
Abstract
Background
The proportion of older patients on the liver transplant waitlist continues to increase. With limited existing data to guide liver transplant evaluation of elderly patients, we aimed to study selection practices and outcomes of patients ≥70 years old. We hypothesized that 1-year patient and graft survival would not differ between appropriately selected elderly patients and those who are younger.
Methods
All patients referred for liver transplantation between 2018 and 2020 were stratified into elderly (age ≥70) and young (age <70) cohorts. Evaluation data pertaining to medical, surgical, and psychosocial risk assessment were reviewed. Recipient characteristics and post-operative outcomes, primarily 1-year graft and patient survival, were compared, with a median follow-up of 16.4 months.
Results
322 patients underwent transplant out of 2331 referred. Elderly patients represented 230 of these referrals and 20 underwent transplant. The most common reasons for denial of elderly patients were multiple medical comorbidities (49%), cardiac risk (15%) and psychosocial barriers (13%). The median MELD of elderly recipients was lower (19 vs 24, P = .02), and proportion of hepatocellular carcinoma was higher (60% vs 23%, P < .001). There was no difference in 1-year graft (elderly 90.9% vs young 93.3%, P = .72) or patient survival (elderly 90.9% vs young 94.7%, P = .88).
Discussion
Liver transplant outcomes and survival are not affected by advanced age in carefully evaluated and selected recipients. Age should not be considered an absolute contraindication for liver transplant referral. Efforts should be made to develop guidelines for risk stratification and donor–recipient matching that optimize outcomes in elderly patients.
Key Takeaways
Despite a growing demand for liver transplantation in older patients, many are excluded from referral and/or waitlisting due to concerns about comorbidity burden and general frailty. Judicious selection of elderly candidates for transplant results in outcomes equivalent to that seen in younger patients, including rates of major complications and 1-year graft and patient survival. With optimized selection through development of pre-transplant guidelines specifically for elderly patients in need of liver transplants, we can continue to meet the needs of this cohort.
Introduction
Liver transplant (LT) is the only curative treatment for end-stage liver disease. The shortage of organs and the complexity of LT has necessitated selection criteria, of which advanced age has historically been an absolute contraindication. Progress in perioperative and surgical care of LT recipients has permitted transplantation in increasingly older patients with acceptable outcomes. However, there is no well-defined acceptable recipient upper age limit. Amidst this debate, the current transplant waitlist is older than it has ever been despite a relative stability in length. At the end of 2020, 21.7% of the adult waiting list was 65 years or older, a marked increase from 9.4% in 2010. 1 As the population ages and life expectancy increases, the need for LT continues to grow among elderly patients.2,3
Recipient age has not been established as an independent risk factor for poor outcomes,4-6 and morbidity in elderly patients undergoing LT is often attributed to medical comorbidities and poor physical function. Post-transplant mortality is greater in all-comers with low body mass index (BMI), 7 cardiovascular disease, 8 coronary artery disease (CAD), diabetes, chronic obstructive pulmonary disease (COPD), and chronic kidney disease (CKD). 9 Frailty, the physiologic decline commonly associated with advanced age, can prognosticate need for delisting and 90-day mortality in transplant candidates. 5 This is closely tied to malnutrition and may present as underweight BMI (<18.5), muscle wasting, and weight loss; however, nutrition status may be masked by ascites and obesity. Discerning selection of older patients without these risk factors is at the crux of more favorable outcomes.
The lack of established guidelines for judicious patient evaluation and selection of elderly patients has led to high variability in center-specific selection criteria. We aimed to study specific selection practices and outcomes of patients ≥70 years old undergoing LT. We hypothesized that 1-year graft and patient outcomes would not differ between well-selected elderly patients and their younger peers.
Methods
Patients referred for LT between January 1, 2018 and December 31, 2020 were retrospectively identified using a single center institutional transplant database. Patients were divided into 2 cohorts based on age at time of referral, an “elderly” group (age ≥ 70) and a “young” group (age < 70). Baseline demographics included sex, race, laboratory MELD score, presence of specific complications of cirrhosis, pre-operative functional status, pre-transplant dialysis, ICU admission, or mechanical ventilator, anatomic and surgical factors including multi-organ transplant, presence of portal vein thrombosis, prior abdominal surgery or TIPS, and time to transplant. Donor characteristics including cold ischemia time and donor risk index (DRI) were also collected. DRI is a metric of donor quality which helps predict graft failure after LT and utilizes 7 risk factors, which include age, height, race, donor cause of death, DCD donor, partial/split liver graft, organ geographic location, and cold ischemia time. 10 Recipients were followed for a minimum period of 12 months. Institutional Review Board (IRB) exemption was obtained from our institution for this study including need for consent.
The primary outcomes were 1-year patient and graft survival. Secondary outcomes included intensive care unit (ICU) and hospital length of stay (LOS), respiratory failure rate (defined as the need for high flow nasal cannula or non-invasive positive pressure ventilation), rate of re-intubation, rate of major post-operative complications (ie, Clavien-Dindo grade ≥ III), and 30-day re-admissions. Pre-operative variables included recipient characteristics, laboratory model for end-stage liver disease (MELD) score, end-stage liver disease complications, pre-transplant dialysis or ventilator need, time to transplant, and poor functional status (based on the Karnofsky Performance Status Scale). The Karnofsky Performance Status Scale measures functional status on an 11-point scale ranging from 100% (no symptoms) to 0% (death), based on a patient’s ability to carry out their normal work and activities, the presence of symptoms, need for assistance, or how much time is spent bed-bound. 11
For univariate analyses, a comparison of continuous variables was done using the Mann-Whitney U test and Student’s t test as appropriate. The Pearson chi-squared coefficient was applied to categorical and binary data elements with Fisher’s exact test used where appropriate. Variables were identified as parametric or non-parametric using the Shapiro-Wilk test where a P > .05 identified a normally distributed sample. Median values with interquartile ranges (IQR) were reported for non-parametric continuous variables and mean values with standard deviations were reported for parametric continuous variables. A P < .05 was considered statistically significant. Kaplan-Meier survival analysis was used to compare 1-year patient and graft survival rates. All analyses were performed using Stata 15 (StataCorp, College Station, TX).
Results
Elderly Patient Selection Criteria
230 elderly patients were referred during the study period; about two-thirds (153; 67%) were found ineligible, primarily due to multiple medical contraindications (23%), patient choice (18%), low MELD or “too well” for LT (13%), financial/insurance complications (7%), and patient death (6%) (Figure 1). Transplant evaluation was completed in the remaining 77 patients, with selection criteria defined in an ad hoc fashion; 33 (43%) patients were declined, 32 (42%) were listed for transplant, and 12 (16%) were still undergoing work-up. At the end of the study period, 20 of the waitlisted patients had undergone transplant (62.5%), 7 remained active on the waitlist (22%), 1 was inactive due to COVID-19 infection (3%). Notably, 4 patients (12.5%) had been removed from the waitlist due to clinical deterioration, either from advancement of malignancy or worsening of other medical comorbidities, namely CAD, CKD, pulmonary hypertension, or sepsis. Outcomes of liver transplant referrals made for elderly patients between 2018 and 2020.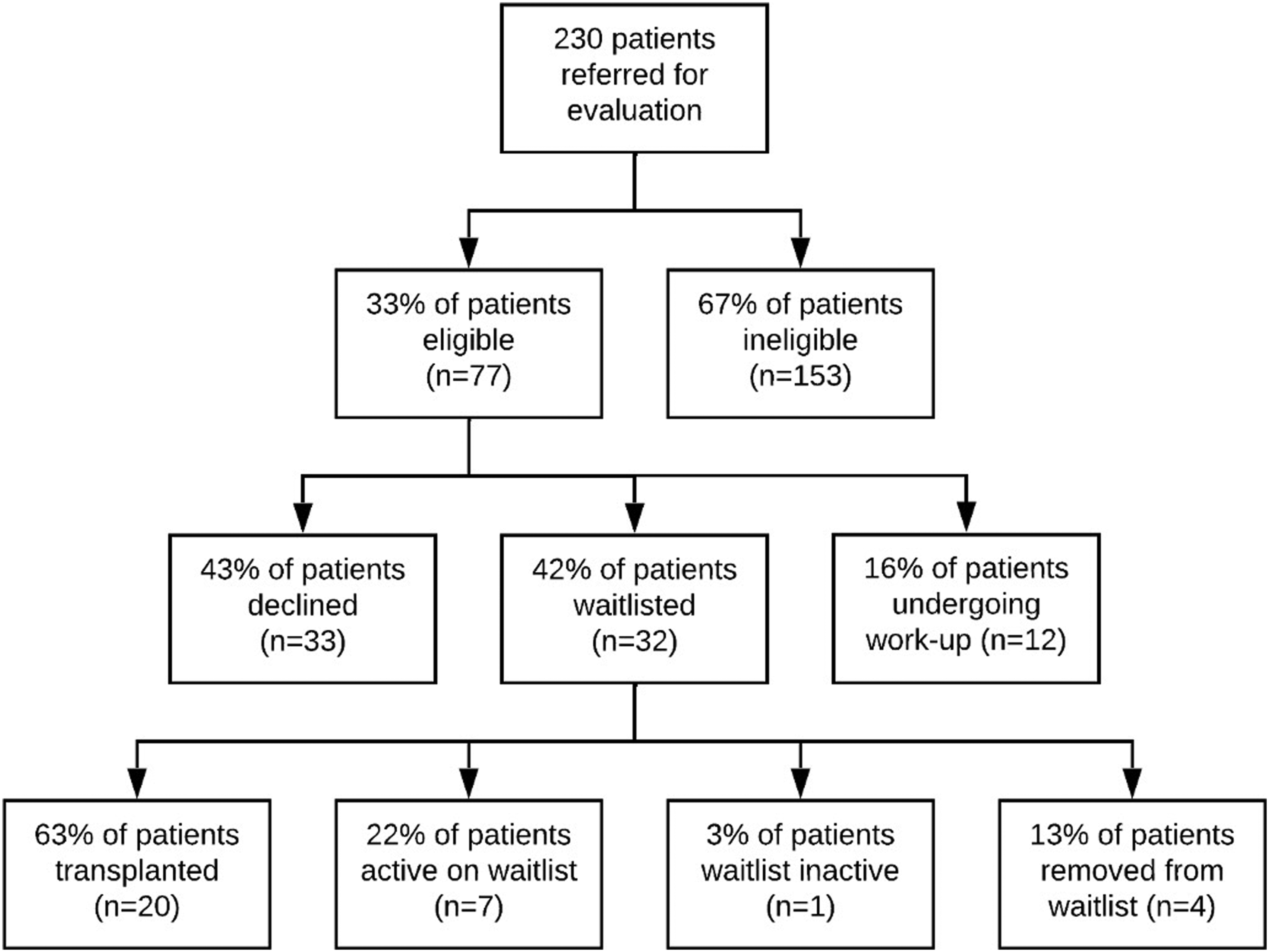
Reasons for denial in the 33 patients deemed eligible at referral varied. Severity of medical co-morbidities and patient deterioration during the evaluation phase were most common, representing 33% and 24%, respectively. The remaining patients died during the evaluation period (9%), had malignancies too advanced for transplant to be curative (6%), elected not to undergo transplant (6%), had improvement in their condition no longer warranting transplant (6%), or lacked sufficient social support (3%).
Elderly patients who underwent LT and those that were declined had similar medical problems, including CAD, CKD, type 2 diabetes, COPD, and atrial fibrillation. However, these comorbidities were well-controlled and stable, that is, without acute exacerbations or related hospitalizations while awaiting transplant. Cardiac risk was assessed in all evaluated patients, with dobutamine or exercise-induced stress test if indicated, particularly in patients with hyperlipidemia, hypertension, diabetes, or smoking history. Based on the results of non-invasive tests, selected candidates underwent coronary angiogram to diagnose and treat intervenable obstructive coronary artery lesions. Abnormal findings that often-precluded transplant in this population included frequent premature ventricular contractions, substantial wall motion defects, stress-induced ST depressions, chest pain, tachypnea, or hypoxia during stress testing, and significant coronary occlusion on cardiac catheterization. Pulmonary evaluation was also performed on a case-by-case basis, with 6-minute walk or pulmonary function testing (PFT). A reduced 6-minute walk distance (<400 m) or PFT abnormalities (reduced forced vital capacity, forced expiratory flow and volumes, etc.) were among findings present in patients denied for transplant.
Patient and Donor Characteristics
Comparison of Liver Transplant Recipient and Donor Characteristics in Young (Age <70 Years Old) and Elderly (Age ≥70 Years Old) Cohorts.
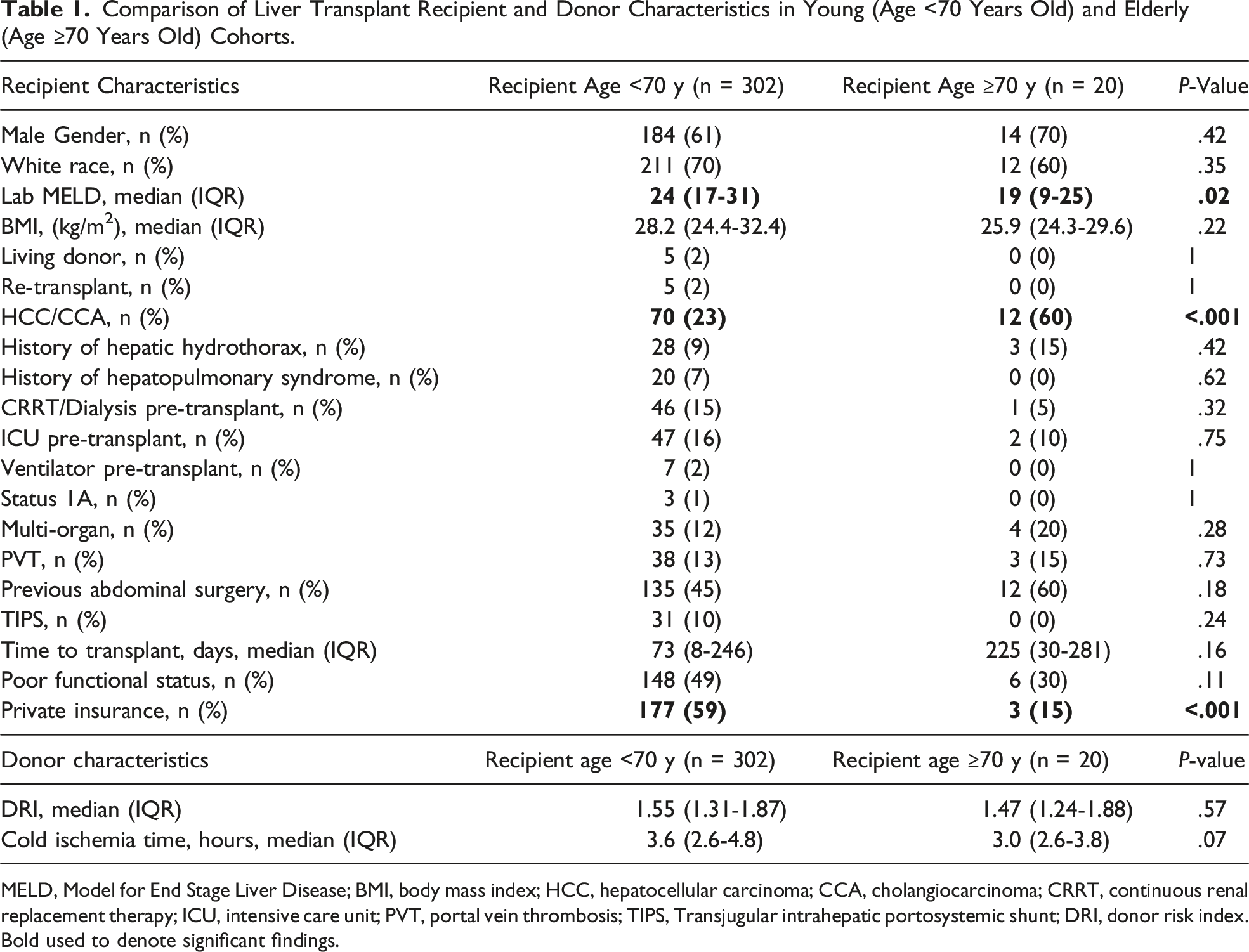
MELD, Model for End Stage Liver Disease; BMI, body mass index; HCC, hepatocellular carcinoma; CCA, cholangiocarcinoma; CRRT, continuous renal replacement therapy; ICU, intensive care unit; PVT, portal vein thrombosis; TIPS, Transjugular intrahepatic portosystemic shunt; DRI, donor risk index. Bold used to denote significant findings.
Post-Operative Outcomes
Comparision of Post-Operative Outcomes of Young (Age <70 Years Old) and Elderly (Age ≥70 Years Old) Patients Undergoing Liver Transplant.
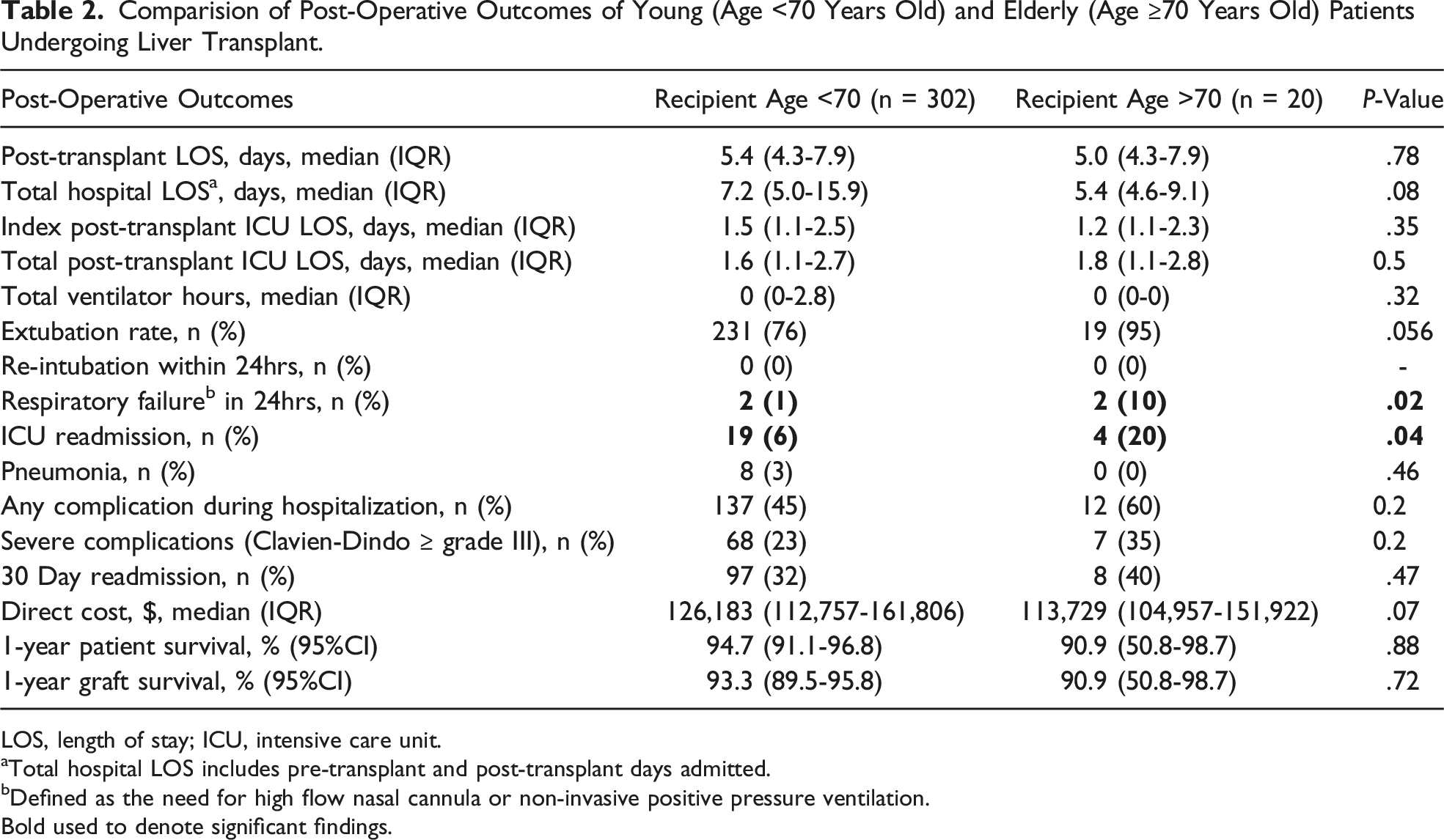
LOS, length of stay; ICU, intensive care unit.
aTotal hospital LOS includes pre-transplant and post-transplant days admitted.
bDefined as the need for high flow nasal cannula or non-invasive positive pressure ventilation. Bold used to denote significant findings.
Discussion
In this study, advanced age alone was not a significant risk factor for poor patient or graft outcomes in LT recipients. Specifically, age ≥70 years did not lead to differences in 1-yearpatient and graft survival, or worsening of secondary post-operative outcomes including hospital or ICU LOS, in-hospital complications, or Clavien-Dindo complications ≥ grade III. Despite higher rates of post-operative high flow nasal cannula or non-invasive positive pressure ventilation, elderly patients had higher primary extubation rates (95% vs 76%, P = .056) and furthermore, none required re-intubation. An increased rate of ICU re-admissions was observed and was likely in part due to a lowered clinical threshold to transfer elderly patients to a higher level of care.
Within a conflicted body of literature, our findings support the cautious transplantation of well-selected elderly patients. Wilson et al came to similar conclusions in one of the largest US multicenter studies of elderly LT patients. In their case-controlled analysis, recipient age was not identified as an independent risk factor for graft loss or patient mortality at 5-year follow-up. 12 However, other studies have failed to come to the same conclusion. For example, Sharpton et al found that age was associated with 1-year graft loss, though elderly graft loss was attenuated at lower MELD scores. 13 Significantly lower 5-year survival rates in patients over age 70 were reported by Sharma et al based on 2002-2012 UNOS data, 14 and studies from Chen et al and Gil et al have reported similar findings in Taiwanese and Korean populations, respectively.15,16 A more recent systematic review and meta-analysis of 10 studies including 4,752 elderly (age ≥70) LT recipients demonstrated higher perioperative mortality and graft failure in this population, though with considerable heterogeneity noted upon analysis. 17 Whether this variance across studies stems from center-specific factors, progressive improvements in surgical and intensive care over the last decade, or a wide variation in selection practices and patient populations, it underlines that advanced recipient age should not be an absolute contraindication for referral or transplant without characterization of physiologic age.
Over the last several years, many physical frailty screening tools have been developed to better objectively assess patient physiologic age and medical vulnerability. Common factors of these measures include recent weight loss, diminished capacity for physical activity, and presence of certain chronic illnesses. In addition, sarcopenia, or the loss of muscle mass and skeletal strength, is central to the functional decline seen in older adults and can also be objectively accounted for. In patients awaiting LT, frailty has been firmly established as an independent risk factor for poor outcomes. Post-transplant patients with higher Liver Frailty Index scores had higher morality rates and health care utilization costs, including hospital length of stay and non-home discharge. 18 Measurement of frailty provides rich data regarding functional status and suitability for transplantation more than chronologic age, and should be part of the work-up for all transplant candidates, especially those who are older.
We found elderly patients were more likely to undergo LT for malignancy, representing 60% of our elderly study population in comparison to 23% of younger patients. While locoregional therapies exist for hepatocellular carcinoma (HCC), some patients may not be eligible due to tumor distribution or burden, or underlying cirrhosis. Recent data from Shah et al reported a survival advantage for elderly patients with HCC undergoing LT vs liver-directed therapy alone. 19 Patients undergoing LT had more significant comorbidities and higher MELD scores, and yet 5-year survival rates in the LT group were 70% compared to 31% in the directed therapy group. This study also found a yearly 3% increase in risk of mortality in patients over age 70 regardless of treatment option. Taken together these findings emphasize that while LT is beneficial in these patients, careful counseling of elderly patients prior to listing remains paramount.
While many patients may be adequate candidates at the time of initial evaluation, an extended waiting period prior to LT may result in changes to clinical status, especially in older patients. In our study, elderly patients waited almost three times as long for LT (225 vs 73 days). This longer wait for elderly patients has been seen across centers and regions, and likely due to lower MELD scores, with higher rates of HCC and preserved liver function. Almost one-third of the current waitlist is over age 65, and increased wait times may challenge the feasibility of LT and necessitate removal in declining patients. 20 Thus, optimizing outcomes in elderly patients requires appropriate selection and ongoing re-evaluation. Specifically, older patients should be held to more rigorous and stringent selection criteria than their younger peers who may be listed with higher MELD scores as they typically have less physiologic reserve. Gilbo et al found elderly patients to have a low-risk profile when they demonstrated a more stable disease, that is, HCC within Milan criteria, lower MELD (<15), and not admitted to the ICU or on continuous renal replacement therapy prior to organ offer. However, the only significant predictor of poor patient survival was hospitalization in the ICU prior to LT. 21
Limitations of this study include sample size and the single-institution population. Additionally, it is important to note that although it is now a standard practice at our institution, during the study period we did not conduct a formal frailty or sarcopenia assessment in our patient cohorts. Lastly, due to a median overall follow-up time of 16.4 months, we were unable to examine more remote metrics such as 5-year outcomes, which are critical to understand the benefits and durability of LT in this population. Despite this, because of the paucity of granular data on patients over age 70 in the literature, this study addresses gaps and helps inform selection guidelines in these patients.
Many questions remain unanswered with regards to liver transplantation of elderly recipients. Indeed, the burden of overall medical comorbidities, frailty, and nutritional status should be objectively assessed, and multidisciplinary judgment applied in determining if LT is likely to confer survival benefit to a patient. This includes the potential utility of pre-habilitation protocols in expanding indications and even further improving outcomes of this higher risk group of patients. Considering our finding of a correlation between age of recipients, ICU readmission, and respiratory failure, dedicated post-operative protocols to help mitigate these risks are being established. Importantly, as most research has been focused on graft and patient survival rather than the quality of life after transplant, further investigation into this as well as functional status remains imperative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.