
Abstract
Tracheostomy for prolonged ventilation of patients with COVID-19 was often delayed due to high viral loads and persistent high ventilatory requirements. With prolonged intubation and significant dose corticosteroid use, patients with COVID-19 are at risk for tracheomalacia, and urgent tube exchange may be required to address persistent cuff leak and to maintain adequate mechanical ventilation. We sought to describe our single center experience with COVID-19 patients requiring tracheostomy and the tracheal complications that followed. We performed a review of patients with COVID-19 who underwent tracheostomy from June 2020 to October 2021. 45 patients were identified; 82.2% survived their index hospitalization. Tracheostomy was performed after 16.4 days of mechanical ventilation. 22.2% required urgent exchange to an extended length tracheostomy tube after 7.2 days from initial tracheostomy. Placement of an extended length tracheostomy tube can reduce cuff leak in ventilated COVID-19 patients and may be considered during initial tracheostomy placement.
Introduction
The 2019 coronavirus disease (COVID-19) resulted in a significant burden of respiratory failure, and many patients with COVID-19 required a prolonged course of mechanical ventilation. These patients are at an increased risk of complications related to time with an endotracheal tube, notably tracheomalacia. In addition to the prolonged mechanical ventilation times due to the severity of respiratory failure as well as concerns for health care worker exposure, patients with COVID-19 had multiple additional risk factors for the development of tracheomalacia. High-dose corticosteroid administration, a mainstay of early treatments for COVID-19, can lead to increased susceptibility to trauma from the endotracheal tube cuff and impaired tracheal healing.
For patients who underwent tracheostomy in the setting of COVID-19, prolonged mechanical ventilation, and the subsequent development of acquired tracheomalacia or other pathologies of the trachea (eg, tracheomegaly), resulted in a poor seal of the tracheostomy cuff to the trachea. 1 This poor seal prevents a ventilator from delivering adequate tidal volumes to the lungs while maintaining positive end-expiratory pressure (PEEP), and an urgent tracheostomy tube exchange may be required to maintain adequate oxygenation and ventilation. After we noted many patients with COVID-19 requiring urgent tracheostomy tube exchanges secondary to persistent cuff leak, we sought to describe our single center experience with COVID-19 patients requiring tracheostomy.
Methods
IRB approval was obtained for this study. This is a retrospective review of patients who underwent percutaneous tracheostomy at an academic medical center from June 2020 to October 2021. Patients were identified through a review of the electronic medical record (EMR). We identified patients undergoing tracheostomy who had a concomitant diagnosis of COVID-19 during the same admission. Demographic data were collected. Details regarding the procedure were collected, and the EMR was reviewed for subsequent complications related to the airway or tracheostomy, most notably need for urgent or emergent tracheostomy exchange. Descriptive statistics were performed.
Results
Patient Demographics and Procedure Details.
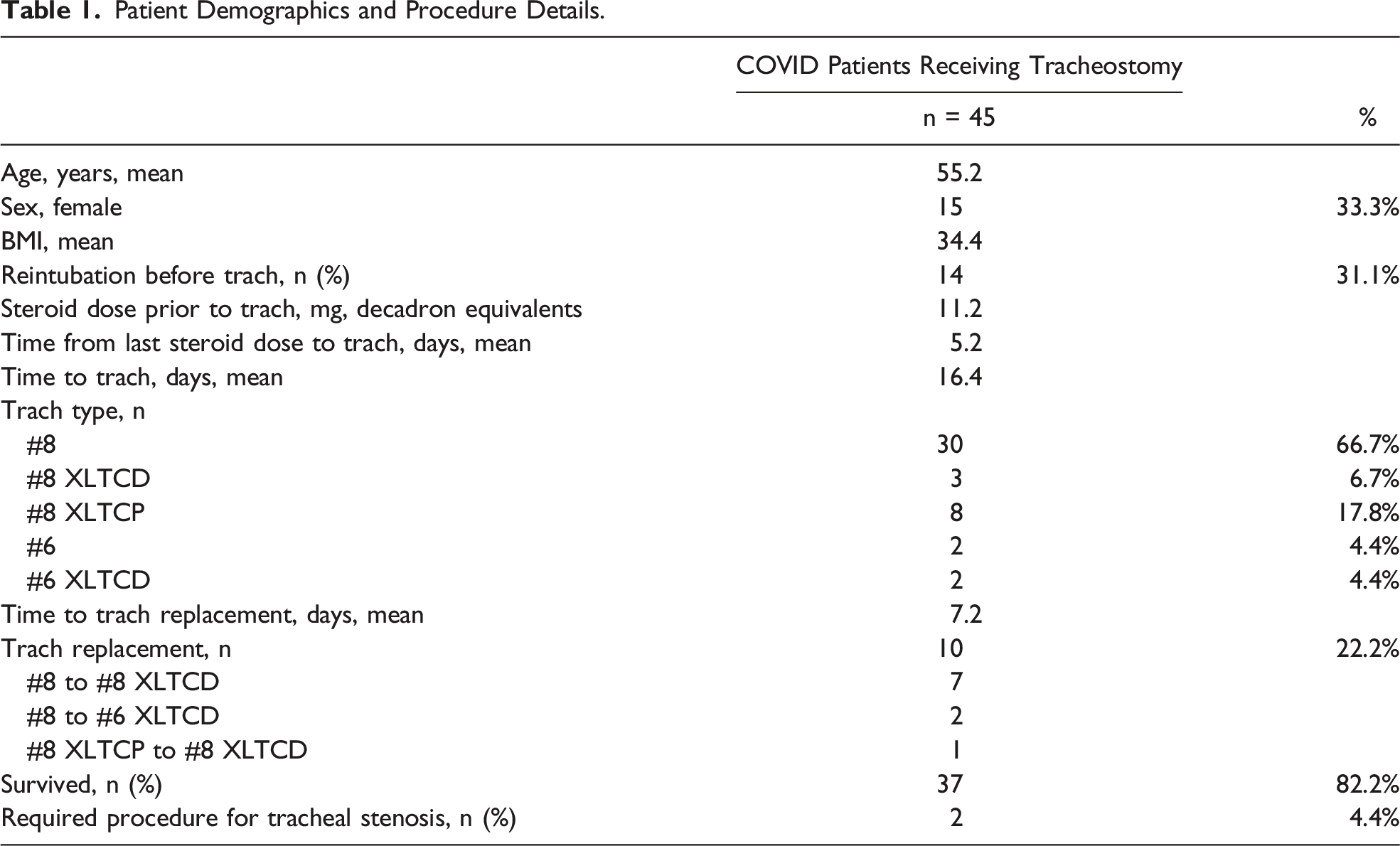
Tracheostomy was performed after 16 days (mean) of mechanical ventilation. Most patients (66.7%) had a standard length #8 Jackson-sized cuffed tracheostomy tube at the index insertion. Ten patients (22.2%) required urgent exchange of the tracheostomy tube at a mean of 7.2 days after initial insertion. All tracheostomy tube exchanges were to an extra length, distal tube. The survival rate to discharge was 82.2%. Two patients (4.4%) went on to require tracheal resection for tracheal stenosis.
Discussion
Acquired tracheomalacia and tracheal complications have been described for decades. The pathophysiology of acquired tracheomalacia is not well elucidated; however, endotracheal injury from inflated or hyper-inflated endotracheal tube cuffs as well as repeated injury from reintubations may have a role in the subsequent development of tracheomalacia.1,2 Continuous or repeated tracheal injury, resulting from endotracheal intubation or chronic cuff hyper-inflation, may lead to decreased perfusion and subsequent poor healing, resulting in compromised tissue integrity of the trachea. Loss of healthy tracheal tissue may lead to collapse of the airways or, conversely, an abnormal enlargement. In either circumstance or any cause of tracheal injury, the result is compromised tracheal tissue which makes maintenance of an effective seal from a cuff or balloon more difficult.
Many patients with COVID-19 required a prolonged course of mechanical ventilation via an endotracheal tube. Re-intubation of patients with COVID-19 was frequent, as many patients experienced improvement in their respiratory failure but subsequently had a pulmonary complication from a secondary bacterial pneumonia or other complications related to the debility from critical illness. One of the mainstays of early treatment for COVID-19 was glucocorticoid administration, and while this may have had a beneficial impact on treatment of the pneumonia, its immunosuppressive effects may also have impaired tracheal healing. Another factor that may contribute to the development of tracheomalacia is that endotracheal intubation often was extended before tracheostomy placement occurred in an effort to limit the procedure team’s exposure to high viral loads.
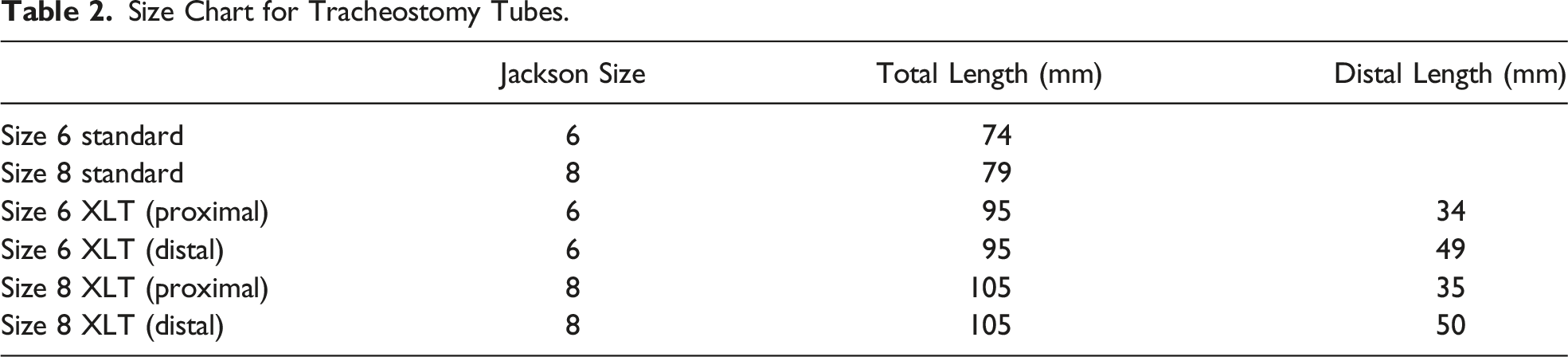
Size Chart for Tracheostomy Tubes.
In conclusion, there is a high rate of potentially life-threatening tracheal complications of prolonged mechanical ventilation in patients with COVID-19. Placement of an extended length tracheostomy tube can reduce cuff leak in ventilated patients, and use of the extended length tracheostomy tube at initial tracheostomy placement may reduce the need for urgent tracheostomy exchange.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.