Large bowel obstructions (LBO) often present as surgical emergencies in the setting of a mechanical obstruction. Sometimes, however, the decision to operate is not straightforward. With an aging population, more patients are presenting with comorbidities that can be prohibitive to general anesthesia. Considering that colorectal emergencies are common, novel approaches are necessary to mitigate the morbidity and mortality risk for general anesthesia and surgery.
Regional blocks and sedation are frequently used for a variety of procedures to minimize postoperative pain and general anesthetic risk. Within colorectal surgery, there have been reports of epidurals for awake colectomies.1 However, the risk of hypotension with epidural anesthesia can be prohibitive for patients with severe cardiovascular comorbidities. As an alternative to general anesthesia and epidural anesthesia, we utilized ultrasound-guided transversus abdominis plane (TAP) and rectus sheath (RS) blocks to perform awake colostomies in three patients with LBO requiring emergent diversion. Block details and short-term patient outcomes for all cases are summarized in Table 1.
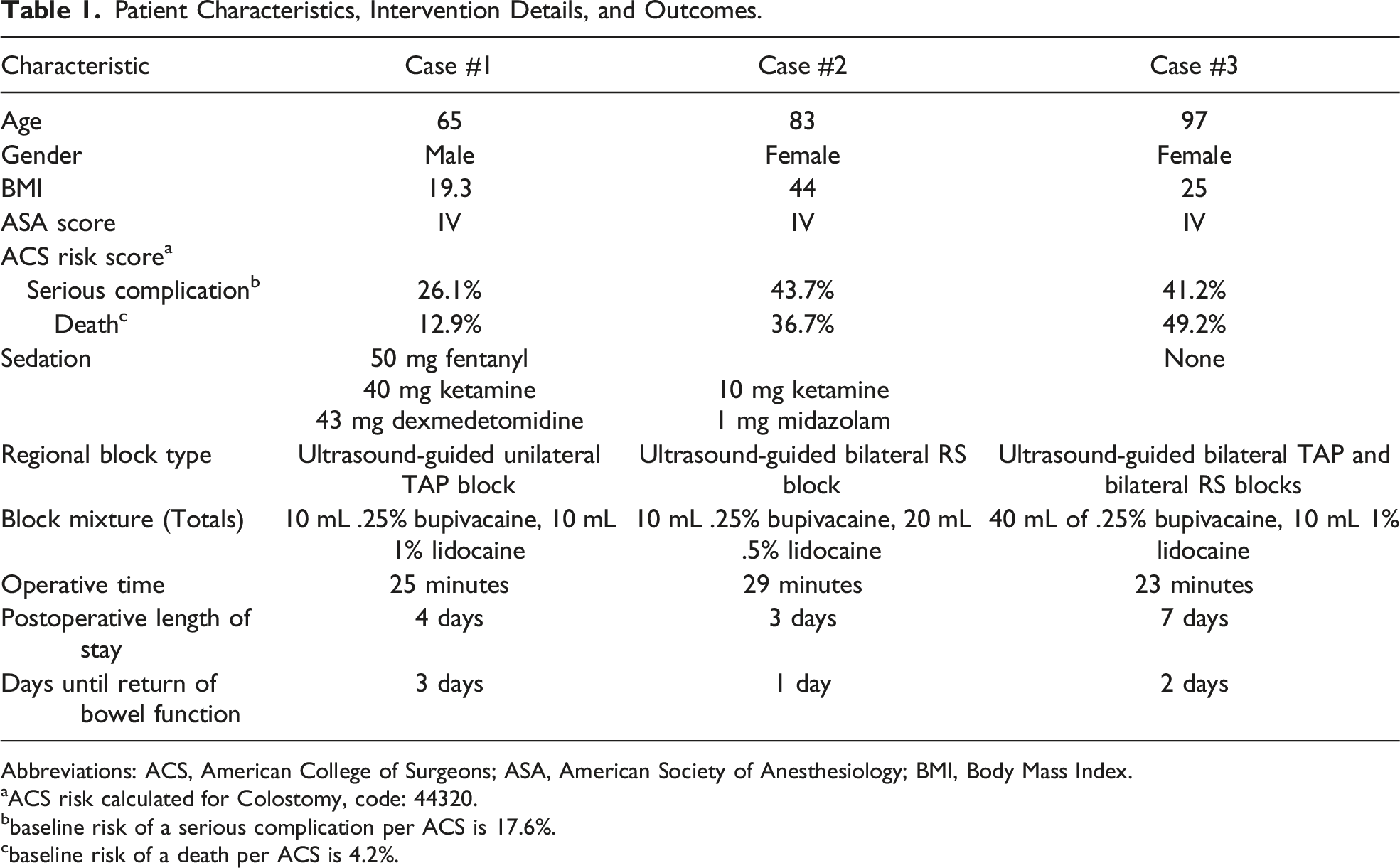
Patient Characteristics, Intervention Details, and Outcomes.
Ultrasound-guided bilateral TAP and bilateral RS blocks
Block mixture (Totals)
10 mL .25% bupivacaine, 10 mL 1% lidocaine
10 mL .25% bupivacaine, 20 mL .5% lidocaine
40 mL of .25% bupivacaine, 10 mL 1% lidocaine
Operative time
25 minutes
29 minutes
23 minutes
Postoperative length of stay
4 days
3 days
7 days
Days until return of bowel function
3 days
1 day
2 days
Abbreviations: ACS, American College of Surgeons; ASA, American Society of Anesthesiology; BMI, Body Mass Index.
aACS risk calculated for Colostomy, code: 44320.
bbaseline risk of a serious complication per ACS is 17.6%.
cbaseline risk of a death per ACS is 4.2%.
Case 1: A 65-year-old male with no prior surgical history and a medical history significant for severe chronic obstructive pulmonary disease (COPD) requiring home oxygen, stage IIA lung cancer, stroke, and pulmonary embolism presented to the emergency department with a 1-day history of severe left lower quadrant abdominal pain. Workup revealed a diverticular stricture causing complete obstruction. Due to the large bowel obstruction and concern for bowel perforation, a diversion was indicated. However, given the patient’s comorbidities, the risks of general anesthesia outweighed the benefits of surgery. Therefore, in discussion the anesthesiology team, it was decided that patient would benefit from diversion under regional anesthesia. Via ultrasound guidance, the plane between the internal oblique and transversus abdominis muscles was identified and a unilateral, left-sided TAP block was performed by the anesthesiology team. Ketamine infusion was used for sedation and a total of 50 mcg of fentanyl were used for analgesia. A total of 17 mL of 1% Lidocaine with epinephrine were used at the incision site. A disc of skin and subcutaneous tissue was removed from the left upper quadrant. A longitudinal fasciotomy on the anterior and posterior rectus sheath was made. The omentum was identified and reflected cephalad. Transverse colon was identified and, with gentle manipulation, delivered through the fascial defect. A transverse colotomy was made and a loop colostomy was matured in a Brooke fashion. The patient tolerated the procedure well with no perioperative complications.
Case 2: An 83-year-old female with a prior surgical history of appendectomy and a medical history of diverticular disease, congestive heart failure, COPD, severe aortic stenosis, hypertension, and obstructive sleep apnea presented with a 2-day history of nausea and vomiting. CT scan demonstrated a sigmoid obstruction secondary to a diverticular stricture. Due to a large bowel obstruction and multiple, severe comorbidities, she underwent an awake diverting transverse loop colostomy. In the operating room, the anesthesiologist performed ultrasound-guided bilateral RS blocks by injecting a lidocaine/bupivacaine mixture in the space between the rectus abdominis muscle and posterior rectus sheath. Ketamine and midazolam were also administered intravenously for sedation. Patient did not require further intravenous analgesia. At the incision site, 69 mL of .25% bupivacaine mixed with 1% lidocaine (70/30 ratio) were used. Operation was performed as previously mentioned. Patient’s peri-operative course was uncomplicated.
Case 3: A 97-year-old female with no past surgical history and a past medical history significant for congestive heart failure, atrial fibrillation, diverticulosis, stage III chronic kidney disease, and recent stroke presented with profuse diarrhea. CT of the abdomen and pelvis revealed dilation of her large bowel with transition in the sigmoid colon along with distention of the small bowel. Due to her multiple comorbidities and recent stroke history, she was unlikely to tolerate general anesthesia without a major morbidity or mortality. An attempt was made preoperatively to endoscopically stent the stricture; however, the procedure was aborted secondary to bowel tortuosity and poor visualization. Bilateral TAP blocks and RS blocks were performed via ultrasound guidance by the anesthesia team prior to the start of the operation. A total of 2.5 mL of 1% lidocaine with 10 mL of .25% bupivacaine were injected per block. A transverse loop colostomy was constructed as previously mentioned. No additional intravenous analgesic or sedating agents were utilized. The patient tolerated the procedure well without acute peri-operative complications and did not require any conscious sedation during the operation.
Three awake colostomies were performed under regional analgesia by the same fellowship-trained colorectal surgeon at our institution from 2020 to 2021. All three patients achieved regional anesthesia with TAP or RS blocks. Various degrees of conscious sedation were achieved with ketamine and midazolam when necessary. All surgeries were performed in under 30 minutes. All patients were discharged 4-7 days later with an average length of stay of 4.7 days. Using the American College of Surgeons surgical risk calculator for colostomy (CPT code 44320), patients had perioperative risks of serious complications ranging from 26% to 43.7% and risk of death ranging from 12.9% to 49.2%. These patients were at an elevated risk of morbidity and mortality as the average patient risk for this same procedure is approximately 17% for serious complications and 4% for death.
Although the approach to postoperative pain control is often multimodal, regional anesthesia gained in popularity in peri- and postoperative pain management because of advances in ultrasound guidance and ability to visualize the planes, nerves, and vasculature. Truncal blocks, such as TAP and RS blocks, reduce postoperative pain scores and narcotic usage in abdominal and gynecological surgeries.2 Although commonly used as alternative to general anesthesia in extremity surgeries, there is paucity of reports that utilize these field blocks as a complete alternative to general anesthesia for intra-abdominal surgery.
Other alternatives to general anesthesia for colorectal surgeries have been previously discussed. Local anesthesia, in conjunction with intravenous fentanyl, was used in a case series of 8 patients for colon cancer resections via low midline or transverse abdominal or lower midline incisions.4 Although they initially had comorbidities prohibitive of general anesthesia, the patients had acceptable postoperative outcomes after colonic resection under local anesthesia. By the same token, in a case series of 17 patients, local anesthesia was successfully used as an alternative to general anesthesia for ileostomy closure.3 Although neither of those approaches utilize truncal abdominal blocks, they serve as further proof of feasibility and efficacy of alternatives to general anesthesia.
In rare instances, where the risks of general anesthesia outweigh the benefits of surgery, it is important that surgeons consider other anesthetic options such as regional and local anesthesia for bowel diversion. For abdominal procedures, a TAP or RS block can be very effective alternatives to general anesthesia with acceptable postoperative outcomes. Careful discussion with the patients regarding peri- and postoperative expectations is paramount to the success of the procedure. Importantly, these interventions and successful outcomes necessitate the orchestrated efforts of the entire operative team and explicit communication and collaboration between all parties involved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Marc M. Mankarious
References
1.
KoltunWAMcKennaKJRungG. Awake epidural anesthesia is effective and safe in the high-risk colectomy patient. Dis Colon Rectum. 1994;37(12):1236-1241. doi:10.1007/BF02257788
2.
SviggumHPNiesenADSitesBDDilgerJA. Trunk blocks 101: Transversus abdominis plane, ilioinguinal-iliohypogastric, and rectus sheath blocks. Int Anesthesiol Clin. 2012;50(1):74-92. doi:10.1097/AIA.0b013e31823bc2eb
3.
HaagmansMJBrinkertWBleichrodtRPvan GoorHBremersAJ. Short-term outcome of loop ileostomy closure under local anesthesia: Results of a feasibility study. Dis Colon Rectum. 2004;47(11):1930-1933. doi:10.1007/s10350-004-0686-9
4.
SebastianJSranHMarzoukD. Is radical bowel cancer resection under local anaesthesia and sedation feasible?Indian J Surg. 2015;77(4):260-264. doi:10.1007/s12262-015-1281-0