
Abstract
Background
Over 20% of United States adolescents are obese. A thicker layer of subcutaneous adiposity might provide a protective “armor” layer against penetrating wounds. We hypothesized that adolescents with obesity presenting after isolated thoracic and abdominal penetrating trauma have lower rates of severe injury and mortality than adolescents without obesity.
Methods
The 2017-2019 Trauma Quality Improvement Program database was queried for patients between 12 and 17 years old presenting with knife or gunshot wounds. Patients with body mass index (BMI) ≥30 (obese) were compared to patients with BMI <30. Sub-analyses were performed for adolescents with isolated abdominal trauma and isolated thoracic trauma. Severe injury was defined as an abbreviated injury scale grade >3. Bivariate analyses were performed.
Results
12,181 patients were identified; 1603 (13.2%) had obesity. In isolated abdominal gunshot or knife wounds, rates of severe intra-abdominal injuries and mortality were similar (all P > .05) between groups. In isolated thoracic gunshot wounds, adolescents with obesity had a lower rate of severe thoracic injury (5.1% vs 13.4%, P = .005) but statistically similar mortality (2.2% vs 6.3%, P = .053) compared to adolescents without obesity. In isolated thoracic knife wounds, rates of severe thoracic injuries and mortality were similar (all P > .05) between groups.
Discussion
Adolescent trauma patients with and without obesity presenting after isolated abdominal or thoracic knife wounds had similar rates of severe injury, operative intervention, and mortality. However, adolescents with obesity presenting after an isolated thoracic gunshot wound had a lower rate of severe injury. This may impact the future work-up and management of adolescents sustaining isolated thoracic gunshot wounds.
Keywords
Key Takeaways
• Adolescent trauma patients with and without obesity presenting after isolated abdominal or thoracic knife wounds had similar rates of severe injury, operative intervention, and mortality. • Adolescents with obesity presenting after an isolated thoracic gunshot wound had a lower rate of severe injury but a similar rate of mortality.
Introduction
The prevalence of obesity in adolescents has steadily increased in the United States from 10.5% in 1988 to 21.2% in 2018. 1 Furthermore, injury is the leading cause of death in adolescents, causing more than 60% of deaths annually. 2
Due to a rising prevalence of obesity and a higher rate of mortality in the adolescent population following trauma, the relationship between obesity and injury is of particular interest to trauma providers. Some authors have proposed possible protective mechanisms of excess body mass, such as the “cushion effect,” where abdominal fat functions as insulating tissue from blunt abdominal trauma 3 and the “armor phenomenon,” where subcutaneous fat distribution limits the wound depth from a penetrating injury (ie, stab wound or gunshot wound). 4
Previous authors have investigated if obesity is truly associated with decreased injury severity and morbidity after trauma in the adult population with varied results. A higher body mass index (BMI) has been associated with a lower mortality5,6 and injury severity score (ISS) 3 for adult blunt trauma patients, and a recent meta-analysis by Chen et al, concluded that an armor phenomenon may exist for adolescents with obesity that sustain thoracoabdominal stab injuries, but this may not lead to improved outcomes. 4 In fact, some studies have found that patients with obesity have a longer length of stay (LOS) in the intensive care unit (ICU) after trauma 7 and obesity is an independent risk factor for complications such as nosocomial infections, 8 prolonged mechanical ventilation, and postoperative pulmonary complications. 9
However, studies in the adolescent population evaluating the effect of obesity on injury after penetrating trauma are limited. In children, studies have reported differences in injury patterns between patients with obesity and without obesity but have failed to demonstrate a significant difference in mortality, length of stay, or complications. However, this may be due to limitations of sample size inherent to a single-center study design.10-12
Therefore, this study aims to examine the association between obesity in adolescents and severe penetrating torso injuries using a large national database. We hypothesize that adolescents with obesity presenting after penetrating thoracic and abdominal trauma have a lower rate of severe traumatic injury and mortality.
Methods
Data Source
This study was approved, and a waiver of consent granted under our Institutional Review Board as part of a national database study using deidentified patient data. A retrospective analysis using the Trauma Quality Improvement Program (TQIP) from years 2017 to 2019 was performed. The TQIP database was queried to identify adolescent patients between the ages of 12 and 17 years old who presented with knife or gunshot wounds. Patients with missing information for either height or weight were excluded.
Study Outcomes and Inclusion/Exclusion Criteria
The primary outcome was severe injury to the abdomen or thorax for each analysis, respectively; this was defined by an abbreviated injury scale (AIS) grade >3 for the respective body region. Mortality was the secondary outcome. Additional outcomes evaluated included total hospital LOS, ICU LOS, and ventilator days.
Patient demographic data was collected including age, sex (self-reported), ISS, race, and comorbidities (diabetes, attention deficit hyperactivity disorder, hypertension, personality disorder, smoking, and substance abuse). Injuries collected included the small intestine, colon, rectum, pancreas, lung, kidney, liver, spleen, and bladder. Operations involving the respiratory, gastrointestinal, urinary, hepatobiliary, and cardiovascular systems were also collected, according to the International Classification of Diseases (ICD)-10 procedure codes.
The BMI for all patients was calculated. Two groups were compared: adolescent penetrating trauma patients with obesity (BMI ≥30 kg/m2) and adolescent penetrating trauma patients without obesity (BMI <30 kg/m2). We performed a separate sub-analysis for isolated abdominal penetrating trauma by excluding all patients with any grade of injury outside of the abdomen using the AIS for the head, neck, thorax, upper extremity, and lower extremity. A similar sub-analysis was performed for isolated thoracic penetrating trauma, excluding all patients with any grade of injury outside of the thorax (ie, AIS for the head, neck, abdomen, upper extremity, and lower extremity).
Statistical Methods
Continuous variables were compared using Mann-Whitney U test and represented with medians and interquartile range. Categorical variables were compared using chi-square and represented with percentages. Adolescents with obesity were compared to a reference group of adolescents without obesity. All P-values were two-sided, with a statistical significance level of <.05. All statistical analyses were performed with IBM SPSS Statistics for Windows, version 28. (Armonk, NY: IBM Corp).
Results
Demographics, Comorbidities, and Injury Profile
Demographics of Patients With Penetrating Injuries Stratified by Obese vs Non-obese.
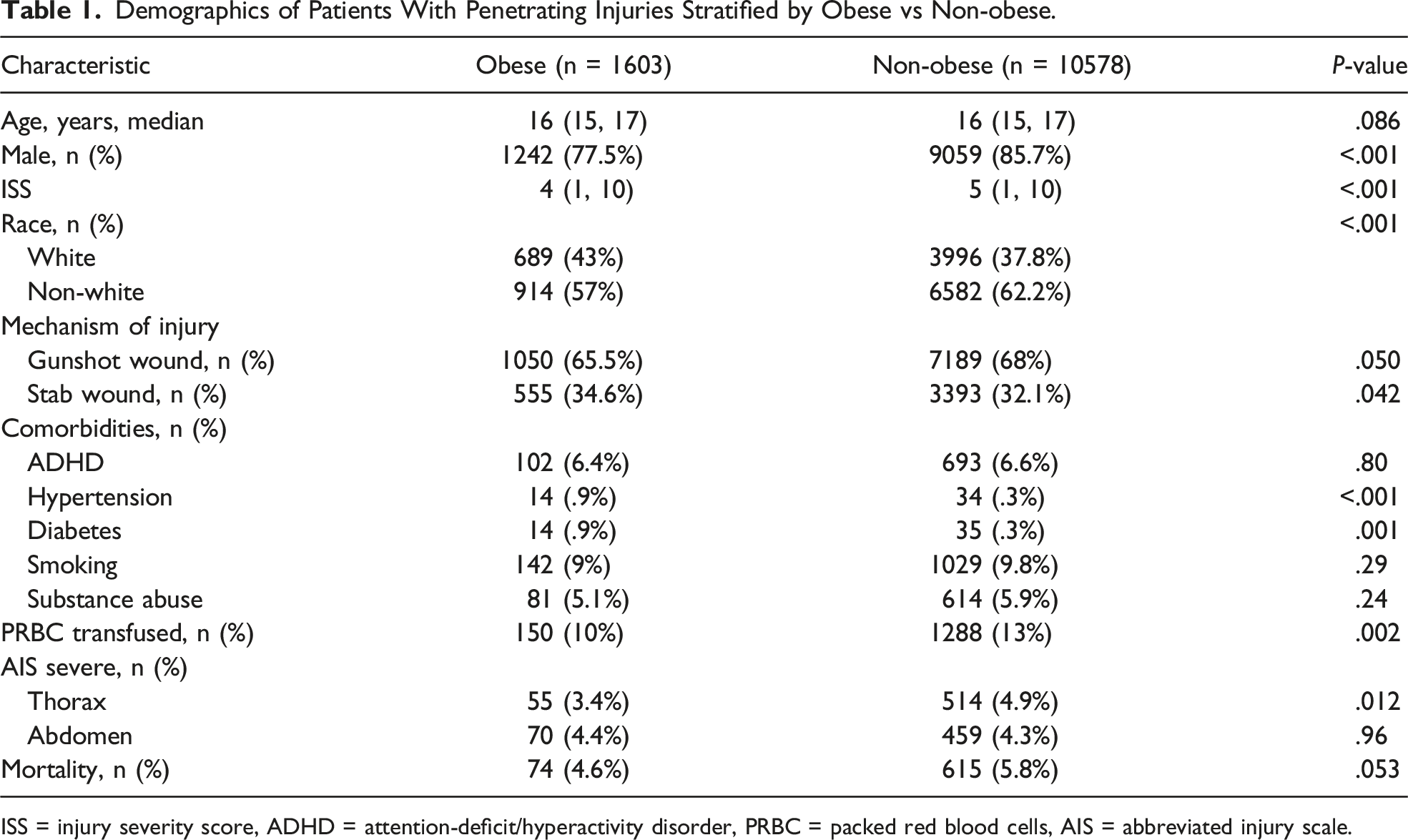
ISS = injury severity score, ADHD = attention-deficit/hyperactivity disorder, PRBC = packed red blood cells, AIS = abbreviated injury scale.
Clinical Outcomes of Patients With Isolated Thoracic Injuries Caused by Gun and Stab Wounds, Stratified by Obese vs Non-obese.
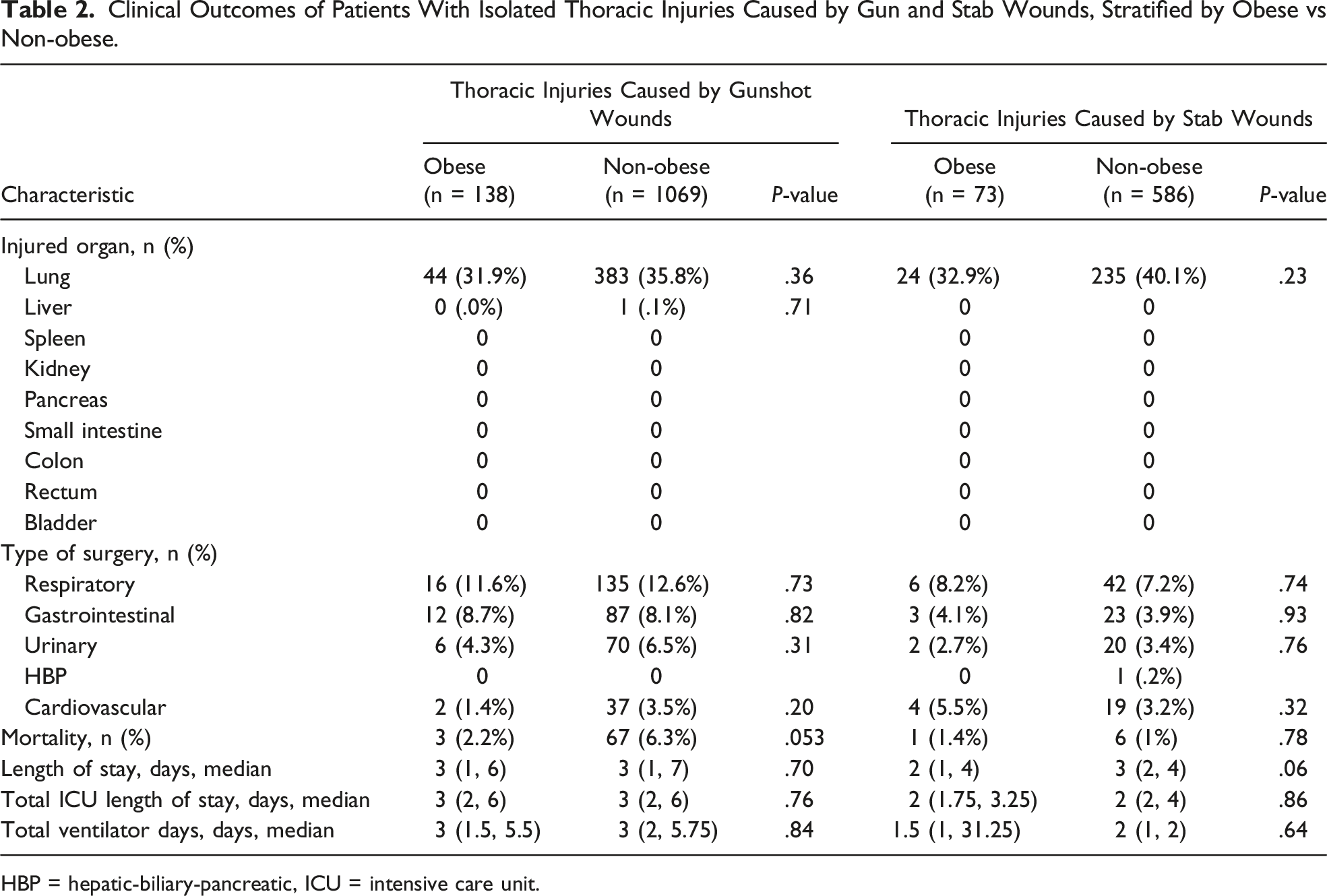
HBP = hepatic-biliary-pancreatic, ICU = intensive care unit.
Outcomes for Adolescent Trauma Patients With Isolated Thoracic Injury
Adolescents with obesity sustaining gunshot wounds had a lower rate of severe thoracic injuries (5.1% vs 13.4%, P = .005) compared to patients without obesity. However, adolescents with obesity presenting after a gunshot wound with isolated thoracic injuries had a similar rate of mortality (2.2% vs 6.3%, P = .053) median LOS, ICU LOS, and ventilator days (all P > .05).
Adolescents with obesity with isolated thoracic injuries caused by stab wounds had a similar rate of severe thoracic injury (13.7% vs 8.9%, P = .183) and mortality (1.4% vs 1%, P = .78), compared to patients without obesity. Adolescents with and without obesity sustaining isolated thoracic gunshot wounds also had a similar median LOS, ICU LOS, and ventilator days (all P > .05). (Table 2).
Outcomes for Adolescent Trauma Patients With Isolated Abdominal Injury
Adolescents with obesity with isolated abdominal gunshot wounds had a similar rate of severe abdominal injuries (12.1% vs 10.2%, P = .46) and mortality (1.2% vs 1.9%, P = .53) compared to patients without obesity. Both groups also had a similar median LOS, ICU LOS and ventilator days (all P > .05).
Clinical Outcomes of Patients with Isolated Abdominal Injuries Caused by Gun and Stab Wounds, Stratified by Obese vs Non-obese.
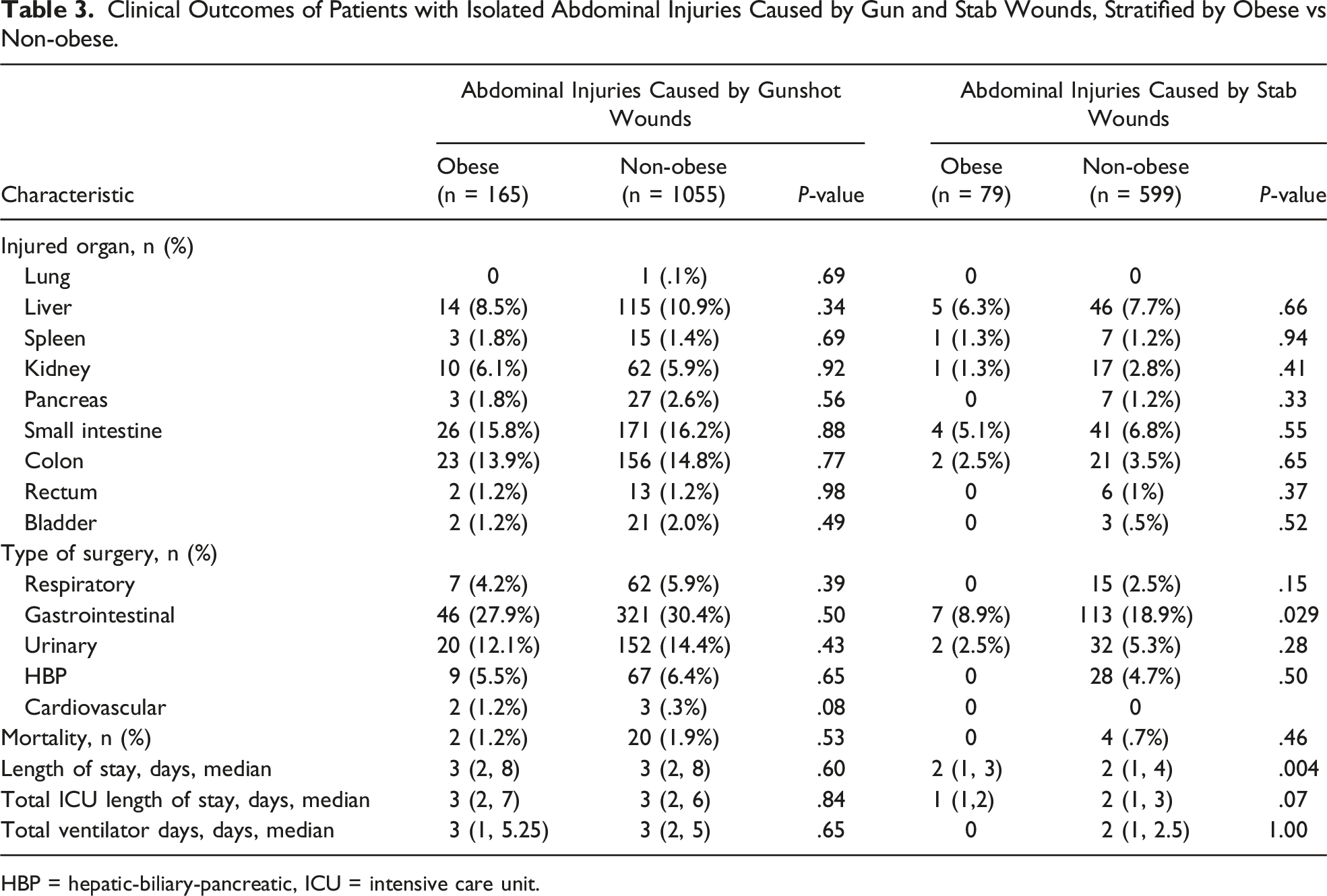
HBP = hepatic-biliary-pancreatic, ICU = intensive care unit.
Discussion
The effect of obesity in penetrating trauma is still controversial. With an alarming increase in the prevalence of obesity in adolescents, it is imperative to understand injury patterns in this population to guide workup and treatment algorithms. This national analysis found that adolescent patients with obesity had a significantly lower rate of isolated severe thoracic injury caused by gunshot wounds, but a similar rate of severe thoracic injuries caused by stab wounds. In addition, there was also a similar rate of severe isolated abdominal injuries caused by gunshot or stab wounds. Also, all populations studied had similar rates of mortality for adolescent trauma patients with and without obesity.
There are few studies comparing obese vs non-obese penetrating trauma.13-18 Furthermore, most studies in general evaluating obesity exclude patients less than 18 years old and focus on blunt trauma outcomes.3,5,6,15,16 In adult patients sustaining abdominal stab wounds, Bloom et al found decreased rates of peritoneal violation, severity of abdominal injury, and ISS with increasing BMI. In fact, patients in the thinnest group required an operation three times more often than those in the most obese category (BMI <18.5, 67% vs BMI >35, 20%, P = .03). 14 Patel et al also reported that adult (>16 years of age) patients with obesity were less likely to have abdominal fascial penetration and sustained fewer visceral injuries compared to overweight and normal weight cohorts. 17 That said, adolescent firearm injuries are increasing and now comprise the most common cause of injury-related death in this population. 19 Similar to adults, Castle et al performed a retrospective review of the National Trauma Data Bank and found a lower rate of operation needed for overweight and pediatric patients with obesity (ages 2-18 years old) sustaining penetrating thoracoabdominal trauma. However, they did not perform separate analysis regarding the mechanism of injury (eg, gunshot vs stab wounds) and location of injury. 12 In furtherance of these findings, this current study found that specifically, adolescents with obesity with isolated thoracic injuries caused by gunshot wounds had a lower rate of severe injuries. This is the first study to the knowledge of these authors to evaluate the “armor effect” in an adolescent population and may be helpful for providers when considering the possibility of tangential injury if clinically appropriate.
Mortality is obviously an important outcome and is also truly objective. In regards to adult penetrating trauma, Osborne et al found similar mortality between obese (BMI >30) and non-obese (BMI <30) patients in a limited sample size of 132 subjects. 6 Drury et al compared three BMI groups (normal weight, overweight, and obese) in adults who suffered either blunt or penetrating trauma, and although not statistically significant, the authors highlight that the overweight BMI group had the lowest mortality rate while the normal BMI group had the highest mortality rate. 16 In contrast, Owattanapanich et al studied isolated abdominal injuries caused by gunshot wounds in patients ≥16 years old, comparing patients with BMI >30 (obesity) vs patients BMI <30. Patients with obesity had increased mortality (6.5% vs 4.2%, P = .010) as well as hospital length of stay, ventilator days, and hospital acquired pneumonia. On subsequent multivariate logistic regression, obesity was independently associated with increased mortality (OR, 1.636; P = .021). 13 In contrast, this current national analysis of adolescents found a statistically similar rate of mortality after isolated thoracic and abdominal trauma caused by gunshot or stab wound. A possible explanation for the differences in outcomes between our study and the previously presented study is the patient population investigated. Our study analyzed a younger cohort, which despite having obesity, has not had the time to develop obesity-related medical complications from diabetes and/or metabolic syndrome. Thus, they may receive the armor effect (protective effect of having increased truncal mass to prevent internal injury) without the detriment of the long-term metabolic complications associated with obesity.
As a large retrospective database study, there are inherent limitations to this study including coding errors, missing information, and reporting bias. Additionally, given the retrospective design, the findings cannot be interpreted as causation and serve primarily to establish correlation and warrant further exploration. Furthermore, the use of BMI as a surrogate for estimating body fat and thus obesity is an important limiting factor as well. Although BMI is widely accepted and is the most readily available tool for stratifying patients by weight, it is truly excess body fat rather than the excess weight that correlates with ill-health. Given that BMI is calculated based on just height and weight, it fails to account for other factors like age, sex, and muscularity that play a role in determining a patient’s body fat. 20 In addition, the notably unstandardized fashion in which height and weight are collected across the country is an important limitation. Many trauma centers directly measure these values; however, it is possible that using bed weights which may include clothes or other objects and skew weight data. Furthermore, other trauma centers may rely on self-reported values or estimates. Despite these limitations, this study is strengthened by its large national population.
Conclusion
This analysis, spanning three years of data from the TQIP database, demonstrated that adolescent trauma patients with obesity presenting after isolated thoracic or abdominal knife wounds had similar rates of severe injuries and mortality compared to adolescents without obesity. However, adolescent patients with obesity presenting after an isolated thoracic gunshot wound had a nearly 25% relatively lower rate of severe injury. As such, trauma providers should consider this information when making emergent decisions regarding the work-up and treatment of firearm injuries in adolescent trauma patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.