
Abstract
Background
Marijuana use among adolescents may have increased after its legalization in the United States. An association between violence and marijuana use in adults has been demonstrated in previous reports. We hypothesized that adolescent trauma patients presenting with a positive marijuana screen (pMS) are more likely to have been injured by gunfire or knives and will have more severe injuries overall, compared to patients with a negative marijuana screen (nMS).
Methods
The 2017 Trauma Quality Improvement Program database was queried for adolescent (13-17 years old) pMS patients and compared to adolescents who tested negative for all substance/alcohol. Patients with positive polysubstance/alcohol were excluded.
Results
From 8257 adolescent trauma patients, 2060 (24.9%) had a pMS with a higher rate of males in the pMS group (76.3% vs 64.3%, P < .001). The pMS group presented more frequently after gun (20.3% vs 7.9%, P < .001) or knife trauma (5.7% vs 3.0%, P < .001) and less frequently after falls (8.9% vs 15.6%, P < .001) and bicycle collisions (3.3% vs 4.8%, P = .002). The rate of serious thoracic injury (AIS ≥3) was higher for pMS patients (16.7% vs 12.0%, P < .001), and more pMS patients required emergent operation (14.9% vs 10.6%, P < .001).
Discussion
In our adolescent patient population, one quarter tested positive for marijuana. These patients are more likely to be injured by guns and/or knives suffering serious injuries, and often require immediate operative intervention. A marijuana cessation program for adolescents can help improve outcomes in this high-risk patient group.
Key Takeaways
• Gun and knife trauma are more prevalent in adolescent patients presenting with a positive marijuana screen. • Patients with a positive marijuana screen more often presented with serious thoracic injuries and required an emergent operation compared to patients with a negative marijuana screen.
Introduction
Recreational marijuana use is relatively common worldwide and nearly 20% of the population in the United States has used marijuana in the past year. 1 The primary psychoactive component in marijuana is tetrahydrocannabinol (THC). 2 Its effects range from euphoria to anxiety and psychosis, 2 and its popularity has skyrocketed since the widespread legalization of medicinal and recreational marijuana use in the United States. 3 The effect of THC on users is through its interaction with endocannabinoid receptors throughout the body. 2 These receptors play a crucial role in regulating emotional behaviors. 4 Although this is a complex interaction affecting a wide range of behaviors and resulting in acute impairments of learning and memory, 5 users can experience lapses in judgment predisposing them to high-risk behaviors including aggression and violence. 6 Adolescent and pediatric patients are particularly vulnerable to the effects of THC, given their significantly increased expression of CB1 receptors. 2
Within many US States, recreational use of marijuana is legal for adults aged 21 years and older, however, the new widespread commercial availability raises concerns about marijuana use in adolescent populations. 2 In support of this concern, the rate of trauma patients screening positive for marijuana (pMS) after legalization has increased compared to pre-legalization amongst all age groups. 7 The prevalence of pMS in adolescent trauma patients presenting to a Level-I trauma center in California increased by nearly 20% after recreational legalization. 8
Health-care providers, including social workers and case managers, play critical roles in mitigating high-risk behaviors amongst trauma patients, helping them make lifestyle changes that may help prevent placing them in precarious situations in the future. A previous single-center study demonstrated a strong association between marijuana use in adolescent trauma patients and increased rates of injury and trauma center admissions. 9 These admissions may be related to violence as either a victim or aggressor. The purpose of this study was to evaluate the severity of injuries suffered by adolescent patients who have used marijuana. We hypothesized that patients presenting with a positive marijuana screen (pMS) would be more often involved in mechanisms involving gunfire or knife trauma and have more severe injuries, compared to patients with a negative marijuana screen (nMS).
Methods
This retrospective study was deemed exempt by our local Institutional Review Board. The 2017 TQIP database was queried for all adolescent trauma patients (13-17 years old) who were screened for illicit substances and alcohol upon hospital admission. We excluded patients who were dead on arrival and patients who did not undergo substance testing. Also, to avoid potential confounders, all patients with positive alcohol screens (EtOH >0) or substance screens—aside from marijuana—(eg opioids, cocaine, methamphetamines, benzodiazepines, barbiturates) were excluded. We excluded patients that were not tested for alcohol, and we excluded patients that were not tested for illicit drugs.
Patients who screened positive for marijuana only (pMS group) were compared to patients who tested negative for all substances and alcohol (nMS group). The primary outcome of this study was the mechanism of trauma. We included both blunt and penetrating (ie gunfire or stab) mechanisms of injury. The secondary outcomes were the severity of injury, as defined by the abbreviated injury scale (AIS) for the head, thorax, abdomen, and spine. Demographics collected for this study included age, sex, injury severity score (ISS), and vitals upon hospital presentation. Other measured outcomes included total hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, respiratory complications (defined as acute respiratory distress syndrome (ARDS), pneumonia, and/or unplanned intubation), as well as the rate of mortality. We also examined the rate of undergoing any operation during hospitalization including the cerebrovascular, gastrointestinal, respiratory, hepatopancreaticobiliary, genitourinary, and orthopedic systems.
For bivariate analysis, the Mann-Whitney U test and Pearson’s chi-squared analysis were used for continuous and categorical variables, respectively; continuous variables were reported as medians with an interquartile range and categorical variables were reported as frequencies. All P-values were two-sided, with a statistical significance set at P < .05. All analyses were performed with IBM SPSS Statistics for Windows (Version 28, IBM Corp., Armonk, NY).
Results
From 14 496 adolescent trauma patients, 8257 patients met the inclusion criteria. Of these, 6197 (75.1%) patients tested negative for all substances and alcohol (nMS), and 2060 (24.9%) patients tested positive for marijuana only (pMS). The median age for both pMS and nMS patients was similar (16 years), with a higher rate of males in the pMS group (76.3% vs 64.3%, P < .001).
Compared to nMS patients, pMS patients had a higher median ISS (9 vs 8, P < .001) and a higher rate of severe (AIS grade>3) injuries to the thorax (16.7% vs 12.0%, P < .001) but similar rates of severe injuries to the abdomen, spine, and head (all P > .05). The most common overall injury in both groups was to the lungs (pMS 22.8%, nMS 18.7%, P < .001).
Demographics of Adolescent Trauma Patients With and Without Positive Marijuana Screen on Admission.
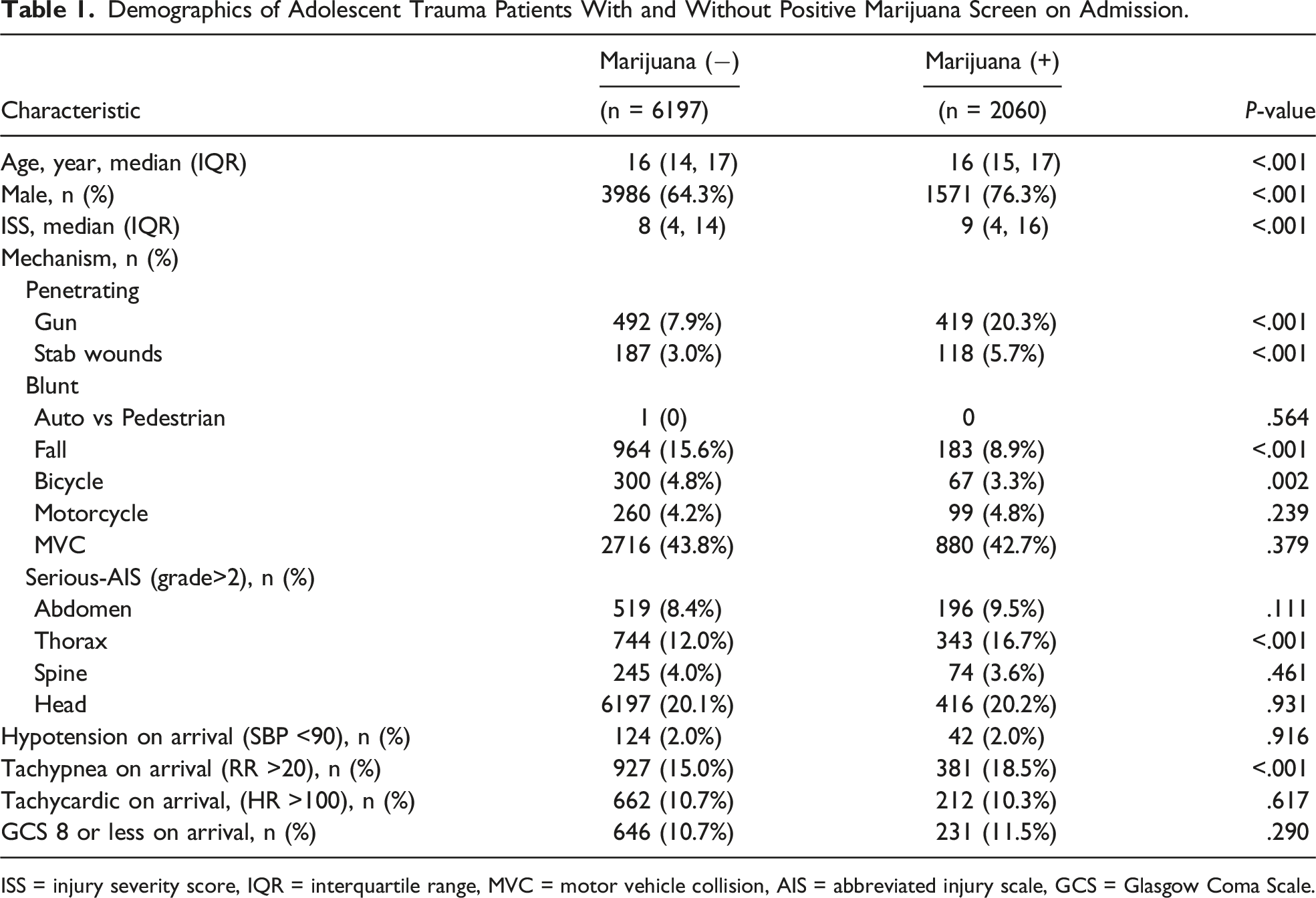
ISS = injury severity score, IQR = interquartile range, MVC = motor vehicle collision, AIS = abbreviated injury scale, GCS = Glasgow Coma Scale.
Clinical Outcomes in Adolescent Trauma Patients With and Without Positive Marijuana Screen on Admission.
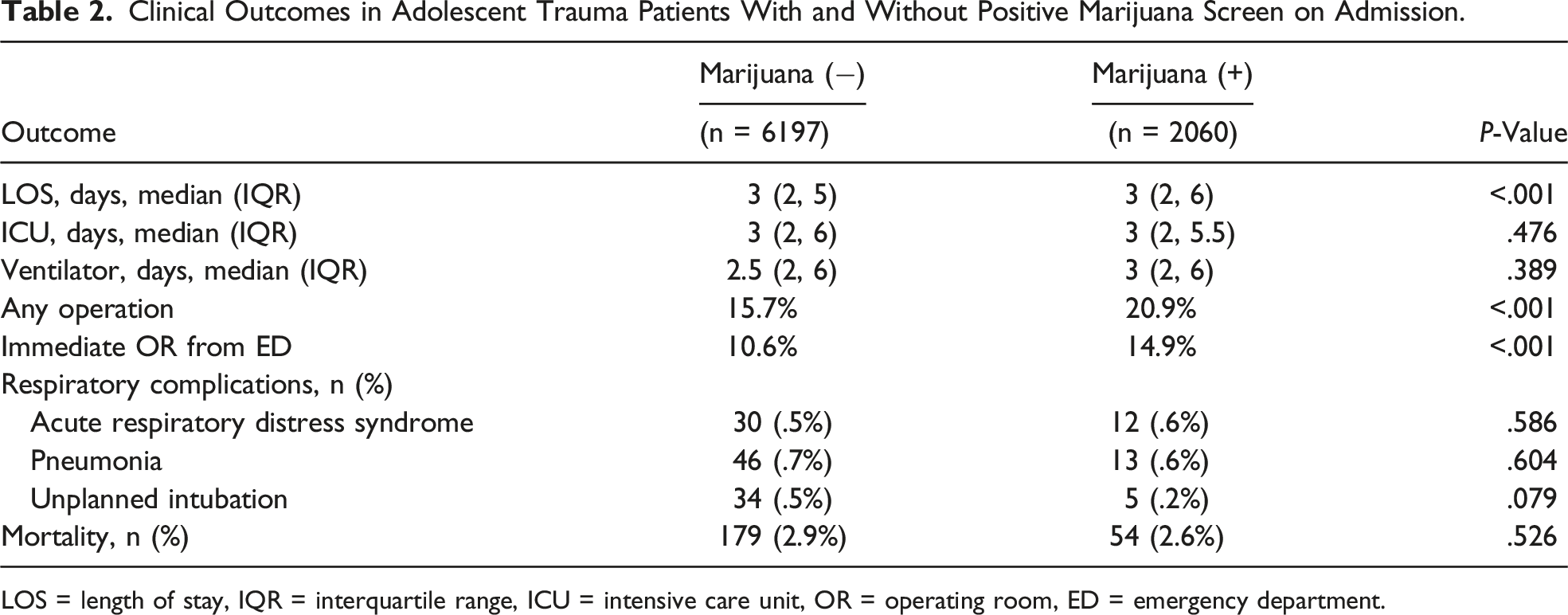
LOS = length of stay, IQR = interquartile range, ICU = intensive care unit, OR = operating room, ED = emergency department.
Discussion
This study sought to evaluate the incidence of penetrating trauma in adolescents with a positive marijuana screen compared to those with negative alcohol and substance screen. Previous studies have demonstrated a relationship between marijuana use and aggression leading to violent behaviors. 4 This national analysis demonstrated that both gunfire and knife injuries were more common among pMS adolescents while blunt trauma mechanisms such as falling and bicycle accidents were more prevalent among nMS patients. Also, pMS patients more often presented with serious thoracic injuries and required an emergent operation compared to nMS patients. While we are currently limited in our ability to determine if the individual patient is the aggressor or victim, there is a clear correlation between pMS and gun or knife trauma.
Marijuana may pre-dispose users to aggressive behaviors, which may consequently result in gun or knife violence. 4 Marijuana can trigger aggression due to effects on the endocannabinoid system (ECS). The ECS plays a critical role in regulating the maturation of neuronal networks that support cognitive and behavioral functions during adolescence. 6 The adolescent brain is more vulnerable and may have more pronounced responses to THC effects due to increased expression of cannabinoid receptors. 2 This association may disproportionally affect adolescents, as multilevel growth curve models have demonstrated physical and social aggression following a curvilinear trajectory throughout adolescence. 10 Furthermore, adolescents disproportionally suffer the consequences of violence which include traumatic injury. 11 Substance use, including marijuana, can lead to acute and long-term pharmacological effects on functional behavior. 12 Hypervigilance, cognitive dissonance, irrationality, and disinhibition of aggressive impulses have all been described as potential socio-behavioral consequences of adolescent substance use.2,4 This trend has been consistently shown in national surveys, which have reported two-fold higher rates of violent behaviors in adolescents who used any illicit substance within the previous year. 13 Moreover, multiple studies have demonstrated that adult pMS patients are more likely to be associated with penetrating traumas (stabbing, gunshot wounds).3,7 Our study confirms these associations in adolescent patients as we found a positive association between pMS and gun or knife trauma. Healthcare providers may be in a unique position to counsel adolescents presenting with pMS to abstain from marijuana use, which may potentially mitigate trauma recidivism.
Although marijuana use can potentially lead to aggression on behalf of the user, it may also place users in vulnerable situations where they may be the victim of a violent attack. Marijuana can decrease one’s ability to accurately identify, evaluate, or avoid dangerous persons or situations. 6 Adolescents engaged in marijuana use have been demonstrated to be associated with increased victimization by intimate partner violence. 14 In addition, being a victim of a violent crime can increase the odds of using marijuana in the future possibly leading to a viscous cycle. 15 Although our study cannot determine if the trauma patient was the perpetrator or the victim of gun or knife trauma, there appears to be a clear correlation between the two. Much of the existing literature focuses on marijuana and victimization in the context of domestic violence and not penetrating trauma. Future studies are needed to confirm if marijuana use is specifically associated with being a victim of gun or knife trauma.
Marijuana has been associated with decreased reaction time and poor balance. 16 This disturbance in equilibrium has been associated with an increased risk of motor vehicle collisions. 17 In adolescent patients, most of whom are too young to drive, the same disturbance in equilibrium may result in a higher incidence of falls and bicycle collisions. A previous study examining the impairment of marijuana on bicycle riding could not define a THC concentration that led to an inability to ride a bicycle safely. 18 Our study found the opposite to be true in that pMS patients had a lower incidence of falls and bicycle collisions. This may be related to the temporal relation as there is a time-dependent reaction response with marijuana with the most severe impairment occurring shortly after consumption. 19 The temporal relationship of marijuana use and injury is unavailable in TQIP. Future research is needed to confirm these findings.
A link between marijuana use in trauma patients and adverse outcomes may partially be explained by the severity of injuries. 20 Lank et al. 20 have previously reported that pMS trauma patients are admitted with more serious injuries. Bloom et al. 3 also reported the prevalence of pMS patients admitted with severe thoracic injuries is significantly higher than nMS patients (3.8% vs 2.6%, P < .001). Our study confirms these previous reports with respect to thoracic injuries, in the adolescent population. However, we did not find an association between marijuana use and severe abdominal, spine, or head injuries. This may simply be a reflection of the overall higher rates of penetrating thoracic trauma in pMS patients vs abdominal trauma. The specific location of the gunshot or stab wound is not available in the dataset.
Limitations of this study are those inherent to a retrospective database design which includes missing data, coding errors, and reporting bias. Many relevant variables such as self-reported detailed substance use history, cause of patient mortality, and post-discharge data were not available in this database. The sensitivity of currently available marijuana screening tests was another important limitation of this study. It should be noted there is a wide range of methodologies and protocols used by individual participating institutions regarding screening for illicit substances and/or alcohol, and no standardized practice exists in TQIP. Patients with low levels of marijuana consumption may not be detected due to the standard detection limit of 50 ng/mL for THC. Since marijuana screening in this database was an all-or-nothing variable, the frequency, quantity, method (ie ingestion vs inhalation), and temporal relationship between marijuana use and injury were also not available for analysis. In fact, the half-life of THC varies from 20 to 36 hours in occasional users to 4-5 days in heavy users, requiring 30 days for complete elimination from the body; therefore, it is unclear if the use of marijuana occurred around the time of trauma or before it. This limitation is important to consider as the intoxicating effects of marijuana may have been gone by the time in which the trauma occurred; however, the patient may have continued to screen positive for marijuana upon admission. The retrospective nature of the analysis also limits our ability to determine whether a direct causation—rather than a correlation—between marijuana and gun or knife trauma exists. Lastly, a lack of data regarding the circumstances preceding injury limits our ability to distinguish whether a patient was a victim or a perpetrator of violence. Despite these limitations, the generalizability of these results is strengthened by the large number of patients and trauma centers included.
Conclusion
Our study found that gun and knife trauma are more prevalent in adolescent patients presenting with a pMS. More pMS adolescents sustained serious thoracic injuries which often required immediate operative intervention. While this study could not evaluate whether marijuana directly led to aggression or victimization, resulting in injury, it clearly demonstrates a correlation between marijuana use in adolescents and involvement in high-risk situations with guns and/or knives. These results are particularly concerning as the rate of marijuana use in adolescent trauma patients is high and is expected to continue to rise with legalization in the US. Hence, primary and secondary prevention efforts may be warranted to help curtail the worsening epidemic of marijuana use in adolescents as it appears related to knife/firearm violence. Although marijuana may result in disturbances in equilibrium, we found marijuana to be associated with a lower incidence of falls and bicycle collisions in adolescent trauma patients. These findings need to be validated with future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.