
Abstract
The management and outcomes for patients with metastatic melanoma have been revolutionized by immunotherapy. This case report highlights the role of surgery as an adjuvant to systemic therapies when there is oligoprogressive disease. We describe a 74-year-old man with metastatic melanoma who initially had a complete radiographic response after dual agent immunotherapy but subsequently developed a large metastasis in the retroperitoneum. After multidisciplinary discussion, he underwent margin negative resection that required en bloc segmental resection of the infra-renal inferior vena cava. To our knowledge, this is the first reported resection of a melanoma metastasis in this location.
Keywords
Since 2010, immunotherapy has revolutionized the treatment of metastatic melanoma. These new therapies, including ipilimumab, an anti–cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) monoclonal antibody, and anti–programmed death 1 agents (nivolumab and pembrolizumab), have been shown to substantially increase survival. Combination therapy, particularly of ipilimumab and nivolumab, is now a standard treatment for advanced melanoma, with five-year overall survival rates of 30-50%. 1 Even in the face of widespread metastatic disease, durable disease control, even complete responses, may be achieved. Thus, the role of surgery for advanced melanoma is undergoing a paradigm shift, with the emergence of metastatectomy for single or oligo-progressive disease in carefully selected patients.
This case report highlights the role of surgery as an adjuvant to systemic therapies when there is a single site of progressive metastasis.
A 74-year-old male was diagnosed with cutaneous melanoma of the left upper posterior arm in 2015, which was managed with wide local excision and axillary lymph node dissection. Final surgical pathology revealed a pT2a N1a, resected with negative margins. He remained asymptomatic until 2018 when he presented with weight loss and melena. Workup revealed metastatic melanoma involving the lung and multiple inguinal and retroperitoneal lymph nodes. He was treated with immunotherapy (ipilimumab and nivolumab) and had a complete radiographic response. However, six months later, it recurred in the retroperitoneum, and this single site of disease continued to enlarge despite continued immunotherapy. The progressive disease reached 10 cm in maximal dimension and encased the inferior vena cava (IVC, Figure 1). Coronal computed tomographic imaging showing the retroperitoneal mass and its adjacent structures.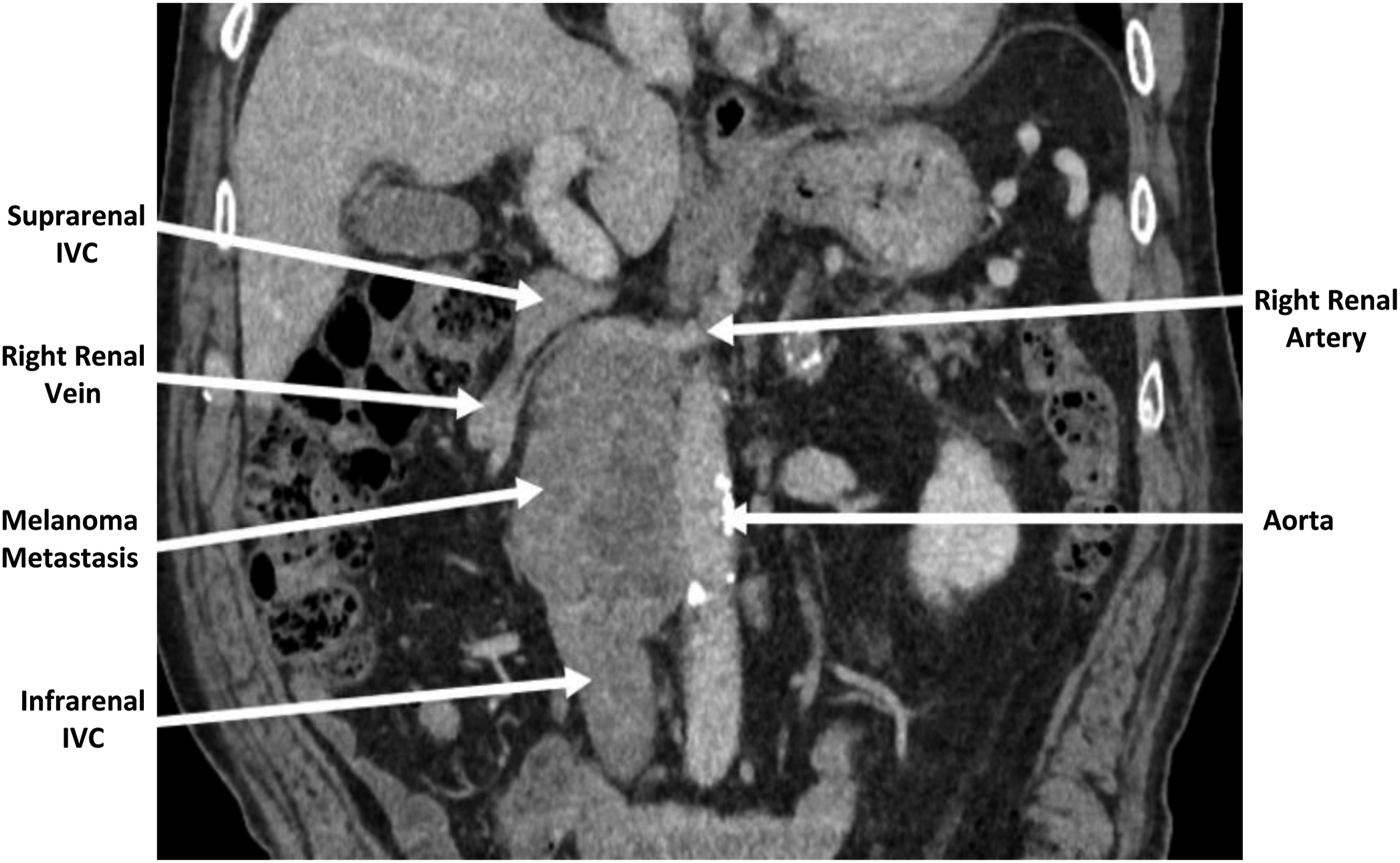
After multidisciplinary discussion, resection of this single site of progressive disease was recommended. At operation, exploration first confirmed that there were no other sites of metastasis. A right-sided visceral rotation fully exposed the retroperitoneal mass. The mass was densely adherent to the IVC but not invading the aorta or right kidney. En bloc resection of the mass with a short segment of the IVC was performed. The IVC was reconstructed with a synthetic tube graft (Figure 2). The patient had an uneventful recovery and was discharged home on aspirin and atorvastatin on postoperative day six. The final pathology report showed metastatic melanoma with the confirmation of negative margins. The patient continues to do well six months postoperatively. (A) Right retroperitoneal mass. (B) Operative field after reconstruction of the IVC.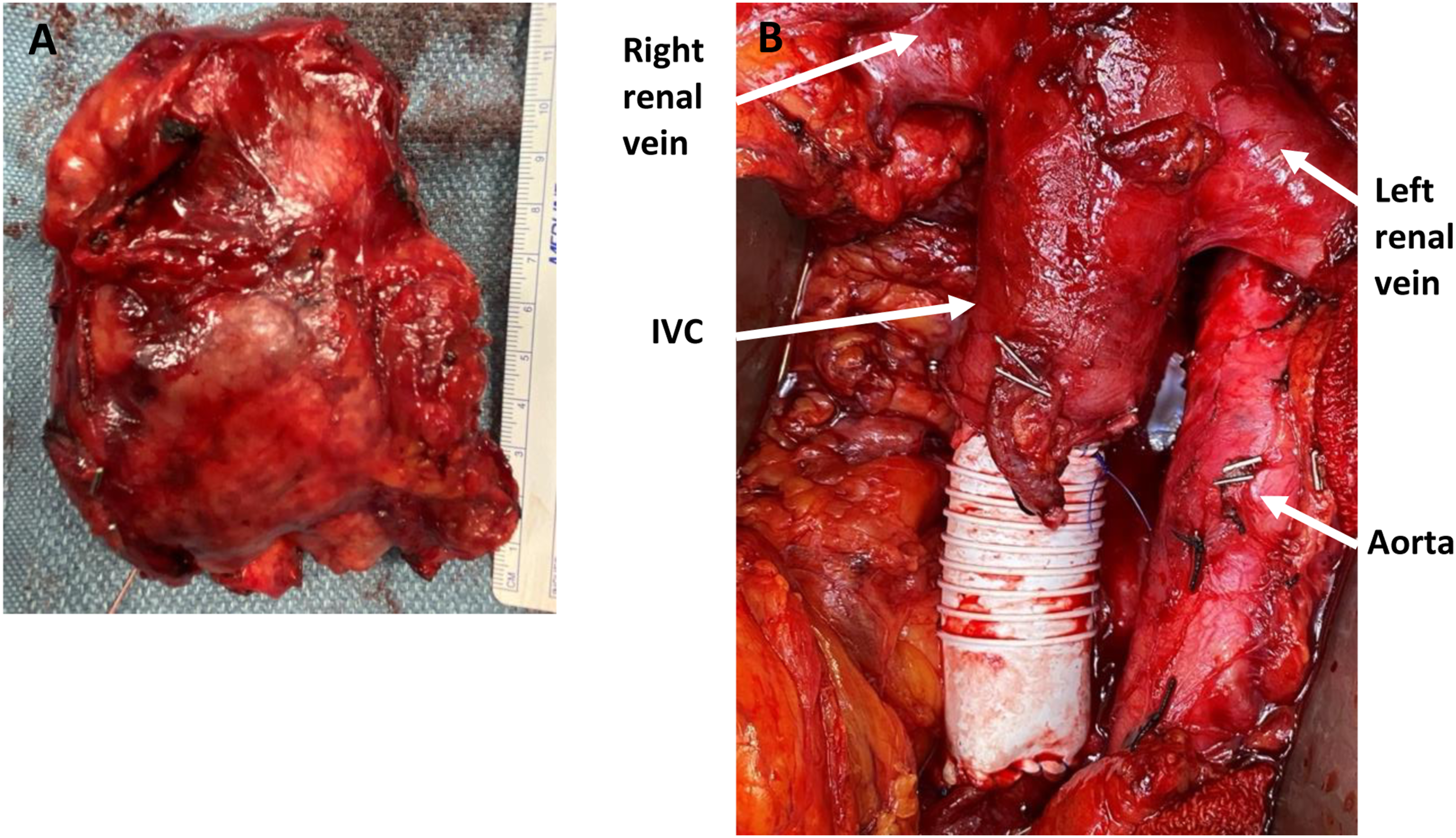
We present a case report in which a 74-year-old man underwent resection of single site of melanoma metastasis that was progressing on immunotherapy. Complete gross resection of the retroperitoneal metastasis required en bloc resection of a portion of the IVC.
Metastasis to the retroperitoneum is rare—in fact, we were unable to find a published case of a melanoma metastasis to the retroperitoneum being resected. Metastases to rare sites are more likely to occur in conjunction with metastases to other, more common sites. Thus, for example, there is a wealth of published data about the role of resection for melanoma metastases to the lung, the small bowel, and the liver. 2 These retrospective data show that in carefully selected patients, complete resection of all metastatic disease is associated with durable palliation and survival benefit. In this era of immunotherapy and targeted therapy for melanoma, a new indication for surgical resection is the presence of oligoprogressive disease. 3 Such oligoprogressive metastases have developed resistance to targeted therapies or immune “escape.”
General recommendations regarding how to best select patients for local therapies (especially surgical resection) include multidisciplinary discussion that considers duration of disease-free interval and relative disease stability on systemic therapy, rate of growth of oligoprogressive sites, performance status, and magnitude of the operation (in terms of complications, length of postoperative recovery and quality of life, and how long the patient will be off systemic therapy).
In terms of the technical details of this operation, the preoperative imaging showing severe deformity of the IVC by the tumor made us very suspicious that en bloc IVC resection would be necessary to achieve complete gross resection of the tumor. Reconstruction of the IVC with an interposition graft at our center is a routine procedure with low morbidity, and in cases where there is not complete IVC obstruction, can reduce the incidence of postoperative lower extremity edema. 4 The high flow rate through the IVC means that postoperative therapeutic anticoagulation is not necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.