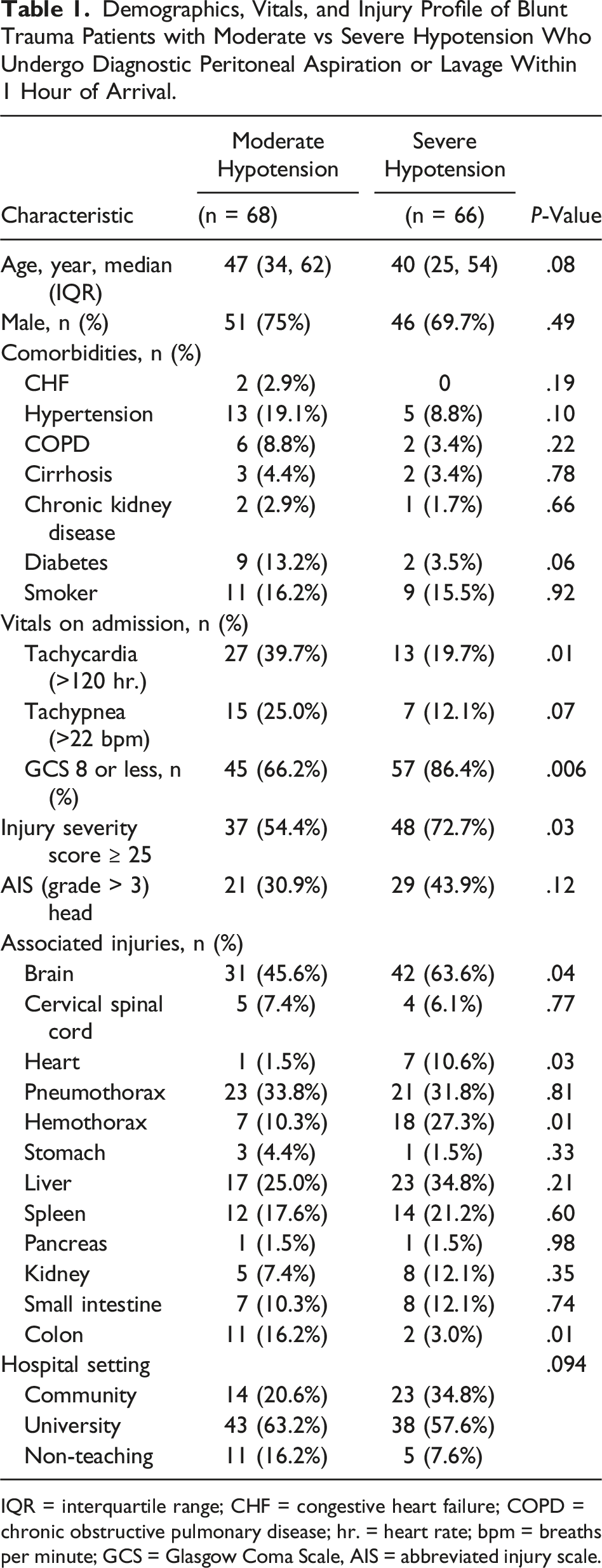
IQR = interquartile range; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; hr. = heart rate; bpm = breaths per minute; GCS = Glasgow Coma Scale, AIS = abbreviated injury scale.
Injury Profile of Moderately vs Severely Hypotensive BTPs Undergoing DPA/DPL
BTPs with severe hypotension had a higher rate of severe trauma (ISS ≥ 25) (72.7% vs 54.4%, P = .03) compared to the moderately hypotensive group. The majority of organs injured were similar between cohorts, except the severely hypotensive group had a lower rate of injury to the colon (3.0% vs 16.2%, P = .01) but had higher rates of hemothorax (27.3% vs 10.3%, P = .01) and injury to the brain (63.6% vs 45.6%, P = .04) and heart (10.6% vs 1.5%, P = .03) compared to the moderately hypotensive group (Table 1).
Clinical Outcomes of Moderately vs Severely Hypotensive BTPs Undergoing DPA/DPL
Outcomes of Blunt Trauma Patients with Moderate vs Severe Hypotension Who Undergo Diagnostic Peritoneal Aspiration or Lavage Within 1 Hour of Arrival.
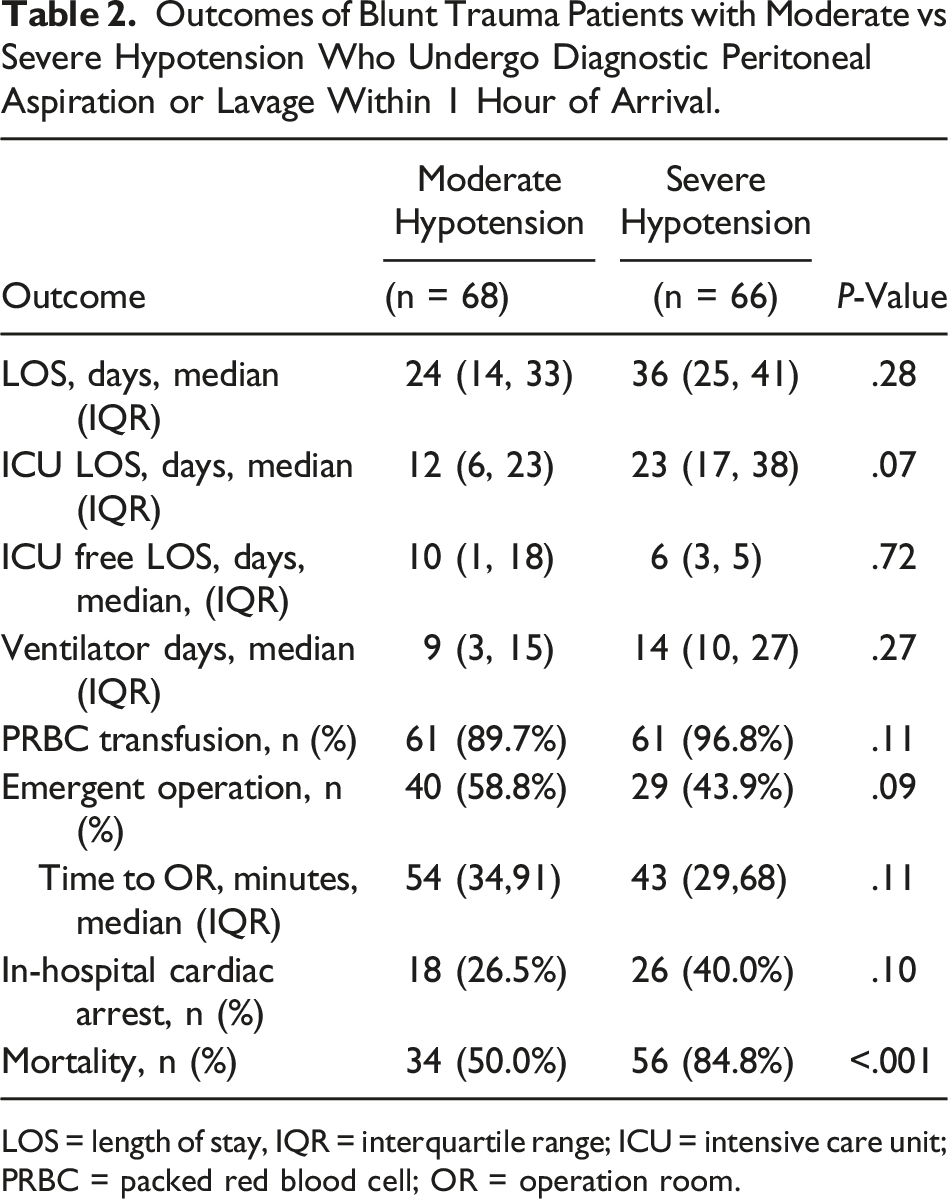
LOS = length of stay, IQR = interquartile range; ICU = intensive care unit; PRBC = packed red blood cell; OR = operation room.
Multivariable a Logistic Regression Analysis for Risk of Death in Blunt Trauma Patients With Hypotension Who Undergo Diagnostic Peritoneal Aspiration or Lavage Within 1 Hour of Arrival.
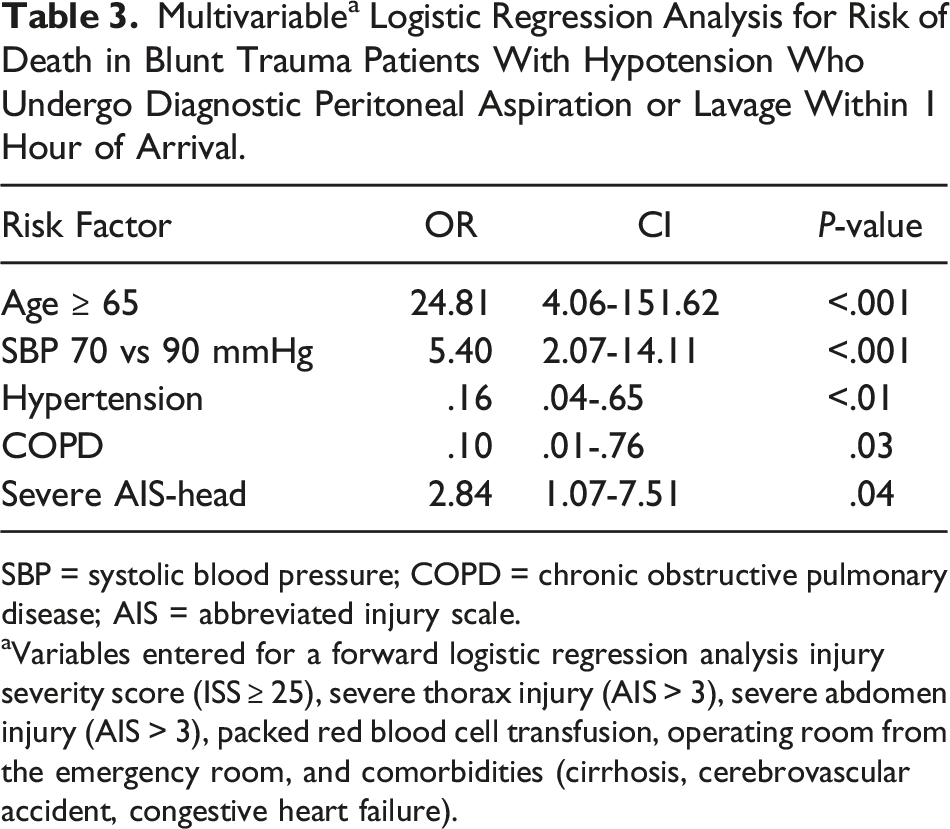
SBP = systolic blood pressure; COPD = chronic obstructive pulmonary disease; AIS = abbreviated injury scale.
aVariables entered for a forward logistic regression analysis injury severity score (ISS ≥ 25), severe thorax injury (AIS > 3), severe abdomen injury (AIS > 3), packed red blood cell transfusion, operating room from the emergency room, and comorbidities (cirrhosis, cerebrovascular accident, congestive heart failure).
Discussion
There is now a renewed interest in the use of DPA/DPL for hypotensive trauma patients as several recent studies have demonstrated limitations of the FAST exam.5,10 However, the ideal population for the use of DPA/DPL remains ill defined. This national study demonstrated that the risk of death in BTPs who underwent DPA/DPL with severe hypotension was over 5 times greater than that of moderately hypotensive patients undergoing DPA/DPL within 1 hour of arrival. In addition, in all BTPs undergoing DPA/DPL, patients over the age of 65 had an over 25 times increased risk of death when DPA/DPL was performed suggesting that the use of DPA/DPL in older adult patients with severe hypotension should be performed with extreme caution as they may not benefit from this tool and may be better served by immediate surgery instead of another diagnostic procedure. Finally, despite using multiple years of recent national data, we found that the use of DPA/DPL continues to be rare in current practice.
Blunt trauma injuries can be occult, clinically asymptomatic, and fatal, highlighting the importance of using effective tools or diagnostic studies to identify such injuries. 13 In hypotensive BTPs, the margin of error for any diagnostic test must be very low to prevent catastrophic consequences. 5 DPA/DPL were previously considered the gold standard due to relatively high sensitivity and specificity. 14 In 1965, Root et al reported a dramatic decrease in morbidity and mortality for trauma patients with unknown intraperitoneal hemorrhage in the first series of DPL utilization. 15 More recently, in 2016, Li et al. emphasized the significance of DPA/DPL use on lowering complication and mortality rates. 16 In addition, DPA/DPL can help quickly differentiate between blood and enteric contents, thus guiding surgical treatment and improving the rate of mortality.9,17 In this study, we found that DPA/DPL used in BTPs with moderate and severe hypotension is associated with a nearly 50% and 90% mortality rate, respectively. Furthermore, severely hypotensive BTPs had an over 5-fold increased associated risk of death even when controlling for other known predictors of mortality. This calls to question the use of this diagnostic treatment in this population, who may be best served by immediate surgical intervention (eg, resuscitative thoracotomy, emergent laparotomy etc.).
In view of the invasive nature of DPA/DPL,6,8 the safety profile has to be incorporated into any risk/benefit discussion regarding its use. Drew et al determined that use of DPA/DPL in children under 10 years of age with blunt trauma had an accuracy above 99% in determining the presence or absence of intra-abdominal hemorrhage. 18 This has further been corroborated in studies of adolescents and generalized adult populations.4,10,13 However, none of these studies specifically stratified older adults (eg, > 65 years old). It has been well documented that patients over the age of 65 tend to have higher morbidity and mortality rates following a major trauma. The less tolerance to injuries in these patients can attribute to many factors. 19 Elderly patients have a higher prevalence of underlying comorbidities and medication use including anticoagulants, therefore adversely affecting the prognosis due to increased complications, organ dysfunction, and death.19,20 Preexisting comorbidities including cardiovascular, respiratory, hepatic and renal disease, as well as diabetes are known to dramatically increase mortality in older adults. 19 Also, older patients are more likely to die from blunt trauma, whereas younger patient’s mortalities are due to penetrating trauma. 19 In this current study, DPA/DPL use in BTPs over the age of 65 was associated with an over 25 times increased risk of mortality. Future studies are needed to confirm these findings but, in the meantime, providers should be cautious with using DPA/DPL in older adults.
Limitations of this study include those inherent to retrospective database studies, such as missing data, coding errors, as well as selection and reporting bias. This study has a large number of variables compared to the limited number of patients, which can bring about unstable results. Also, despite this being a national analysis the incidence of DPA/DPL was relatively rare, and whether DPA or DPL was used specifically is unknown. In addition, potential unaddressed confounders include not knowing the duration of the DPA/DPL procedure (ie, minutes the procedures lasted and when it started in relation to the time of arrival), and cause of patient death. Also, the TQIP database only includes index hospitalization data and thus may underestimate mortality and complications. Another limitation of this study is the lack of data regarding if other modalities such as FAST or CT imaging were also used and their temporal relationship to DPA/DPL. Furthermore, the findings of the DPA/DPL (eg, if positive and was blood or enteric contents found) are not known, although the incidence of emergent operations was similar between cohorts. Finally, we were unable to determine the sensitivity and specificity of the DPA/DPL performed, and again this study does not compare those who underwent DPA/DPL vs those who did not. Thus, the conclusions do not address definitively whether to perform this diagnostic test, they merely serve as data for providers considering using DPA/DPL.
Conclusion
This national analysis spanning 3 years of data found that the associated risk of mortality in only BTPs undergoing DPA/DPL is greater for those who present with severe hypotension and undergo DPA/DPL compared to moderate hypotension and undergo DPA/DPL. Also, importantly after adjusting for known risk factors of mortality in a population that underwent DPA/DPL, there was a substantial association between death and older age, defined as 65 years and older. Thus, the authors suggest that DPA/DPL for older BTPs presenting with severe hypotension should be used with caution. Future prospective research with larger patient samples and direct comparisons of DPA/DPL vs no DPA/DPL are needed to confirm these findings and elucidate if there is an ideal population for DPA/DPL use in the modern era of ultrasonography.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.