
Abstract
Background
A gap remains in the role of neoadjuvant therapy for patients with ILC.
Method
Single-institution retrospective review of patients with ILC who received neoadjuvant therapy between 2008 and 2019.
Results
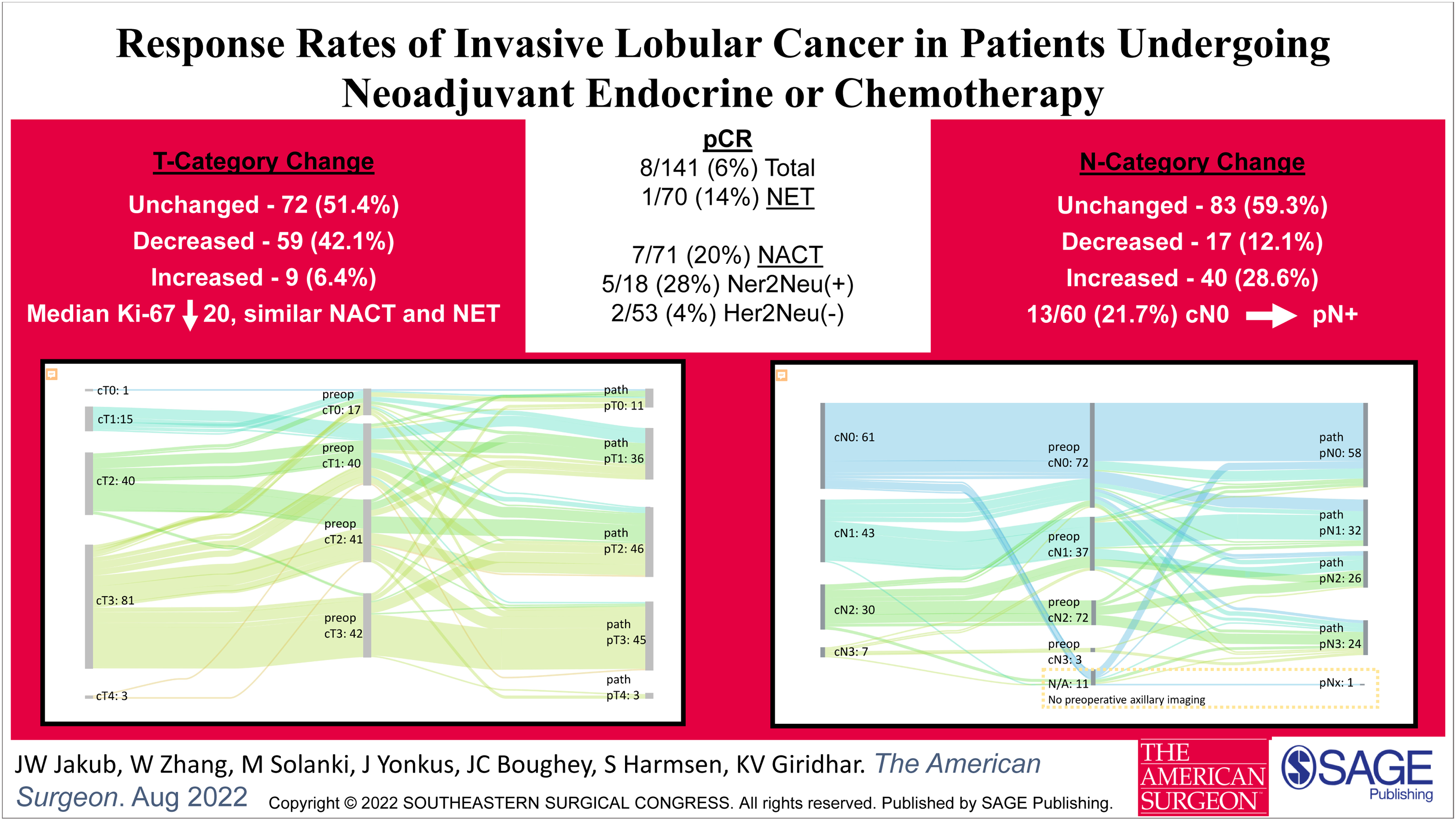
141 patients met inclusion criteria: 71 neoadjuvant chemotherapy (NACT) and 70 neoadjuvant endocrine therapy (NET). 7/71 (9.9%) patients had a pCR following NACT compared to 1/70 (1.4%) with NET (P = .063). pCR was observed in 5/18 (27.8%) patients with Her2Neu-positive disease following NACT, compared to 2/53 (3.8%) with Her2Neu-negative disease (P = .01).
For luminal B tumors, median Ki-67 decrease was similar following NACT and NET (18.3 vs 16.3, P = .26).
T category decreased in 59 (42.1%) patients following neoadjuvant therapy, increased in 9 (6.4%), and was unchanged in 72 (51.4%). More patients had an increase (28.6%) than decrease (12.1%) in their N category, including 13/60 (21.7%) who were clinically node-negative at diagnosis and identified to have node-positive disease following neoadjuvant therapy, at definitive surgery.
Conclusion
In Her2Neu-negative ILC, the potential of a pCR with NACT or NET is low. Most patients’ nodal status and tumor size remain unchanged. There is a potential for pathologic stage to be higher at surgery compared to the clinical stage prior to neoadjuvant therapy.
Get full access to this article
View all access options for this article.