
Abstract
The ideal management of perforated colorectal cancer in the hernia sac remains a challenge for general surgeons. We report such a case requiring a combined-incision surgical approach and two-stage operation. A male patient in his 80s presented with fatigue and a bulge in his left groin. Contrast-enhanced CT scan revealed a sigmoid colon perforation within the left inguinal hernia sac. A combination of midline abdominal and inguinal incisions was performed for the iliopubic tract repair and Hartmann procedure. Six months later, the recurrent inguinal hernia was repaired using the Kugel mesh. The treatment strategy for colonic perforation into the inguinal hernia remains nonstandardized, compared to those for nonperforated cases. Combined inguinal and midline abdominal incisions might be necessary for infected lesion removal and colon mesentery resection; using mesh to repair hernia is a rare option. Hernia repair using mesh can be performed in two stages when recurrence occurs.
Introduction
The development of management guidelines has led to standardizing surgical procedures for inguinal hernias. 1 Despite advances in hernia surgery, perforated colorectal cancer into the hernia sac remains one of the most challenging conditions and a common dilemma for general surgeons. There is still no consensus on the best surgical approach for these exceptional cases; thus, the strategy should be tailored to suit each case, and the surgeon must thoroughly understand the characteristics of each surgical approach, including open laparotomy, inguinal incision, and laparoscopy. Herein, we present a case of colorectal cancer that perforated the inguinal hernia sac and required a combined incision surgical approach. We discuss the ideal surgical management for these difficult situations, including the specific order and timing of each surgical approach, as well as the use of mesh.
Case History
A male patient in his 80s with past medical history of Alzheimer’s disease presented to our hospital with a 2-week history of fatigue and a bulge in his left groin. On arrival at the hospital, his vital signs were stable. Physical examination revealed a huge bulge of 10 cm in size around his left scrotum, while the abdomen was soft and flat, without any tenderness. Although the inguinal hernia contents could not be reduced into the peritoneal cavity, there was no evidence of strangulation. Laboratory findings on admission were WBC, 13200/μL; Hb, 11.0 g/dL; CRP, 22 mg/dL; CEA, 1.9 ng/mL; and CA19-9, 14.5 U/mL. Contrast-enhanced computed tomography (CT) scan revealed that the sigmoid colon had herniated into the left inguinal hernia sac. Abscess formation in the hernia sac and adjacent abdominal wall, as well as inflammation of the bowel wall and air within the sac were detected; thus, perforation of the herniated segment of the colon due to diverticular disease or colon cancer was suspected (Figure 1(A)). Since the contamination was confined to the scrotum and the adjacent abdominal wall, we decided to remove the colon, including the perforation site, and drain the abscess from the inguinal approach first. Surgery was initiated using an anterior approach through the left inguinal incision (Figure 1(B)). The sigmoid colon mesentery was dissected; however, the area around the hernia ring adhered to the surrounding tissue firmly and could not be circumferentially dissected. Therefore, we proceeded with an additional midline abdominal incision (Figure 1(B)). After dissection around the hernia ring, the area of the hernia sac that had been invaded by the tumor was resected. The remaining hernia sac was simply sutured closed, and inguinal hernia repair was performed via the iliopubic tract method as an open non-mesh posterior repair. Hartmann’s procedure was then performed, and gross pathology after colon resection revealed a sigmoid colon cancer with a maximum diameter of 4.5 cm (Figure 1(C)). The histopathological stage was a well-to-moderately differentiated adenocarcinoma, pT4aN0M0 Stage IIB (0/14 lymph nodes harvested). Adjuvant chemotherapy was considered, as this patient had high-risk stage II pT4a colon cancer with a perforated colon. However, this was determined to be inappropriate, as the patient was an 80-year-old man with an Eastern Cooperative Oncology Group Performance Status scale of 3 and a history of Alzheimer’s disease. The patient was subsequently transferred to a rehabilitation hospital without postoperative complications. His left inguinal hernia recurred 6 months after the initial surgery; therefore, the Direct Kugel method via an inguinal approach as a second-stage surgery was performed using Direct Kugel® Patch (two-layer heavyweight polypropylene mesh) (Figure 1(D)). Approximately two years after the initial operation, the patient was healthy, with no evidence of hernia or colorectal cancer recurrence. (A) Contrast-enhanced CT performed on initial admission. Sigmoid colon had herniated into the left inguinal hernia sac with abscess formation (arrowhead). (B) Schematic representation of iliopubic tract repair and Hartmann procedure in our case. Sigmoid colon had herniated into the left inguinal hernia sac with abscess formation in the scrotum (arrowhead). The abscess extended to the abdominal wall (arrow). (C) Resected specimen: Sigmoid colon cancer with perforation. (D) The recurrent inguinal hernia was repaired using Kugel mesh.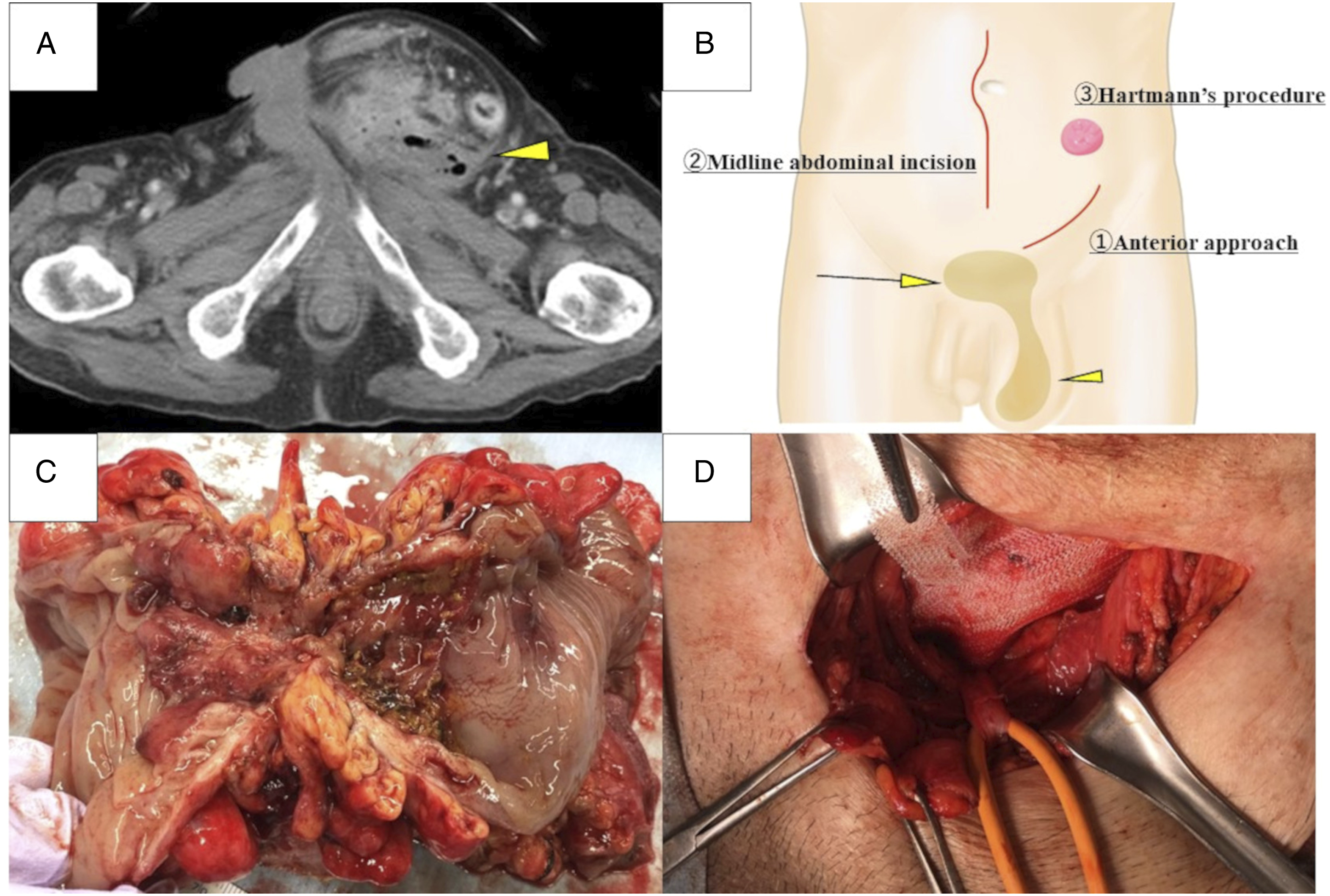
Discussion
Surgical Approach and Mesh Usage in Perforated Cases vs Non-Perforated Cases.
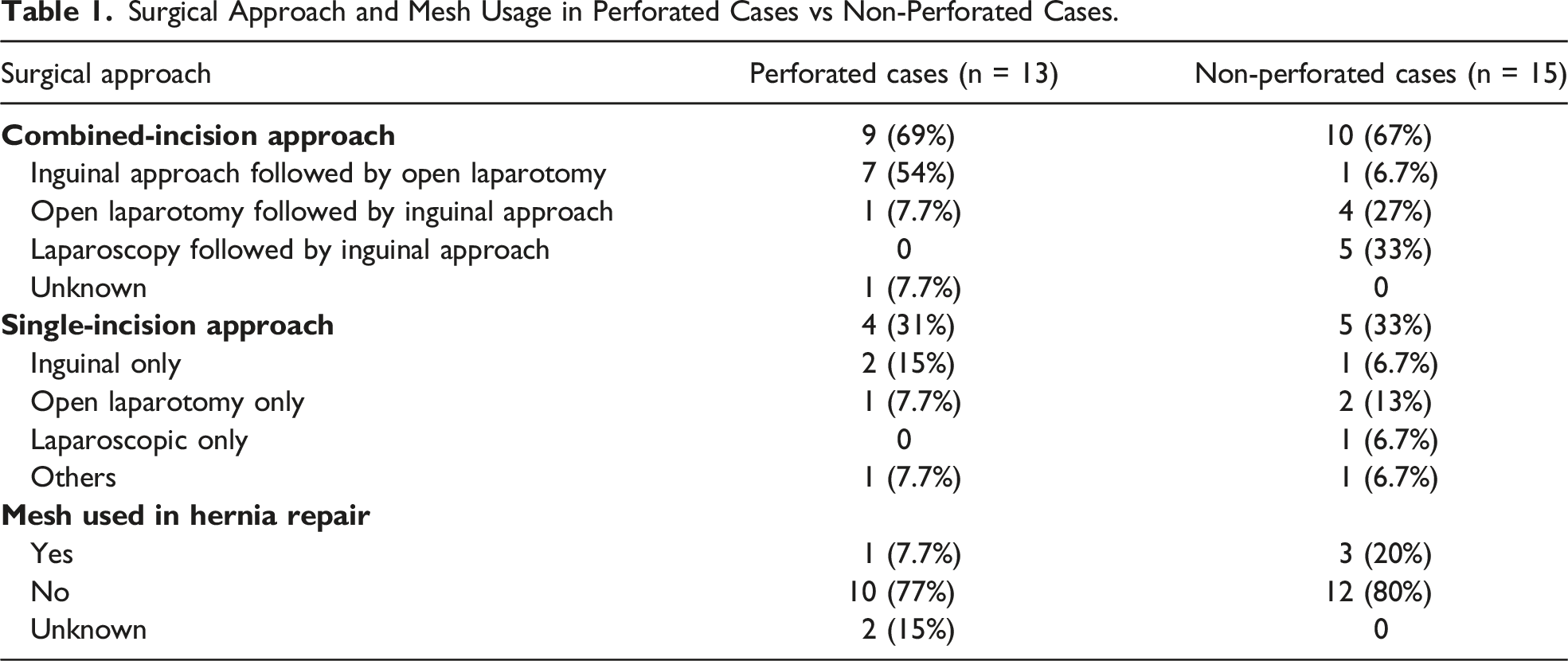
The current general opinion is that using mesh in clean-contaminated surgical fields could be considered on a case-by-case basis; however, the use of mesh in contaminated or dirty surgical fields is still not recommended. 2 Among the case series in Table 1, none of the perforated cases used mesh during hernia repair, except one case with almost no contamination from perforation. 4 Most cases underwent mesh-free hernia repair due to the risk of mesh contamination; the recurrence rate of inguinal hernia cannot be determined because it has rarely been reported in literature. The high recurrence rate of biologic mesh makes it unsuitable for inguinal hernias. Therefore, the utilization of mesh to repair an inguinal hernia is unlikely to be applied as a general principle in a situation with colorectal perforation into a hernia sac, such as in the present case. We believe the initial operation should prioritize the resection of colorectal cancer based on the principles of oncology and infection control and that a two-stage hernia repair with mesh is most effective if the hernia recurs.
Conclusion
Hernia contents may consist of colonic cancer in cases of long-term nonreducible inguinal hernias in the elderly. In cases of perforated colon cancer in the inguinal hernia sac, oncological resection of colorectal cancer and effective infection control should be prioritized during the initial operation. Combined, two-incisional approach starting with an inguinal incision and adding a midline abdominal incision enables the secure removal of the infected lesion and resection of the malignant tissue. Considering the contaminated nature of these conditions, mesh is unlikely to be used; hernia repair using mesh should be performed as a two-stage surgery when necessary.
Supplemental Material
Supplemental Material - Management of Perforated Sigmoid Colon Cancer in an Incarcerated Inguinal Hernia Using a Combined Abdominal and Inguinal Approach
Supplemental Material for Management of Perforated Sigmoid Colon Cancer in an Incarcerated Inguinal Hernia Using a Combined Abdominal and Inguinal Approach by Kohei Chida, Morihiro Katsura, Takashi Kato, Kazuya Sunagawa, and Masafumi Ie in The American Surgeon
Footnotes
Acknowledgements
The authors wish to thank the surgical residents, attending surgeons, and all medical staff involved in this patient’s treatment. The authors wish to thank Mr. Yuji Hatanaka, MD, for his support of the schematic representation.
Author Contributions
KC was responsible for data curation, original draft preparation, patient care, and approval of the final manuscript. MK was responsible for data curation, reviewing and editing, patient care, supervision, and approval of the final manuscript. TK, MI, and KS was responsible for reviewing and editing, patient care, and approval of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Okinawa Chubu Hospital Alumni Association grant.
Patient Consent
Written informed consent was obtained from the patient and the patient’s son, next of kin, for publication of this manuscript and any accompanying images since the patient had mild cognitive impairment due to his age.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.