
Abstract
Background
Surgically assisted rapid palatal expansion (SARPE) is an established method to treat transverse maxillary hypoplasia in skeletally mature adult patients. SARPE affects the surrounding soft tissue. In addition, effects on the airway and breathing have been described. Aim of this study was to assess the effects of SARPE on the nasal soft tissue and the upper airway by means of three-dimensional stereophotogrammetry and cone beam computed tomography (CBCT).
Methods
This retrospective study used preoperative and postoperative cone beam computed tomography (CBCT) scans and three-dimensional stereophotogrammetry. Ten skeletally adult patients (4 male, 6 female; mean age 27.68 years) with transverse maxillary hypoplasia were included. Patients had undergone SARPE procedure, performed by the same surgical team using the same technique. Nasal soft tissue changes were analyzed, using three-dimensional stereophotogrammetry records taken preoperatively (t0) and at the postoperative checkup appointment (t1). The upper airway was assessed using CBCT scans for surgical planning (t0) and the first scan taken after SARPE (t1).
Results
In stereophotogrammetry, it was shown that only a few soft tissue nasal parameters increased significantly and SARPE leads to mainly clinically irrelevant changes in nasal soft tissue. In CBCT, only a significant increase in nasopharyngeal airway volume was found.
Discussion
Results were in alignment with literature. The effects of SARPE on the nasal soft tissue are mostly statistically insignificant and clinically irrelevant. Airway volume significantly increased in the nasopharyngeal area. Further research on SARPE effects should be conducted to reinforce SARPE as a treatment option for sleep apnea patients.
Key Takeaways
• Soft tissue changes after SARPE are mostly insignificant • Airway volume changes can be demonstrated in CBCT scans • SARPE can be considered a treatment option for OSAS
Introduction
Transverse maxillary deficiency can have a dental origin, a skeletal origin, or a combination of the 2.1,2 Orthodontic maxillary expansion by opening the midpalatal suture was first described in 1860 and has become an established method in cases of transverse maxillary deficiency. 3 The method creates new bone by distracting the median palatine suture, where new bone is formed, and therefore broadens the maxilla and dental arch. The technique is traditionally used to treat crossbite, but has gained importance in the treatment of obstructive sleep apnea syndrome (OSAS) in the recent years.4-6 In adult patients, due to the denser bone structure and higher resistance of the midface pillars, orthodontic broadening can show flexion of the maxilla and dental tipping and lead to insufficient results as well as side effects.7,8 For satisfactory results, surgically assisted rapid palatal expansion (SARPE) is used in those patients: the closed suture as well as the midface pillars are surgically released. 8 Additionally to the alteration of the bony midface, SARPE leads to changes of the surrounding area: broadening of the nasal soft tissue and nasal cavity and an enlargement of the pharynx are described.5,6,9
In a study of cone beam computed tomography (CBCT) before and after SARPE, a significant increase in bony and soft-tissue nasal measurements, as well as a correlation between bony and soft tissue changes were shown. 10 Analyses of soft tissue in stereophotogrammetry described significant changes in the nasal area, transverse widening of the inter-alar width, and a slight increase in inter-alar curvature point width after SARPE. 11 Sagittal, transverse plane, and cross-sectional enlargements in lower pharyngeal areas after SARPE were observed in computed tomography after SARPE. 6 Further research suggests that SARPE improves nasal breathing. 12 In sleep apnea patients, SARPE seems to improve several parameters in polysomnography, and has become part of the surgical treatment algorithms for OSAS.5,13
Although changes after SARPE have been described with various methods, to our knowledge, there has not yet been research focusing on detailed measurements of the airway in CBCT as well as the soft tissue on photogrammetric records. The aim of this study was to describe soft tissue and airway changes after SARPE in outpatient care, using virtual three-dimensional analyses of CBCT scans and photogrammetric records from daily practice. Furthermore, this research should improve the understanding of SARPE and its effects on the airway. A more extensive understanding of these effects could support the decision making process in surgical OSAS treatment, where a wide range of procedures with various effects on the airway are available. 13 Improved knowledge and understanding also can contribute to better patient education especially when it comes to esthetic after effects.
Methods
The study was approved by the ethics committee of the Technical University of Munich (reference: 2022-251-S-NP, Munich, Germany).
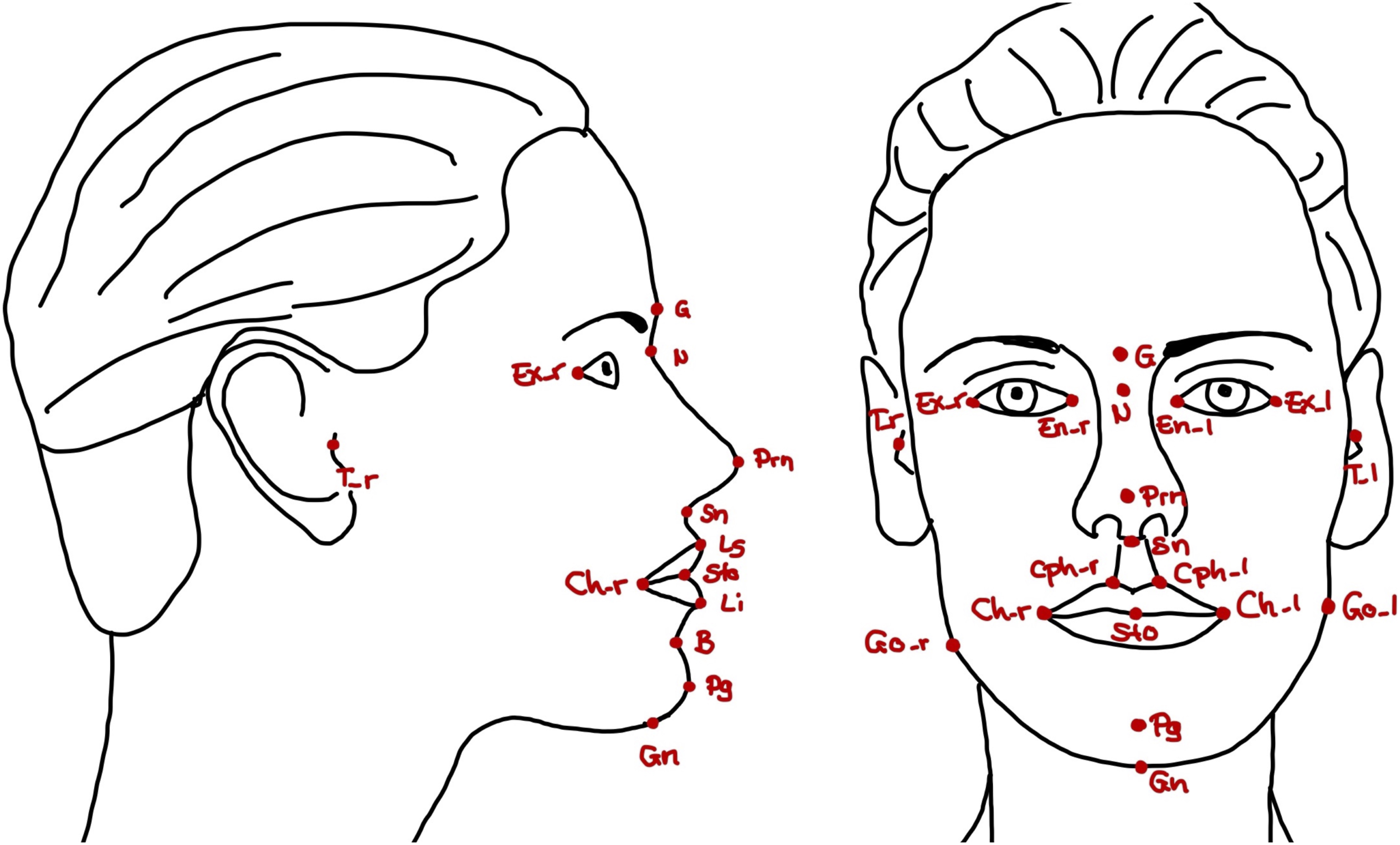
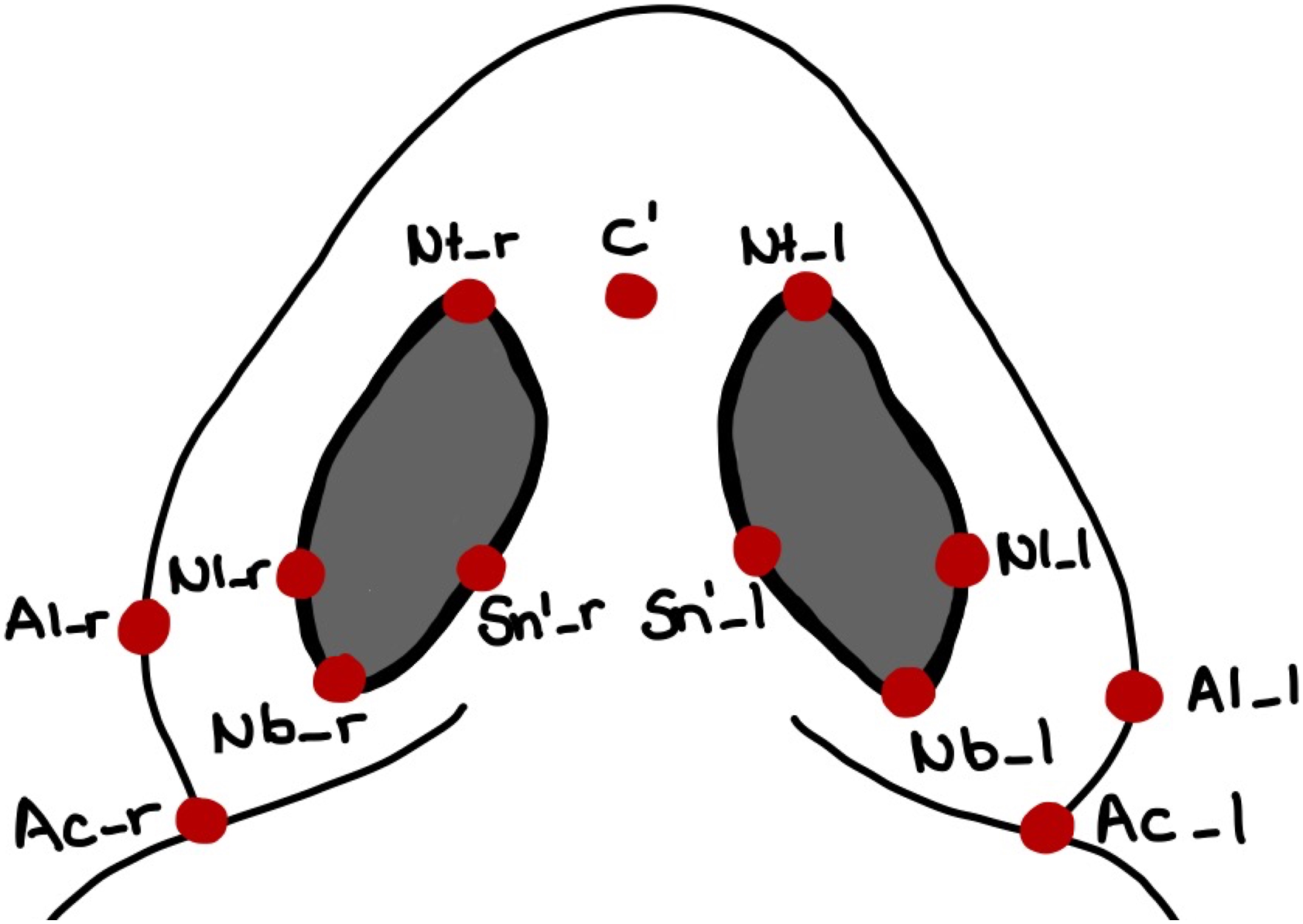
This retrospective study consisted of 10 skeletally mature adult patients (4 male, 6 female; mean age 27.68 years) diagnosed with transverse maxillary hypoplasia, who had undergone the SARPE procedure in our clinic between January 2019 and July 2021. All patients were otherwise healthy. No patient reported sleep apnea. The Body Mass Index (BMI) was not recorded. Informed consent was obtained prior to the surgery. We included all patients who had attended postoperative check-ups until July 2021. Patients with syndromes or incomplete postoperative records were excluded from the study. All surgical patients were operated on under general anesthesia by the same surgical team. Le Fort I plane and midpalatal suture were weakened using a piezo saw. For better lateral movement of the segments, SARPE included pterygomaxillary disjunction and resection of a small bony wedge from the lateral sinus wall. For surgical planning, CBCT scans (ProMax® 3D Mid, Planmeca Oy, Helsinki, Finland), and photogrammetric images (3dMDface-System, 3dMD LLC, Atlanta, GA, USA) were taken before SARPE (t0) and after surgery for postoperative check-ups (t1). Stereophotogrammetry is a method of 3D surface imaging which has become common in orthognathic surgery planning and research. It is a fast and easy to use facial surface imaging modality used for planning and patient education. Stereophotogrammetric systems use a combination of several cameras and lightning to take pictures or videos from several angles, afterward a software assembles those images and creates a three-dimensional model of a patient’s face or body. The airway volume was measured in CBCT in Dolphin Imaging (Version 11.8, Patterson Dental Supply, Chatsworth, Kalifornien) using an individual threshold as well as 73% as a standard threshold for airway recognition. We used 5 different volumes to correspond to the airway sections, respectively, pharyngeal levels (Figure 1, Supplementary Table 1). CBCT is a standard radiological imaging method in dentistry especially in implantology. This modality takes several x-rays and assembles them to a volume. Soft tissue was assessed in the three-dimensional photogrammetric images in 3dMD Vultus (Version 2.3.0.2, 3dMD, Atlanta, GA, USA) (Figures 2 and 3, Supplementary Table 2). Data was collected using Numbers (Version 10.2, Apple Inc. Cupertino, CA, USA). Differences, relative changes, and Dahlberg’s error were calculated using this software. A Dahlberg’s error of less than 2 mm, respectively, less than 2° was considered as clinically acceptable. A: Airway Landmarks according to Supplementary Table 1 used to construct Airway Boundaries in CBCT; B: Airway Boundaries for Determination of the Individual Threshold, Volume individual Threshold and Volume_73 (Supplementary Table 4); C: Airway Boundaries for Airway Volumes (Supplementary Table 4) A - Nasal Cavity (NC), B - Nasopharynx (NP), C - Oropharynx (OP), D - Hypopharynx (HP). Soft tissue landmarks (lateral and frontal view) according to Supplementary Table 2. Soft tissue landmarks (caudal view) according to Supplementary Table 2.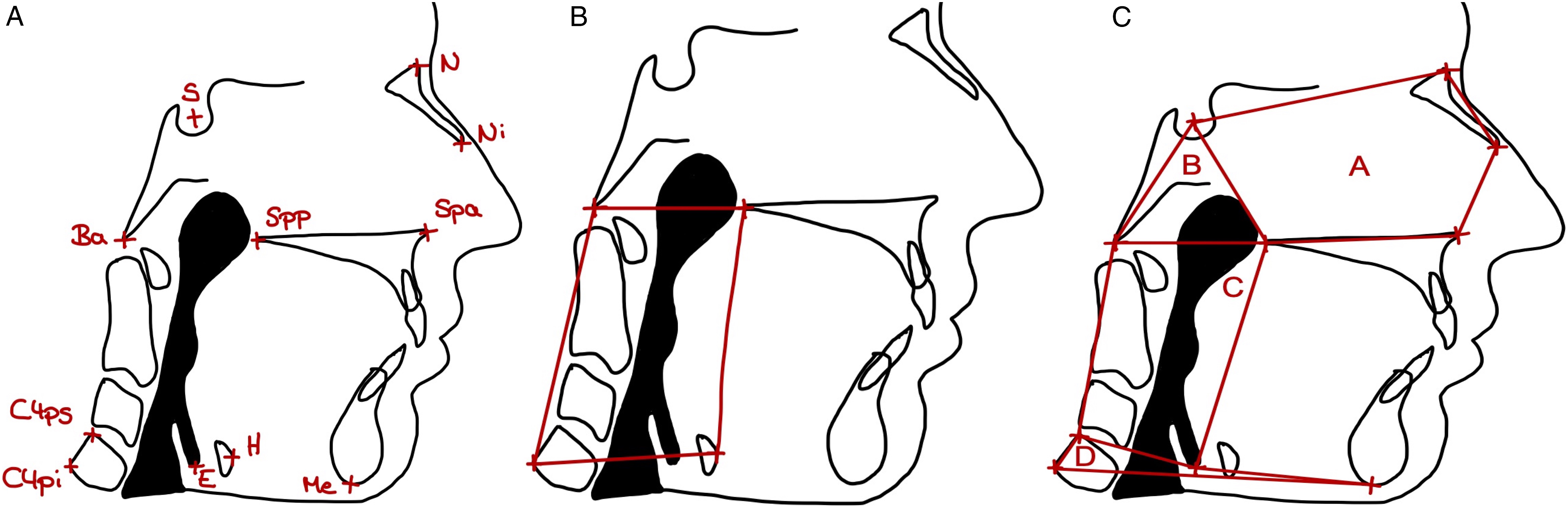
The statistical software SPSS Statistics for Mac (SPSS, Version 27.0, SPSS; IBM Corp. Armonk, NY, USA) was used to calculate mean, and standard deviation. Normally distributed variables were analyzed using Student’s t-tests. For other distributions, Wilcoxon signed-rank test was used. A value of P < .05 was considered significant.
Results
SARPE was performed on 10 patients with transverse maxillary hypoplasia. The mean follow-up time for CBCT was 230.2 days (min 110, max 497), 183.5 days (min 22, max 497) for photogrammetry. Dahlberg’s errors of soft tissue measurements were in the range of ±2 mm, respectively, ±2° except Anterior Nasal Base Angle, Posterior Nasal Base Angle, and Nasal Root Angle (Supplementary Table 3).
In this study, on the photorealistic model, nasal distances changed after SARPE. Significant soft tissue changes could be shown for: Nasomental Angle (P = .02), Anterior Nasal Base Angle (P < .01), Posterior Nasal Base Angle (P < .01), Nose Width (P = .01), Nostril Width, r (P < .01), Nostril Width, l (P = .02), and Nostril Length, l (P = .01) (Supplementary Table 3). Overall, a slight but mostly insignificant transverse widening of the nose could be shown: All mean absolute linear transverse changes were less than 2 mm—with the highest being Nose Width (1.76 mm). Nostril Width showed the highest relative widening (Nostril Width, r 15.54 ± 12.76%, Nostril Width, l 15.10 ± 17.41%). The mean absolute linear vertical change was always less than .55 mm, respectively, .92%. The mean absolute linear sagittal change never exceeded .62 mm, respectively, 2.97%. Similarly small changes were found for the angles in all 3 dimensions (Supplementary Table 3).
Significant airway changes could only be shown for the nasopharyngeal volume (Supplementary Table 4). Standard deviation was rather high for all volumes. The absolute change for all airway levels showed increase as well as decrease, except for the volume of nasopharynx (NP_Volume_73), that always slightly increased (1.55 ± .93 mL). The smallest diameter of Volume (Smallest Area_individual, Smallest Area_73) and OP_Volume (OP_Smallest Area_individual, OP_Smallest Area_73) showed high standard deviation as well.
Discussion
Though the SARPE is not a novel procedure, this study assessed postoperative change using a combination of new virtual three-dimensional imaging modalities. The results of this study showed that soft tissue and airway changes after SARPE can be displayed three-dimensionally via CBCT and stereophotogrammetry taken in daily outpatient practice. No additional images were needed. After SARPE nasopharyngeal volume increased and soft tissue parameters of the nose changed.
Surgically assisted rapid maxillary expansion (SARPE) is used for the treatment of transverse maxillary deficiency in mature patients. Studies of soft tissue changes after SARPE using stereophotogrammetry exist, but are limited to a few parameters.11,14 Although it has been shown that maxillary expansion can have positive effects on breathing and increases upper airway volume, only a few studies have used new three-dimensional methods to improve the understanding of SARPE effects on the airway. 12
Changes in the soft tissue nasal parameters were apparent. The present findings are in alignment with those of previous studies.10,15 The broadening of the soft tissue nose suggests, that patients with narrow nasal passages might benefit from SARPE due to a decrease in airway resistance, as already suggested in the literature. 16
After SARPE treatment, most airway volumes and areas showed changes; however, the volume increase was statistically significant only in the nasopharyngeal area. The highest relative changes were also found in that area. This corresponds with other studies of the airway after SARPE. 17 The changes in the other airway sections are consistent with earlier research on SARPE.5,6,18 The increase in airway volume and consecutive decrease in airway resistance indicate a positive effect of SARPE on patients with OSA as shown in earlier research. 5 Those patients might further benefit from the broadening of the nostrils which could be demonstrated in three-dimensional stereophotogrammetry.
Surgical treatment of OSA depends on the level of obstruction as the procedures aim to stabilize the upper airway in the area of obstruction. Choosing the most appropriate procedure is therefore an important part of sleep surgery. Every patient should be examined and evaluated in an interdisciplinary approach by dentistry, oral and maxillofacial surgery, ENT as well as internal medicine. If surgery is necessary, a thorough evaluation of the upper respiratory tract is required to select the best procedure. SARPE is recommended for obstructions of the nasal level or nasal cavity, while maxillomandibular advancement effects all levels of the upper airway. The latter is a rather long procedure followed by a downtime of several weeks, SARPE on the other hand, can be accomplished in less than 1 hour of general anesthesia and patients are able to return to work after 1 to 2 weeks. 13
The main limitation of this study is the small number of patients, which, together with the inconsistent time intervals between the images and CBCT scans, mean that it should be considered a pilot study. Further research should be conducted with larger collectives and consistent time intervals. In addition, the long-term effects on the airway and soft tissue after SARPE should be analyzed with three-dimensional methods. As this research focused on measuring changes after SARPE on young orthognathic patients with no comorbidities, there is only limited transferability to patients with sleep apnea who tend to be older and less healthy. Furthermore, this study did not use any patient reported outcome measures.
Besides the broadening of the maxillary arch, 2 aspects of SARPE effects should be kept in mind: First, patients with an obstructed nose may benefit from soft-tissue alteration by SARPE. Second, airway changes after SARPE might be helpful for patients with restriction in the nasopharyngeal area. Furthermore, this article proposes a standardized follow-up strategy in outpatient care, thereby eradicating any source of possible error, and herewith aiding the research. We recommend consistent time intervals after surgery as part of the follow-up strategy. We also suggest keeping SARPE in mind as a treatment option for OSAS patients with obstructions in the nasopharyngeal area. This study also shows that soft tissue changes can be found in the nasal area but are rarely significant. We suggest highlighting this insignificance of soft tissue changes in patient education, to avoid the fear of unwanted esthetic changes after SARPE.
Supplemental Material
Supplemental Material - Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT)
Supplemental Material for Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT) by Wiebke Heldmaier, Daniel Lonic, and Denys J. Loeffelbein in The American Surgeon
Supplemental Material
Supplemental Material - Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT)
Supplemental Material for Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT) by Wiebke Heldmaier, Daniel Lonic, and Denys J. Loeffelbein in The American Surgeon
Supplemental Material
Supplemental Material - Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT)
Supplemental Material for Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT) by Wiebke Heldmaier, Daniel Lonic, and Denys J. Loeffelbein in The American Surgeon
Supplemental Material
Supplemental Material - Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT)
Supplemental Material for Three-Dimensional Analyses of Postoperative Effects of Surgically Assisted Rapid Palatal Expansion (SARPE) on the Soft Tissue of the Midface Region and the Upper Airway Space using Stereophotogrammetry and Cone Beam Computed Tomography (CBCT) by Wiebke Heldmaier, Daniel Lonic, and Denys J. Loeffelbein in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.