
Abstract
Background
Race is associated with differences in quality of care process measures and incidence of venous thromboembolism (VTE) in trauma patients. We aimed to investigate if racial disparities exist in the administration of VTE prophylaxis in trauma patients.
Methods
We queried the Trauma Quality Improvement Project database from 2017 to 2019. Patients ages ≥16 years old with ISS ≥15 were included. Patients with no signs of life on arrival, any AIS ≥6, hospital length of stay <1 day, anticoagulant use before admission, or without recorded race were excluded. Patients were grouped by race: white, black, Asian, American Indian, and Native Hawaiian or Pacific Islander. The association between VTE prophylaxis administration and race was determined using a Poisson regression model with robust standard errors to adjust for confounders.
Results
A total of 285,341 patients were included. Black patients had the highest rates of VTE prophylaxis exposure (73.8%), shortest time to administration (1.6 days), and highest use of low molecular weight heparin (56%). Black patients also had the highest incidence of deep vein thrombosis (2.8%) and pulmonary embolism (1.4%). Black patients were 4% more likely to receive VTE prophylaxis than white patients [adj. IRR (95% CI): 1.04 (1.03-1.05), P < .001]. American Indians were 8% less likely to receive VTE prophylaxis [adj. IRR (95% CI): .92 (.88-.97), P < .001] than white patients. No differences between white and Asian or Native Hawaiian or Pacific Islander patients existed.
Discussion
While black patients had the highest incidence of DVT and PE, they had higher administration rates and earlier initiation of VTE prophylaxis. Further work can elucidate modifiable causes of these differences.
Key Takeaways
• Race is associated with differences in quality of care process measures and incidence of venous thromboembolism in trauma patients. • Black patients had the highest incidence of deep vein thrombosis and pulmonary embolism despite having a higher administration rate and earlier initiation of venous thromboembolism prophylaxis.
Introduction
Venous thromboembolism (VTE), which includes both deep venous thrombosis (DVT) and pulmonary embolism (PE), is a major source of both morbidity and mortality in injured patients.1-4 The reported incidence of VTE in trauma patients ranges from 7 to 60%.3,5 Pulmonary embolism is the third most common cause of death in trauma patients who survive the first 24 hours and is a potentially preventable complication.6,7 In addition, a delay in the administration of VTE chemoprophylaxis is also a known risk factor for development of VTE. For these reasons, timely and appropriate initiation of chemical VTE prophylaxis is essential. The Agency for Healthcare Research and Quality has recognized VTE prophylaxis administration as a top patient safety practice and national organizations, including the Western Trauma Association and the American Association for the Surgery of Trauma, have guidelines recommending initiation of VTE chemoprophylaxis within the first 24 hours of injury if no absolute contraindication exists.7-12 Time to administration of VTE prophylaxis and rates of VTE prophylaxis are also important quality process of care measures that provide benchmarks for trauma centers as part of the Trauma Quality Improvement Project. 13
While all trauma patients are at elevated risk for developing VTE, prior studies have found differences in the incidence of VTE in trauma patients across racial groups. 14 Similar findings have been reported in non-injured patients.14,15 White et al found that black patients have a 40% higher incidence of VTE and higher proportions of PE, while Asian patients had a significantly lower incidence of VTE when compared to white patients. 15
Proposed reasons behind these racial disparities in the incidence of VTE are multifactorial and previous studies have focused on differences in risk factors, such as insurance status, comorbidities, access to care, setting of care, socioeconomic status, and practice variation.16-19 Many of these studies are small or focus on differences specifically in outcomes and not in quality process measures. The aim of this study is to determine if racial disparities exist in the initiation and administration of VTE chemoprophylaxis in critically ill trauma patients across different races. The authors hypothesize that there are disparities in initiation and administration of VTE chemoprophylaxis.
Methods
The need for ethical approval by an institutional review board was waived as it only uses de-identified aggregate data. The American College of Surgeons Trauma Quality Improvement Program (TQIP) database was queried for all patients 16 years or older treated at a trauma center between 2017 and 2019 with an injury severity score (ISS) ≥ 15. Patients with minor or moderate injuries were not included in the current study since these patients generally do not require VTE prophylaxis. Patients without signs of life on arrival in the emergency department (ED), any abbreviated injury severity score (AIS) of 6, or hospital length of stay (LOS) less than 1 day were excluded. Patients who were mixed race, unspecified race, had missing race data, or receiving anticoagulation prior to admission were also excluded. Variables collected included race, age, sex, initial vitals on admission to the ED, AIS scores, comorbidities, mechanism of injury, the presence of an advanced directive limiting care, primary intervention performed for hemorrhage control, trauma center level, insurance type, hospital type, VTE prophylaxis (low molecular weight heparin or heparin), hospital LOS, discharge disposition, and complications. The primary outcome was the administration of VTE prophylaxis.
This study complies with both the Declaration of Helsinki, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines and published recommendations for the study of race, ethnicity, sex, and gender.20-22 The categories for “race” used in this study are the same utilized in TQIP, based on the 2010 US Census Bureau.
Statistical Analysis
Patients were split into groups based on their race: white, black, Asian, American Indian, and Native Hawaiian or Pacific Islander. Differences between continuous variables were analyzed using an analysis of variance (ANOVA) and summarized as means and standard deviations (SDs) if they were normally distributed. Otherwise, the Kruskal-Wallis test along with the median and interquartile range (IQR) was used. Categorical variables were presented as counts and percentages, while the statistical significance of differences between categorical variables was determined using a chi-square test or Fisher’s exact test.
A Poisson regression model with robust standard errors was used to determine the association between VTE prophylaxis and race. VTE prophylaxis was used as the outcome in the model. Explanatory variables consisted of demographic data (race, age, and sex), the highest AIS in each region, comorbidities, advanced directives limiting care, trauma type, the type surgery performed for hemorrhage control, payment method, trauma center level, and hospital type. Results are presented as incident rate rations (IRRs) and 95% confidence intervals (CIs). Missing values were managed using multiple imputations by chained equations.
Analyses were performed using the statistical programming language R (R Foundation for Statistical Computing, Vienna, Austria). 23 Statistical significance was defined as a two-sided P-value less than .05.
Results
Demographics and Clinical Characteristics Among Trauma Patients.
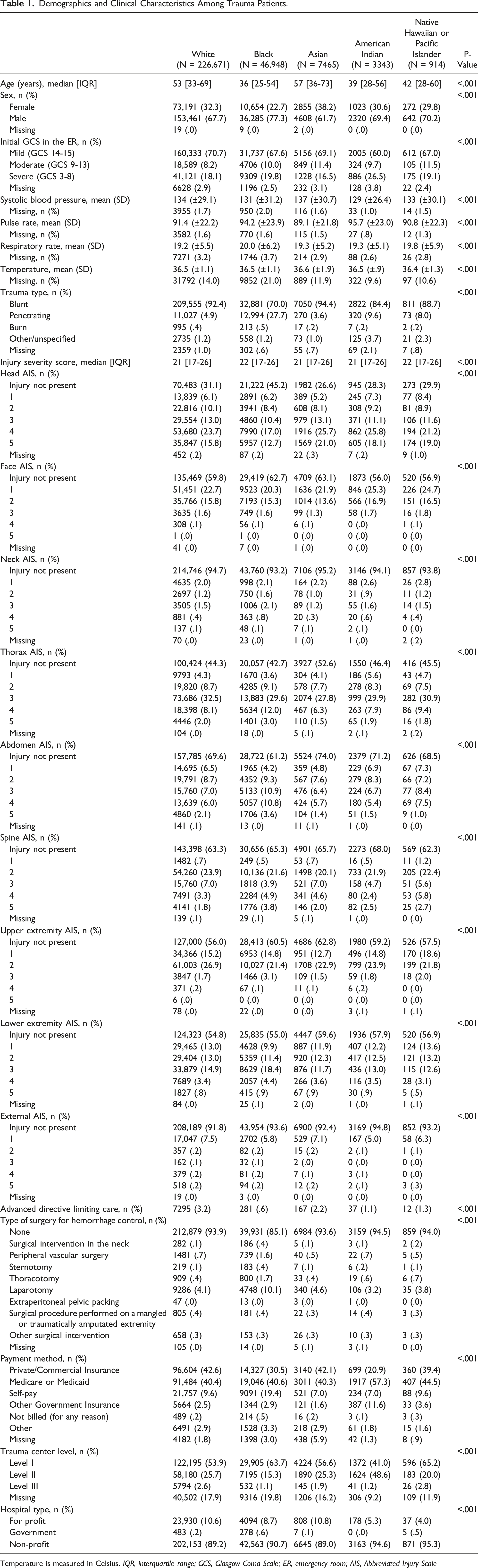
Temperature is measured in Celsius. IQR, interquartile range; GCS, Glasgow Coma Scale; ER, emergency room; AIS, Abbreviated Injury Scale
Comorbidities Among Trauma Patients.
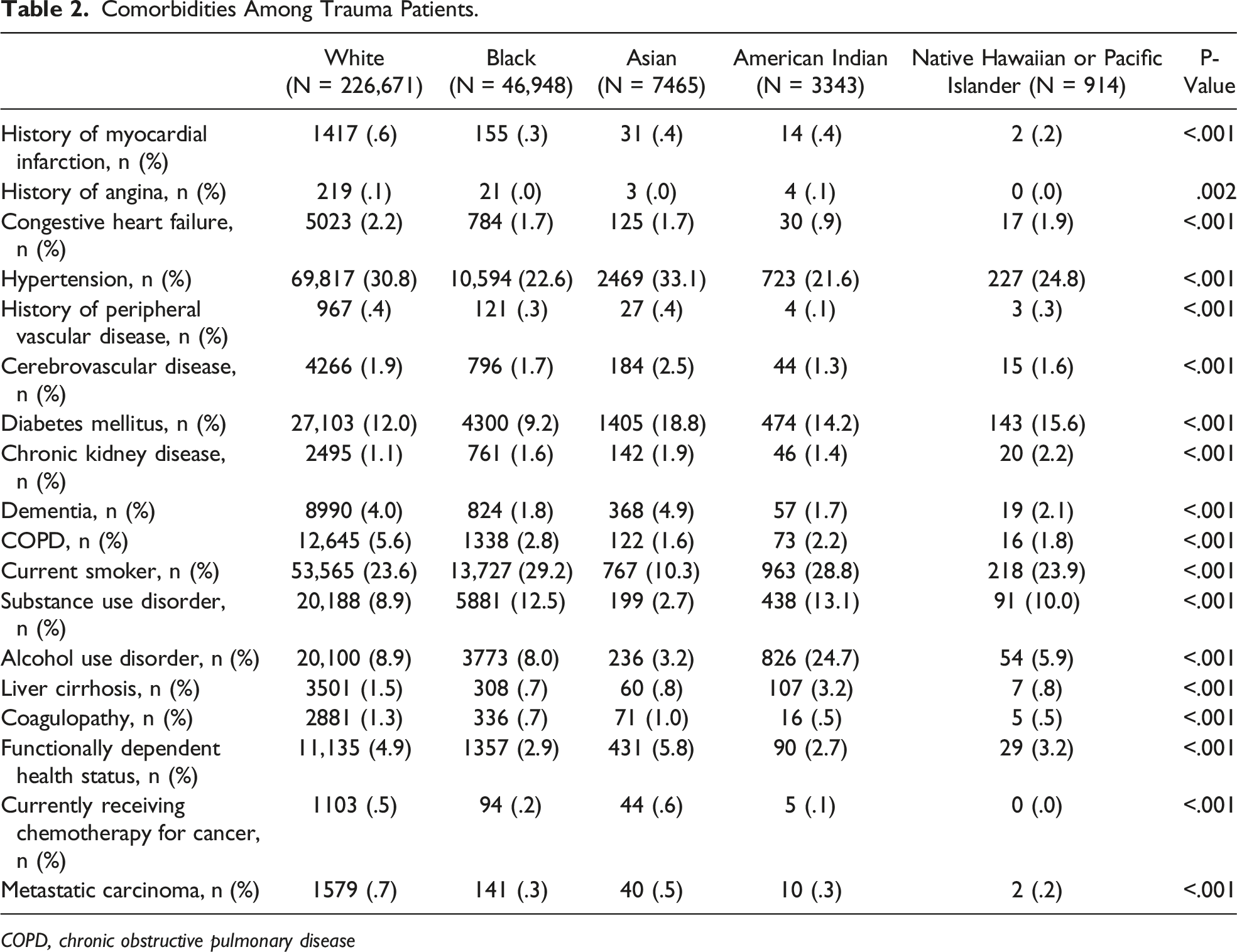
COPD, chronic obstructive pulmonary disease
Crude Outcomes Among Trauma Patients.
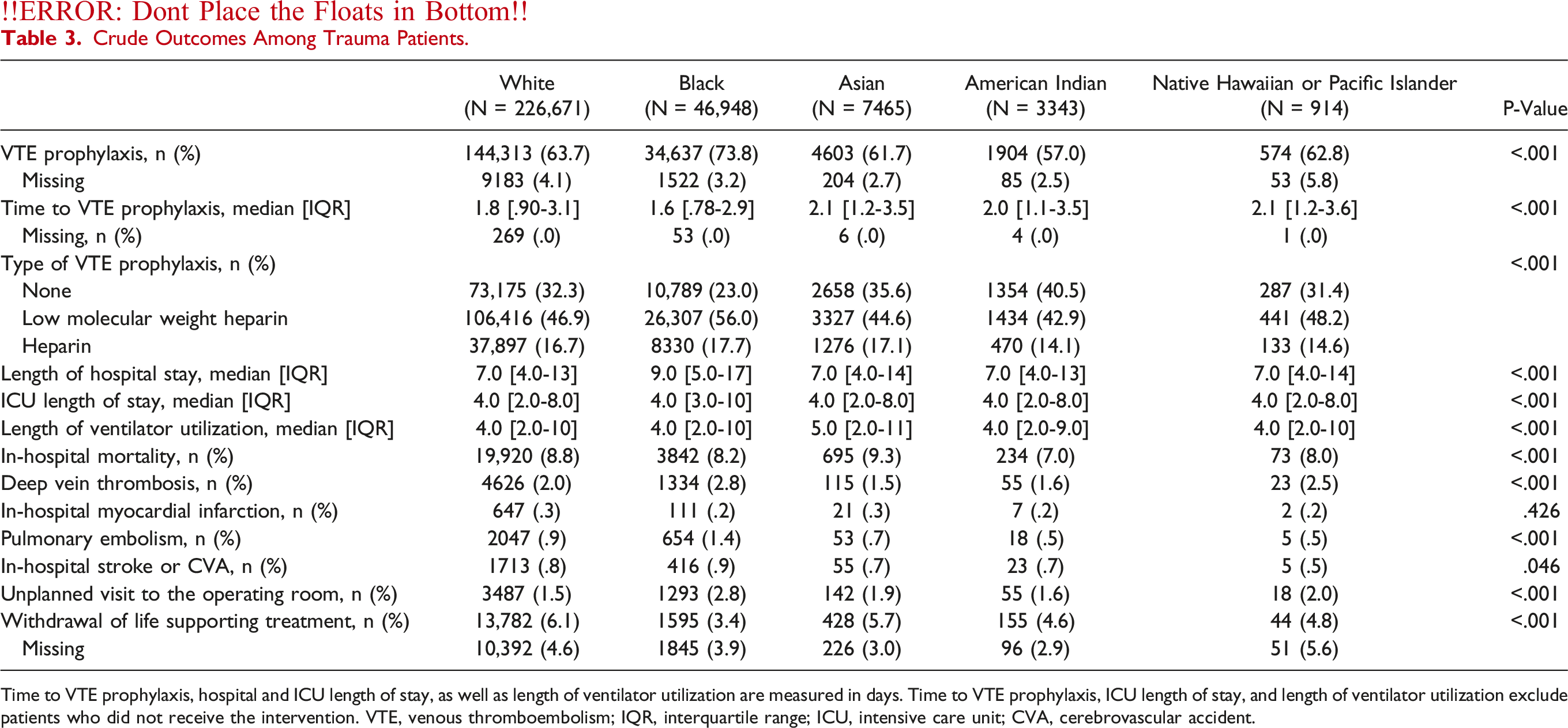
Time to VTE prophylaxis, hospital and ICU length of stay, as well as length of ventilator utilization are measured in days. Time to VTE prophylaxis, ICU length of stay, and length of ventilator utilization exclude patients who did not receive the intervention. VTE, venous thromboembolism; IQR, interquartile range; ICU, intensive care unit; CVA, cerebrovascular accident.
Incidence Rate Ratios for VTE Prophylaxis in Trauma Patients.
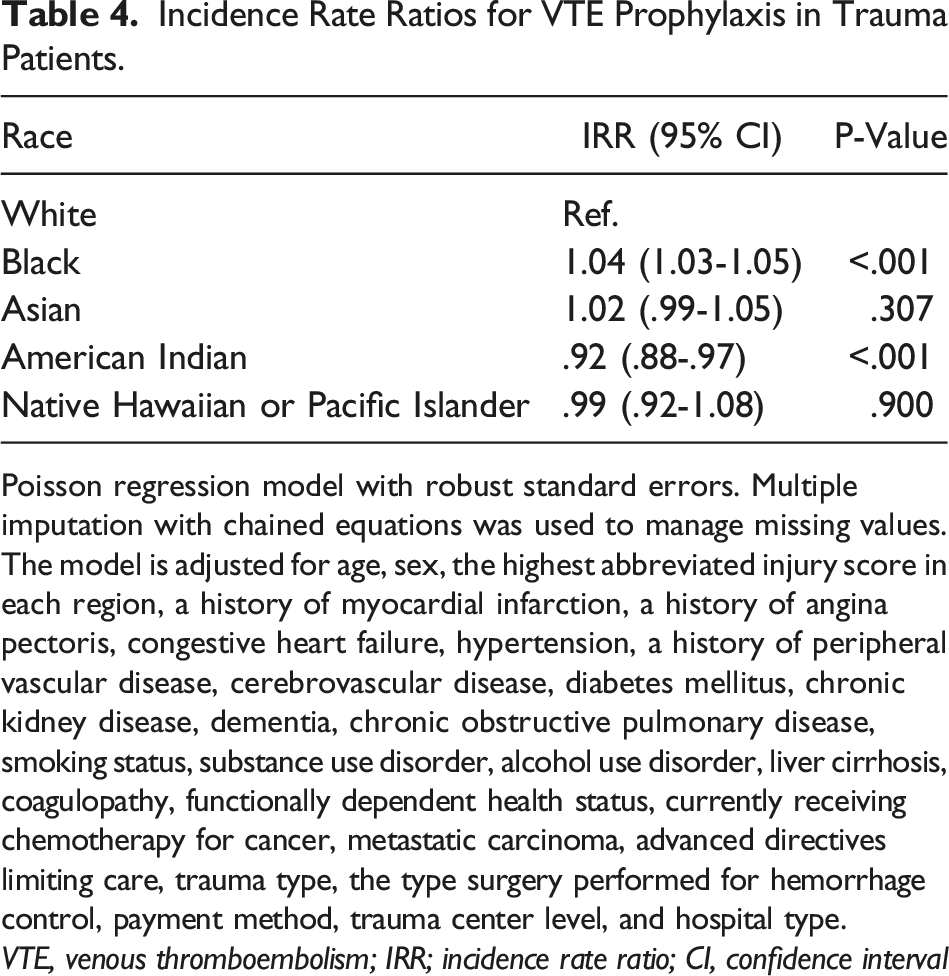
Poisson regression model with robust standard errors. Multiple imputation with chained equations was used to manage missing values. The model is adjusted for age, sex, the highest abbreviated injury score in each region, a history of myocardial infarction, a history of angina pectoris, congestive heart failure, hypertension, a history of peripheral vascular disease, cerebrovascular disease, diabetes mellitus, chronic kidney disease, dementia, chronic obstructive pulmonary disease, smoking status, substance use disorder, alcohol use disorder, liver cirrhosis, coagulopathy, functionally dependent health status, currently receiving chemotherapy for cancer, metastatic carcinoma, advanced directives limiting care, trauma type, the type surgery performed for hemorrhage control, payment method, trauma center level, and hospital type.VTE, venous thromboembolism; IRR; incidence rate ratio; CI, confidence interval
Discussion
VTE continues to be a major source of morbidity and mortality for hospitalized trauma patients. VTE is also known to affect certain racial groups disproportionally. In this retrospective review, our results demonstrate a racial disparity in practices of VTE chemoprophylaxis administration. There were statistically significant differences between racial groups in rates of VTE administration, median time to initiation, and the types of VTE prophylaxis administered. When controlling for available confounding variables, we also found differences in the overall likelihood of receiving VTE chemoprophylaxis during hospitalization. Black patients had the highest rates of administration and the shortest time to initiation, yet still had the highest rates of PE and DVT compared to the other racial groups. On the other hand, American Indian patients were found to be less likely to receive VTE prophylaxis than white patients. VTE are potentially preventable complications, and these findings further demonstrate the importance of identifying areas of improvement so that all patients receive equitable care.
The current study provides further evidence of the extent of racial disparities in this quality measure which can be used to justify large-scale implementation of strategies to limit the impact of these disparities. Prior studies have shown that a standardized approach to VTE prophylaxis administration can significantly reduce VTE rates.24-26 Haut et al also showed that implementation of a computer-based VTE protocol can help reduce disparities.25,27 The persistence in these disparities across race, even in the era of electronic medical records and computerized physician tools, suggests that additional proactive efforts are needed. Nevertheless, the potential to bypass these prompts introduces the possibility of provider bias. Providers at all levels of training have been shown to alter clinical decision making based on implicit biases.28-31 This is especially important in trauma patients where the nuances of administering VTE prophylaxis may be more complex. Our results add to the scientific discourse advocating for proactive safeguards against implicit bias in medicine.
A growing body of literature has shown the importance of recognizing racial disparities in quality process measures. 32 In obstetrics, Dwyer et al found racial differences in a variety of quality measures, such as use of antenatal steroids, timely treatment of severe hypertension, and use of prophylactic antibiotics. 33 Prior studies looking at administration rates of VTE prophylaxis among hospitalized medical patients report rates of 43.3 to 56.7%. 34 In a single institution study examining rates of administered VTE prophylaxis in black and white hospitalized trauma patients, Lau et al found that black patients were prescribed appropriate VTE prophylaxis at higher rates (70.1%) than white patients (56.6%) (P = .025). 27 Guidelines for preventing hospital-associated venous thromboembolism across all medical specialties have included increased computerized order support systems to ensure appropriate administration.35,36 However, in trauma patients, the decision regarding when to start VTE prophylaxis is often more nuanced given the concern for hemorrhage. Factors such as the presence of traumatic brain injury and possibility for ongoing or delayed hemorrhage may complicate the decision process, resulting in administration delays.17,37,38
The current investigation including severely injured patients found that black patients had higher rates of VTE prophylaxis administration (73.8%) compared to white patients (63.7%) (P < .001). However, the results identified disparities in quality process measures by including VTE prophylaxis rates among Asian (61.7%) and Native Hawaiian or Pacific Islander patients (62.8%). The rates in these populations were similar to those seen in white patients and also American Indian patients who had the lowest rate overall (57%) (P < .001). Our study also goes a step beyond by incorporating a variety of clinical, physiological, and patient-specific variables to identify the incidence rate ratio for receiving VTE prophylaxis in this population during hospitalization. This analysis showed that black patients were more likely to receive VTE prophylaxis compared to white patients [1.04 (1.03-1.05), P < .001], while American Indian patients were less likely to receive such prophylaxis [.92, (.88-.97), P < .001].
Reasons for differences in rates of VTE prophylaxis administration are not clear. Across nearly every evidence-based VTE chemoprophylaxis administrative quality metric, black patients had better processes of care. These include the highest likelihood to receive chemical VTE prophylaxis, the highest percentage of patients and having the shortest time to administration (median [IQR]: 1.6 [.78-2.9] days, P < .001), and the highest percentage of patients receiving low molecular weight heparin (LMWH) (56%, P < .001). However, black patients still had the highest incidence of VTE among the five racial cohorts (PE: 1.4% and 2.8%, P < .001). This calls for studies investigating other modifiable risk factors beyond exposure and timing for initiation of VTE prophylaxis, in addition to race, in severely injured patients. In their TQIP review, Knudson et al found that ventilator days and major surgical procedure had the highest odds ratio for VTE following trauma. 5 Although ICU length of stay and length of ventilator utilization did not differ significantly between races, black patients did have the highest rates of surgical intervention for hemorrhage control (14.9%), including laparotomy (10%), thoracotomy (1.7%), and peripheral vascular surgery (1.6%) (P < .001). These patients were therefore already at higher risk of VTE based on mechanism and need for intervention. Haut et al reported a rate of VTE prophylaxis administration of 66.2% that was able to be increased to 84.4% after implementing a clinical decision support system. 25 Our study, in conjunction with the others above, demonstrates the need for additional guidelines for the administration of VTE prophylaxis to ensure appropriate dosing for patients at elevated risk of VTE complications.
The strength of this study comes from the robust TQIP database and represents one of the largest studies analyzing disparities in the administration of VTE chemoprophylaxis. However, this study does have several limitations that the authors acknowledge. It is a retrospective review of a large national database and is subject to those inherent limitations. Further, these data are prior to the first amendment demonstrations of 2020 that increased attention on racial disparities in the United States, including in health care. These dates were chosen as they are the most recent 3 years of data available. Another limitation of the study is the distinction between race and ethnicity. While we were able to include a significant number of patients from each racial category, we did not include the ethnicity categories of Hispanic or Latino. Therefore, we were not able to identify if additional differences in care exist for this significant patient population. Hispanic or Latino patients may identify as any race; however, approximately half view themselves as white. 39 As this was our reference cohort, this must be taken into consideration when interpreting the results. While we attempted to control for typical reasons why VTE prophylaxis may be delayed, including TBI, coagulopathy, and need for surgical control of hemorrhage, there are circumstances that may not be captured by the database. 36 TQIP also does not include data points on the presence of institutional protocols to ensure timely administration. The database also only includes LMWH and heparin so other VTE prophylaxis options are missed. It is also not known how the anticoagulants were dosed and if the dosing was appropriate or achieved therapeutic levels at individual level. We were also not able to determine how many of VTE were clinically significant, which has been estimated to be <1%. 5 We were also not able to control for how the VTE events were diagnosed or account for institutional policies regarding DVT screening.
Conclusion
There are disparities in the initial administration and timing of initiation of VTE chemoprophylaxis based on patients’ race. While black patients had the highest incidence of DVT and PE, they also had a higher incidence of administration and earlier initiation of VTE prophylaxis. Further studies are needed to elucidate modifiable causes of these differences in order to deliver just and equitable care.
Footnotes
Author Contributions
JAZ: study design, data acquisition, analysis and interpretation of data, drafting, and revision of manuscript. MPF: analysis and interpretation of data, drafting, and revision of manuscript. GAB: interpretation of data, drafting, and revision of manuscript. YC: analysis and interpretation of data, and revision of manuscript. MTQ: interpretation of data, drafting, and revision of manuscript. BS: study design, data acquisition, interpretation of data, drafting, and revision of manuscript. SM: study design, analysis and interpretation of data, drafting, and revision of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The abstract of this paper has been accepted for a poster presentation at the 81st Annual Meeting of AAST and Clinical Congress of Acute Care Surgery to be held in Chicago, Illinois on September 21-24, 2022.