
Abstract
Introduction
Decubitus ulcers are a morbid and costly problem faced by healthcare systems and patients across the country. We aim to examine current patterns and characteristics of patients admitted to the hospital with a pressure ulcer.
Materials and methods
From a nationally representative sample of hospital discharge records, the Nationwide Inpatient Sample (NIS), patients with a diagnosis of pressure ulcer 2008-2019 were identified. Patient volume, demographic and clinical data were analyzed for change over time.
Results
The volume of pressure ulcer patients as a proportion of all hospital patients remained constant from 2008 to 2019 (P = .479). During the study period, the proportion of ulcer patients that underwent an ulcer-related procedure significantly decreased (P < .001) while the proportion of ulcers considered severe significantly increased (P < .001).
Conclusions
Our analysis suggests the prevalence of decubitus ulcers remained stable during the time period, with increased severity but reduced frequency of operative intervention.
Key Takeaways
• Decubitus ulcers are a morbid and costly condition. Recent policy changes aim to decrease decubitus ulcer prevalence. • The Nationwide Inpatient Sample (NIS) was used to assess ulcer prevalence 2008-2019. • Despite policy changes, pressure ulcer prevalence remained stable, with increasing severity and decreasing rates of surgical intervention.
Introduction
Pressure injuries (PIs) are caused by unrelenting physical pressure damaging underlying tissue, particularly when soft tissue is compressed against a bony surface. Although most pressure injuries are preventable, 1 they remain a persistent source of morbidity and cost in the US. Treatment can be complex and associated with high recurrence rates – particularly in later-stage full-thickness wounds. 2 National cost estimates range from $3.3 billion 3 to $26.8 billion, 2 representing a significant expense to patients and the healthcare system as a whole. And the costs of management of this preventable disease continue to grow as technological advances in wound care and surgical technique arise. 2 Risk factors for pressure ulcers including immobility and malnutrition have previously been identified, particularly involving factors that impair the microcirculatory system. 4 The rate of pressure injury among critically ill patients is particularly high, at an estimated 14.3%, while the overall rate of hospital-acquired pressure injury is estimated to be 5.85%. 5
The incidence of decubitus ulcers has been established as a healthcare facility quality indicator, drawing increased attention to this disease. As the US healthcare system has moved toward quality measurements and performance incentives for healthcare institutions, several policy initiatives have addressed the need to prevent hospital-acquired conditions such as PIs. In 2008 the US Centers for Medicare and Medicaid Services (CMS) introduced a non-payment model for hospital-acquired conditions (HACs). 6 This was reportedly successful at reducing hospital-acquired pressure ulcer incidence at academic medical centers. 7 And in 2015, the CMS went a step further and implemented use of the Patient Safety Indicator 90 (PSI90) to adjust payments and score hospitals on quality. 8 The PSI90 is a composite rate of hospital-acquired conditions, including PI. This policy effectively penalized hospitals for high rates of selected hospital-acquired conditions. However, despite these incentives, pressure ulcers remain a significant burden on the US healthcare system. 9
In an effort to understand pressure ulcer prevalence and patient characteristics over time, this study examined the volume of pressure ulcer diagnoses among hospital admissions using the Nationwide Inpatient Sample (NIS) annually from 2008 to 2019. The NIS is a nationally representative sample of US hospital discharges, and provides information about patient demographic and clinical variables. The aim of this study was to report trends in pressure ulcer prevalence, as well as ulcer-related procedure prevalence, with respect to patient characteristics.
Methods
Database and Selection of Patients
In this retrospective analysis we conducted a cross-sectional study of hospital discharges in the United States using the 2008 through 2019 years of the Nationwide Inpatient Sample (NIS). The NIS is part of the Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality, 10 and is a 20%, representative sample of discharges from US hospitals, which is weighted to allow for national and longitudinal estimates. The database contains no direct patient identifiers and is consistent with a “limited data set” under the HIPAA Privacy Rule. Population estimates were obtained via incorporation of provided discharge weights.
From this database, patients over 18 years of age with an International Classification of Disease (ICD) 9 or ICD-10 diagnosis code indicating diagnosis of pressure ulcer were identified. As the change from ICD-9 to ICD-10 occurred partway through 2015, discharges in the first quarter of 2015 and before were assessed with ICD-9 codes, and those afterward with ICD-10 codes. The volume of patients captured in the first quarter and second quarter of 2015 were statistically compared to ensure appropriate continuity for trend analysis, in accordance with HCUP guidelines. Years before 2012 were assessed using updated Trend Weights.
Outcomes
The primary outcomes of interest were the volume of hospital discharges associated with a pressure ulcer diagnosis, and the frequency of ulcer-related surgical procedures among this cohort. Ulcer-related procedures were defined by ICD-9 and ICD-10 procedure codes, and included debridement, graft or flap coverage. Secondary outcomes included hospital charges, patient demographics, patient comorbidities, mortality, length of stay and ulcer characteristics (severity and location). Location coding was performed using ICD-9/10 codes, with four location categories identified: back/sacrum, lower extremity, multiple locations and other/unknown. The back/sacrum location included upper back, lower back, buttock and sacral codes. The lower extremity location included lower extremity and foot. The other/unknown category included all other locations including elbow and head. Severity 3 and 4 ulcers were identified with ICD-9/10 codes and considered “severe” for the purposes of this analysis. Patients admitted during the 2008 calendar year were excluded from analysis of severe ulcer trends, as the ICD-9 coding scheme for ulcer severity was not introduced until October 2008. 11 To assess comorbidities, 31 chronic medical conditions were identified using the enhanced-Elixhauser algorithm.
Statistical Analysis
After isolating discharges with a diagnosis of pressure ulcer for each year, data sets were appended to facilitate analysis of trends over time. The number of hospital discharges, associated charges, patient characteristics, and hospital outcomes were determined for each year 2008-2019. Trends were then analyzed for patient sex, payer type, race, ulcer location, ulcer severity procedure occurrence, mortality, age, length of stay, and total inpatient charges.
For each categorical patient characteristic, a series of binary variables was generated to represent each strata (eg for each patient with potential insurance type of Medicare, Medicaid, Private, or Other, four binary variables were created, each representing “yes” or “no” for each payer). The prevalence of each patient characteristic over time was subsequently assessed using multiple logistic regression. Additional model covariates were included to control for confounding factors related to patient demographics (eg age, sex, race, etc.) and hospital characteristics (eg bed size, geographic location, teaching status, etc.). Continuous variables were assessed by multiple linear regression over time, with similar additional covariates used to control for patient demographics and hospital characteristics.
All analysis was performed StataMP 17 (StataCorp, College Station, TX). Significance was set at P < .05.
Results
Trends in Ulcer Volume and Mortality
From 2008-2019, 7,788,105 discharges with a diagnosis code of pressure ulcer were identified, representing an average of 1787 pressure ulcer diagnoses per 100,000 discharges per year. The proportion of all discharges with an ulcer diagnosis did not change during the time period (Figure 1), starting at 1.8% in 2008, and ending at 1.9% in 2019 (P = .479). Yearly patient volumes are presented by ulcer location in Table 1. 62.4% of all ulcers during the time period were located in the sacral or back area, followed by multiple locations and lower extremity location. The odds of a patient having a back/sacrum ulcer decreased during the time period (P < .001) as did the odds of a lower extremity location (P < .001) while the odds of multiple locations or other/unknown increased (P < .001). Annual patient and procedure volume for severe and non-severe pressure ulcers 2008-2019, on a logarithmic scale. Ulcer Volume and Mortality by Year and Location. arepresents β1 of simple linear regression, showing % change per year.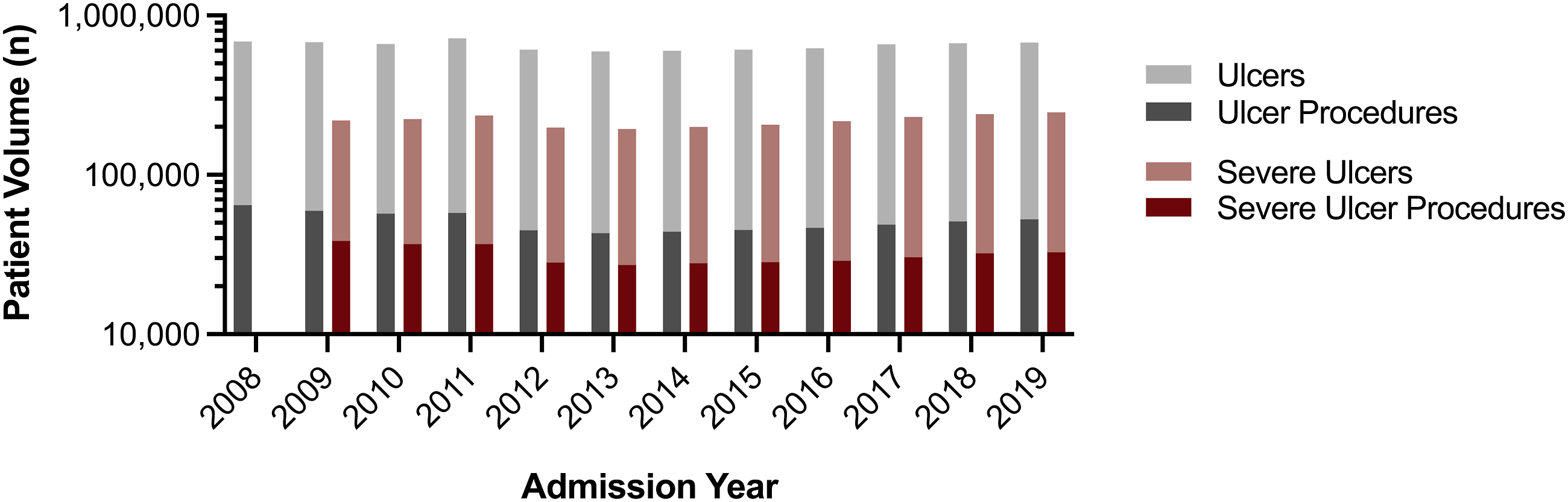
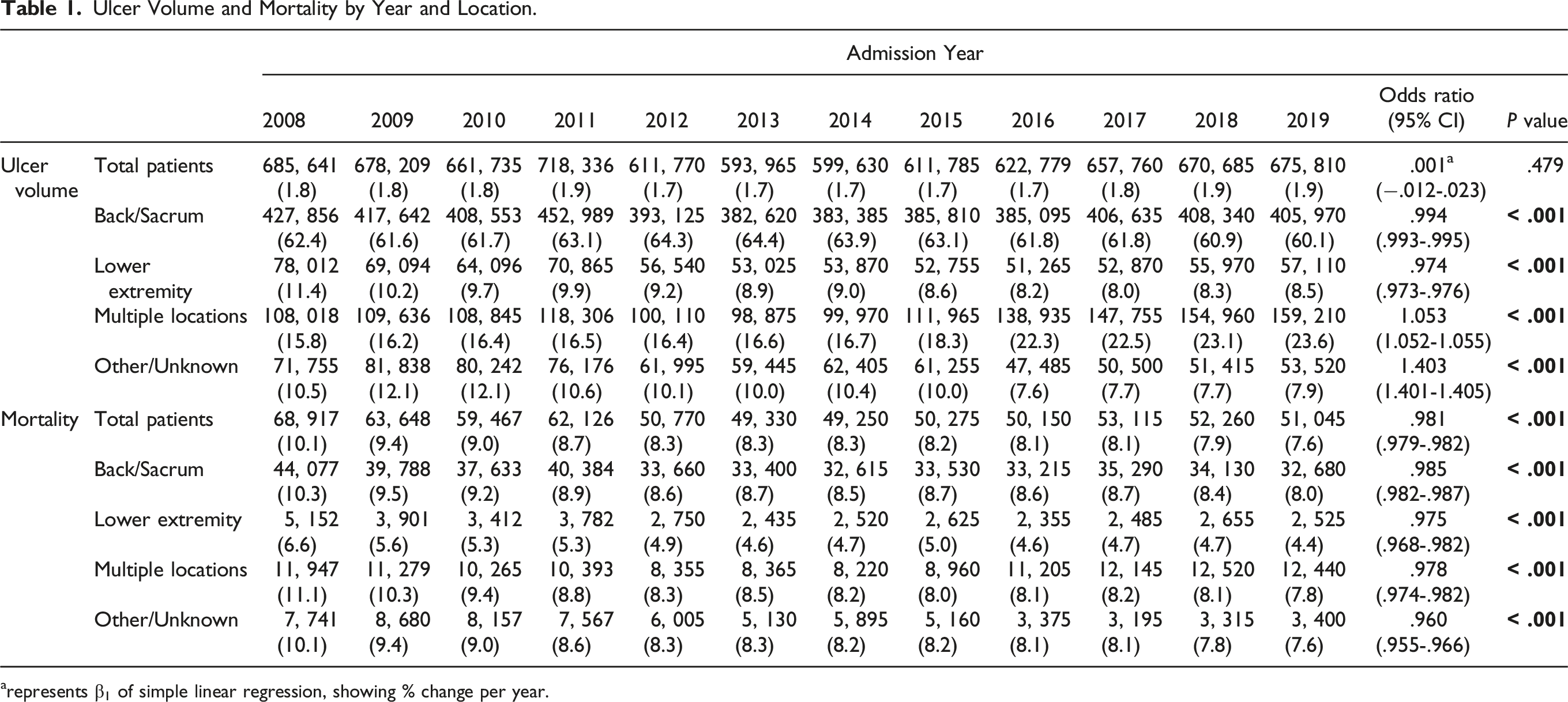
The mortality rate of patients with an ulcer diagnosis decreased from 10.1% in 2008 to 7.6% in 2019 (P < .001). This decrease in mortality rate was observed for each ulcer location (Table 1).
Trends in Patient Demographics
Ulcer Patient Demographics by Year.
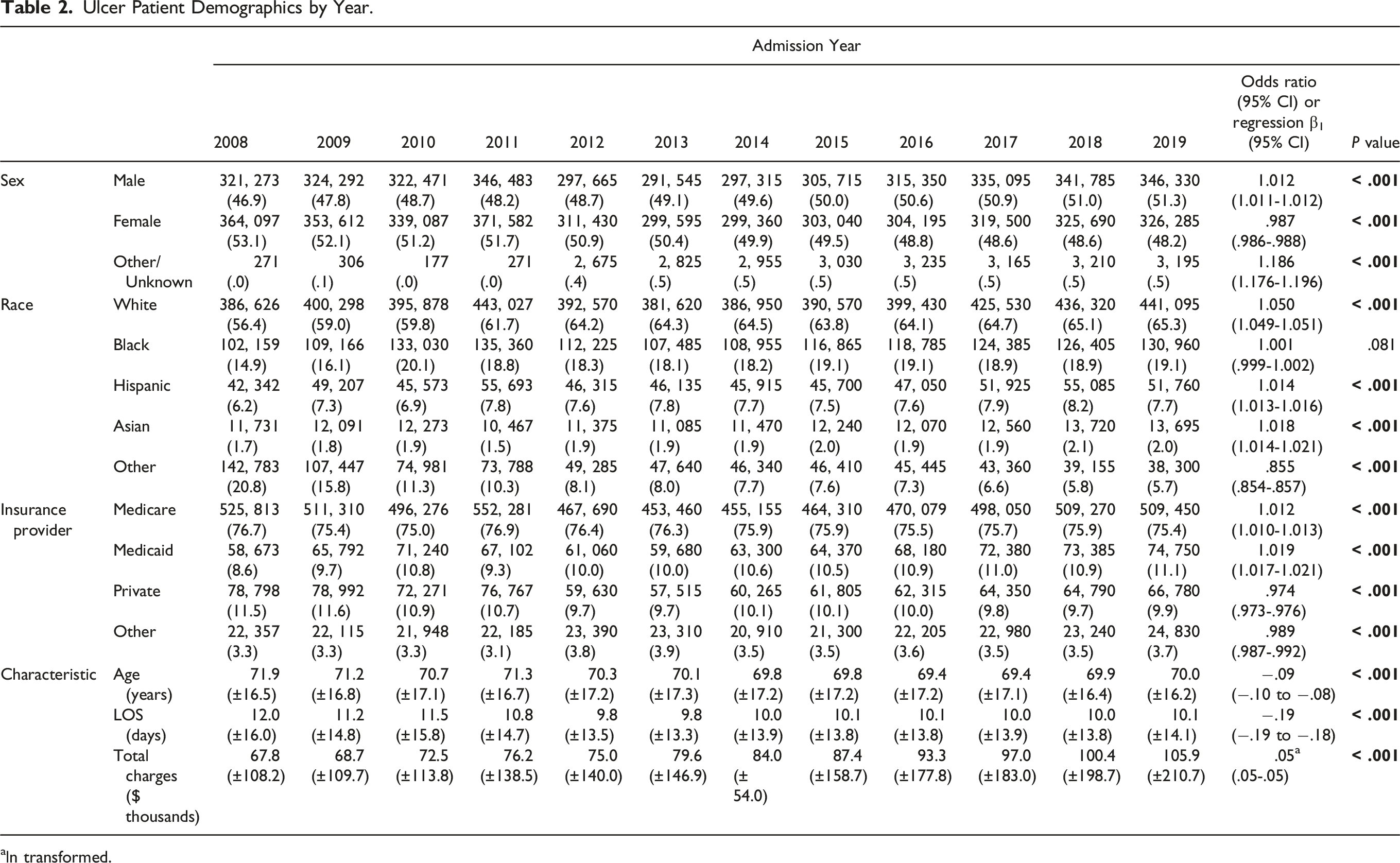
aln transformed.
The average length of stay of patients with an ulcer diagnosis decreased during the time period (P < .001) from 12.0 days in 2008 to 10.1 days in 2019. And the average total charges, logarithmically transformed, increased from $67,800 in 2008 to $105,900 in 2019 (P < .001).
Trends in Procedure Volume
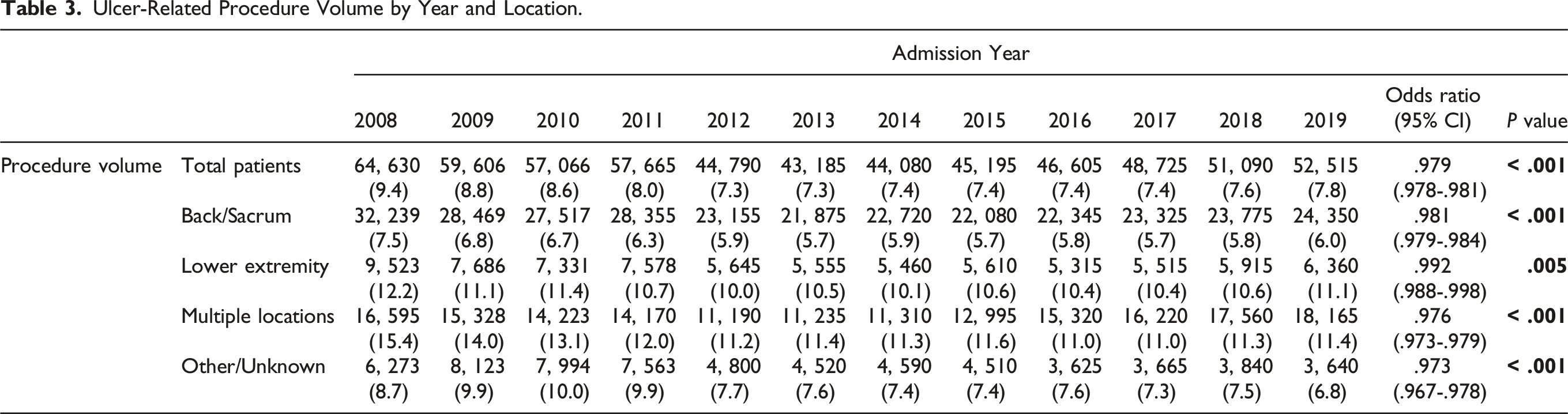
Ulcer-Related Procedure Volume by Year and Location.
Severe Ulcer Subgroup Analysis
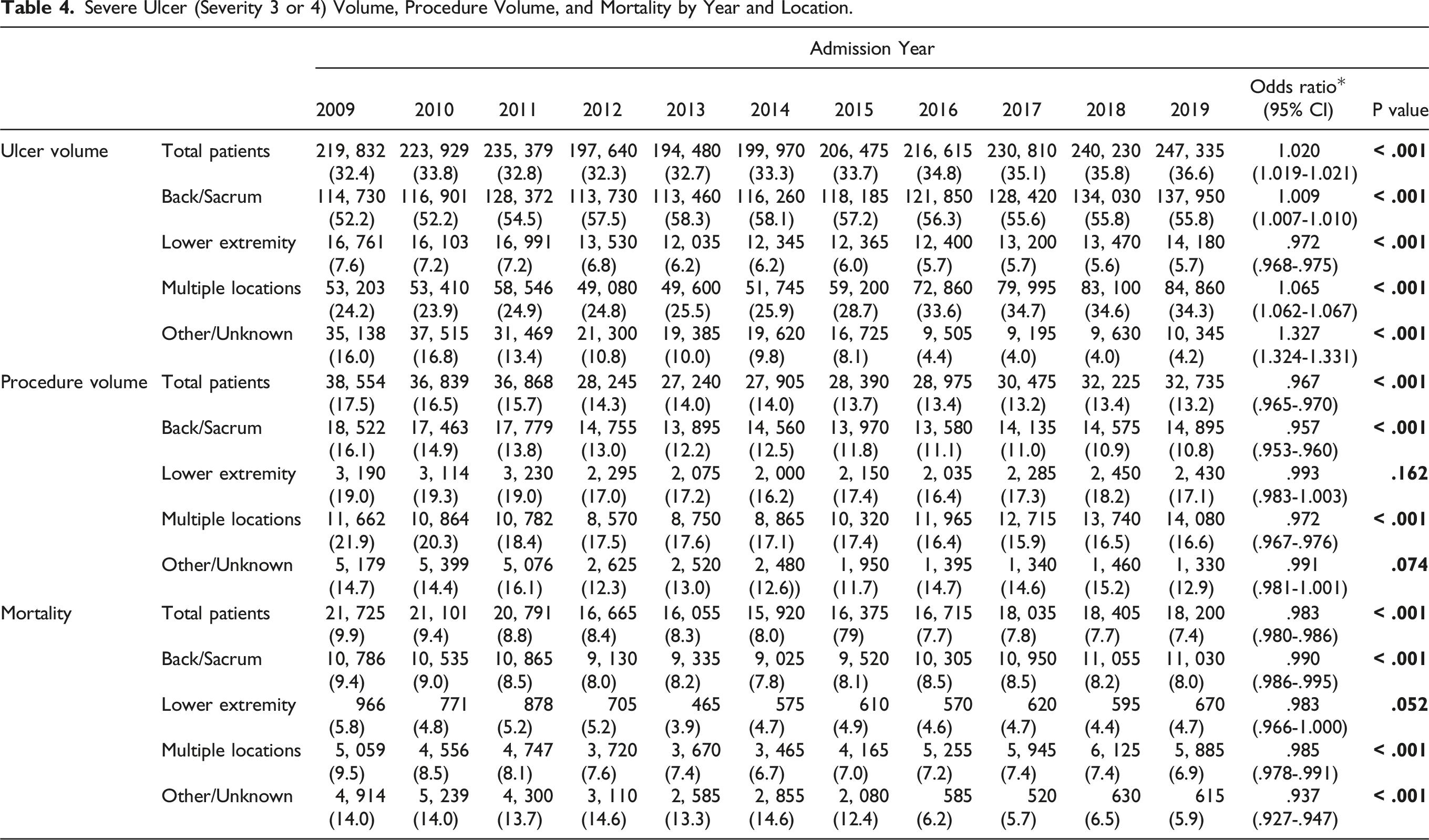
Severe Ulcer (Severity 3 or 4) Volume, Procedure Volume, and Mortality by Year and Location.
Discussion
Large-volume data from the NIS facilitates broad, longitudinal evaluation of changes in healthcare diagnosis, procedure and population dynamics. This type of analysis improves understanding of factors and changes in pervasive diseases, such as pressure ulcer. In this study, analysis of nearly eight million pressure ulcer patients over a twelve-year time period shows that the volume of pressure ulcer diagnoses remained stable from 2008 to 2019. Moreover, in this time period, the volume of ulcer-related procedures decreased despite an increase in the proportion of severe ulcers.
Although reimbursement changes instituted by CMS in 2008 and 2015 have made pressure ulcers a common focus of the medical community, 12 the impact of these policies on ulcer prevalence remains unclear. One investigation found no decrease in hospital-acquired pressure ulcers after the 2008 payment change. 13 Other work has supported this conclusion, and suggested that pressure injury rates have plateaued from 2015-2019. 14 In contrast, a study of acute care facilities revealed a decrease in overall and hospital-acquired pressure injury prevalence from 2006-2019. 15 Another investigation directly contradicted these findings, and suggested that hospital-acquired pressure injury rates rose 29.4% between the years of 2013-2016. Notably, this was the only hospital-acquired condition in the CMS Patient Safety Indicators 90 (PSI 90) that increased in this time, up to a rate of 4.8 cases per 10,000 hospital visits. 12 Our results show rates three times higher than this, likely explained by the fact that the ulcers in our analysis were not exclusively hospital-acquired.
Our results support findings of a plateau. Despite payment incentives ulcers remain prevalent. Reasons for a plateau may be related to the challenging nature of PI prevention. Some other hospital-acquired conditions may be “low hanging fruit” with simple prevention and higher weighting for payment incentives. More severe conditions are given a higher weight, so while pressure injury has a .06 weight, respiratory failure is given .30,12 incentivizing prevention of respiratory failure over pressure injury. Pressure injury may be more difficult to prevent, leading hospitals to focus efforts on other conditions.
Management of pressure ulcers can be complex and multimodal. For severity 3 or 4 ulcers surgical management is indicated, particularly if wounds show little healing with conservative management. Advanced surgical management often includes an advancement or rotational flap. 16 In our analysis, we show that the frequency of ulcer-related procedures went down among the total ulcer population, as well as among those with severe ulcers. Notably, there was also a decrease in procedures among patients with a stage 3 or 4 ulcer, the population most likely to require surgical intervention. 17 Due to the admissions-based nature of the NIS data, no outpatient or ambulatory management is captured, so a possible explanation for this trend could be a transition toward more ambulatory ulcer-related procedures. However, another trend that could explain this change is a movement toward negative pressure wound therapy (NPWT) for the treatment of PIs. NPWT has been added to the reconstructive ladder since its development in the 1990s. 18 And breakthroughs in technology including NPWT with instillation and dwell (NPWTi-d) have proven promising for management of pressure wounds. 19
Changes in population dynamics were assessed for this ulcer cohort. Results showed that the population became younger, and more male. As age is a well-established risk factor for PI, the decrease in age of the population may represent improved risk prediction and prevention in older patients, as new risk assessment tools are introduced. The proportion of patients with Medicaid increased, while the proportion with private insurance decreased, indicating a possible shift in the socioeconomic status of the cohort. Of note, about 75% of ulcer patients were insured under Medicare, with a slight increase over time, despite the small decrease in age over the time period. Race/ethnicity coding improved substantially during the time period, with 20.8% coded as missing or other in 2008, down to 5.7% in 2019.
In 2002, severity 3, 4, and unstageable ulcers acquired after admission were defined as never events, or serious reportable events, by the Agency for Healthcare Research and Quality National Quality Forum. Results from our analysis show an increase in the prevalence of severity 3 and 4 ulcers from 2008 to 2019. In support of our findings, Kayser et al. found that the 2011-2016 reduction in hospital-acquired pressure injuries previously reported 14 was due to a reduction in more superficial PIs rather than deeper, more severe PIs (stage 3, 4 or unstageable). 20 This finding was also supported by Padula et al who found the prevalence of severe pressure ulcers remained steady from 2009 to 2012. 7 Despite this finding, results also showed a decrease in mortality and length of stay. The increase in proportion of severe ulcers in our study was mostly seen from 2015-2019. These results may indicate that preventive efforts are not effective at targeting the most severe ulcers. However another interpretation, similar to changes in procedure volume, may be a movement toward more outpatient and ambulatory management of less severe pressure ulcers, which would increase the captured proportion of severe ulcers in an inpatient setting. Nevertheless, the relatively high prevalence of severe ulcers presented in the results raises the question of whether hospital-acquired ulcers should be measures of hospital quality, or are an unavoidable byproduct of multi-system disease. This question has implications for hospital quality measures and accordingly, payments from payers. Now that we’ve shown the prevalence of severe ulcers is not decreasing, this question should be explored in further work assessing the time of acquisition of these severe ulcers and the patients’ preceding health status.
Certain limitations must be acknowledged in this study. Primarily, the NIS is a discharge-based, administrative database. While this type of database facilitated this large analysis, certain constraints exist. Each discharge was analyzed as a unique instance, with no continuity between discharges. Some of the discharges may have represented multiple admissions for a single patient. Additionally, no data could be obtained on whether pressure ulcers were obtained in the hospital stay or were present on admission. Additionally, the results show pressure ulcers are largely a disease of advanced age. As trends in the entire population of advanced-age patients were not assessed, trends in ulcer prevalence and rates of procedures may be driven by overall trends in this population. Finally, the change in ICD coding during the time period limited granularity of diagnosis-related analyses, although we were able to confirm that the new set of codes did not capture significantly more or less patients. Finally, this analysis measures prevalence of pressure ulcers rather than incidence, which precludes analysis of hospital-acquired ulcers.
In conclusion, it was found that the overall prevalence of pressure ulcers in hospital admissions did not change from 2008-2019 in a nationally-representative sample of US hospital discharges. However during this time period the severity of ulcers increased, which may indicate success in prevention of less severe ulcers, but challenges in preventing more severe ulcers. Further work in identifying risk factors and effective preventative strategies for severe pressure ulcers is warranted. Also during this time period the volume of ulcer-related procedures performed went down, which may indicate a shift toward outpatient and less-invasive management, such as negative pressure wound therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.